How to take proper history of. Shortness of breath mbbs 4th yr medicine
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have excellent material from multiple authoritative textbooks. Let me compile a comprehensive, well-structured answer for an MBBS 4th year student.
History Taking for Shortness of Breath (Dyspnea) - MBBS 4th Year Medicine
Dyspnea is defined as a subjective sensation of difficult, labored, or unpleasant breathing. History is the single most important component of the evaluation - no test replaces it.
1. Presenting Complaint
State it clearly: "Patient complains of shortness of breath / breathlessness / difficulty in breathing."
2. History of Presenting Complaint (HOPI)
A. ONSET
| Feature | Clinical Clue |
|---|---|
| Sudden (seconds to minutes) | Pneumothorax, PE, acute MI, foreign body, anaphylaxis, arrhythmia |
| Acute (hours to days) | Pneumonia, acute heart failure, pulmonary edema, asthma exacerbation |
| Subacute (days to weeks) | Pleural effusion, slowly progressing HF |
| Chronic / Insidious (months to years) | COPD, ILD, anemia, cardiac valvular disease, malignancy |
B. DURATION
- How long has it been present?
- Is it the first episode or recurrent?
C. PROGRESSION
- Getting worse, better, or same?
- Constant or episodic?
- Diurnal variation? (Worse at night = asthma/HF; worse in morning = COPD)
D. SEVERITY
Ask the patient to quantify using:
- MRC Dyspnea Scale (Grades 1-5):
- Grade 1: Only on strenuous exertion
- Grade 2: Walking on incline or hurrying on level
- Grade 3: Walks slower than peers on level / stops after ~100 m
- Grade 4: Too breathless to leave the house
- Grade 5: Breathless on dressing/undressing or at rest
- Compare functional capacity: "How many stairs can you climb? How far can you walk?"
E. CHARACTER / QUALITY
Ask the patient to describe the sensation:
- Air hunger / suffocation (often cardiac or metabolic)
- Chest tightness (asthma, COPD, ACS)
- Inability to take a deep breath (hyperventilation, pleuritis)
- Increased effort / heavy breathing (respiratory muscle weakness, COPD)
F. POSITIONAL FACTORS (very important for 4th year!)
| Symptom | Definition | Suggests |
|---|---|---|
| Orthopnea | Dyspnea on lying flat; ask number of pillows needed | Left heart failure (pulmonary congestion worsens with recumbency) |
| PND (Paroxysmal Nocturnal Dyspnea) | Wakes patient from sleep ~1-2 hrs after lying down; relieved by sitting/standing | Severe left heart failure |
| Bendopnea | Breathlessness while bending forward (e.g., tying shoelaces) | Advanced HF with elevated filling pressures |
| Platypnea | Worse when upright, better when lying down | Hepatopulmonary syndrome, ASD (rare) |
| Trepopnea | Worse lying on one side | Large pleural effusion (worse on affected side), unilateral lung disease |
G. AGGRAVATING AND RELIEVING FACTORS
- Exercise, cold air, dust/smoke (asthma/COPD)
- Seasonal or allergic triggers (asthma)
- Improvement with rest (cardiac causes)
- Improvement with bronchodilators (obstructive airway disease)
- Improvement over weekends vs. weekdays (occupational lung disease)
H. ASSOCIATED SYMPTOMS (pivotal for differential diagnosis)
Respiratory system:
- Cough - productive (pneumonia, bronchiectasis, HF - "pink frothy"), dry (ILD, ACE inhibitor)
- Sputum - color, amount, hemoptysis (PE, TB, cancer, bronchiectasis)
- Wheeze - heard by patient? (asthma, COPD, cardiac asthma)
- Stridor - inspiratory noise (upper airway obstruction)
- Pleuritic chest pain - sharp, worse on breathing/coughing (pneumonia, PE, pneumothorax, pleuritis)
Cardiovascular system:
- Chest pain - nonpleuritic (ACS, aortic dissection, valvular disease)
- Palpitations (arrhythmia causing dyspnea)
- Pedal edema (biventricular HF, nephrotic syndrome, hypoalbuminemia)
- Syncope / pre-syncope (severe valvular disease, severe PE)
- Paroxysmal nocturnal dyspnea / orthopnea (as above)
Systemic:
- Fever + productive cough (pneumonia, bronchitis, exacerbation of COPD/asthma)
- Weight loss + night sweats + chronic cough (TB, malignancy, HIV)
- Pallor / fatigue (anemia causing dyspnea)
- Ankle swelling + ascites (right heart failure, hepatic disease)
- Leg swelling (unilateral) (DVT -> PE; ask about Homan's sign history)
3. Past Medical History
- Known cardiac disease: CAD, valvular disease, hypertension, arrhythmia
- Known respiratory disease: asthma, COPD, TB (old or active), bronchiectasis, ILD
- Previous hospitalizations for breathlessness
- History of myocardial infarction or rheumatic fever
- Diabetes mellitus (accelerates CAD)
- History of cancer (lung cancer, PE risk, lymphangitis carcinomatosis)
- Anemia, thyroid disease
- Connective tissue disorders (Raynaud's, SLE, RA -> ILD or pulmonary hypertension)
4. Drug History
- ACE inhibitors -> dry cough (simulates dyspnea)
- Beta-blockers -> can precipitate bronchospasm in asthmatics
- Amiodarone, bleomycin, methotrexate -> pulmonary toxicity/fibrosis
- OCP / HRT (estrogen) -> PE risk
- NSAIDs -> can worsen asthma (aspirin-exacerbated respiratory disease)
- Current use of bronchodilators, diuretics (response confirms diagnosis)
5. Allergy History
- Drug allergies, environmental allergens, occupational sensitizers
- Ask about atopy (eczema, allergic rhinitis, hay fever) - "atopic triad" + asthma
6. Family History
- Asthma, atopy
- Coronary artery disease, hypertension
- Alpha-1 antitrypsin deficiency (early-onset COPD in non-smokers)
- Cystic fibrosis
7. Social History (extremely important for dyspnea)
Smoking
- Pack years = (packs/day) x (years smoked)
-
40 pack years strongly suggests COPD as a cause
- Current/ex-smoker (risk of lung cancer)
Occupation
- Dust exposure: coal, silica, asbestos -> pneumoconiosis (ask about type of work)
- Farming, bird-keeping, mushroom growing -> Hypersensitivity pneumonitis
- Improvement on weekends/holidays = occupational asthma
Alcohol
- Risk factor for cardiomyopathy, aspiration pneumonia
Travel / residence
- TB-endemic areas
- Recent long-haul travel or immobility -> PE risk
Living conditions
- Indoor cooking smoke/biomass fuel exposure (COPD in non-smokers)
- Pet/bird ownership (allergens, Chlamydophila psittaci)
8. Review of Systems (Quick Screening)
Ask briefly about:
- Weight loss / gain (malignancy vs. HF fluid)
- Appetite
- Joint pains / skin rashes (connective tissue disease)
- Swallowing difficulty (aspiration)
Key Summary: The "SOCRATES + Positional" Framework for Dyspnea
| Parameter | Key Question |
|---|---|
| Site | - |
| Onset | Sudden / gradual? |
| Character | Tightness / air hunger / effort? |
| Radiation | Associated chest pain? Where? |
| Associated symptoms | Cough, wheeze, oedema, fever, palpitations |
| Time course | Constant/intermittent? Morning/night? |
| Exacerbating/relieving | Exercise, cold, allergens, position, medications |
| Severity | MRC grade; how many stairs/meters? |
| Positional** (extra for SOB) | Orthopnea? PND? Bendopnea? Platypnea? |
Common Diagnoses to Identify from History Alone
| History Pattern | Likely Diagnosis |
|---|---|
| Smoker, >40 pack-years, progressive exertional SOB, morning cough | COPD |
| Young patient, episodic wheeze, nocturnal/cold-triggered, family history | Asthma |
| PND + orthopnea + pedal edema + history of HTN/MI/alcohol | Left/Biventricular Heart Failure |
| Sudden SOB + pleuritic chest pain + recent surgery/immobility/OCP/cancer | Pulmonary Embolism |
| Fever + productive cough + sudden SOB | Pneumonia |
| Thin young male, sudden SOB + pleuritic chest pain, no prior illness | Spontaneous Pneumothorax |
| Progressive SOB + dry cough + crackles in connective tissue disease patient | ILD |
| SOB + menorrhagia/melena/pale skin, no cardiorespiratory disease | Anemia |
| Occupational exposure to dust/birds, SOB improves on holiday | Hypersensitivity Pneumonitis / Occupational Asthma |
Sources:
- Goldman-Cecil Medicine, Ch. 71 - Approach to the Patient with Dyspnea
- Symptom to Diagnosis: An Evidence Based Guide, Ch. 15
- Fishman's Pulmonary Diseases and Disorders - Dyspnea and Breathlessness
- Textbook of Family Medicine, 9e - Shortness of Breath
Meningitis signs?
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
I now have comprehensive, authoritative content from Harrison's, Goldman-Cecil, Neuroanatomy through Clinical Cases, Frameworks for Internal Medicine, and Bradley & Daroff's Neurology. Here is the full answer:
Meningitis - Clinical Signs
The classic triad of meningitis is fever + headache + nuchal rigidity, but all three together are present in only ~44% of cases. A combination of any 2 of 4 features (headache, fever, stiff neck, altered mental status) is found in 95% of patients.
The Classic Signs of Meningeal Irritation
1. Nuchal Rigidity (Stiff Neck)
- The pathognomonic sign of meningeal irritation
- The neck resists passive flexion - patient cannot touch chin to chest
- Caused by reflex spasm of the extensor muscles of the neck due to inflammation of the meninges covering the cervical spinal cord
- Important caveat: In elderly patients, cervical spondylosis/osteoarthritis can cause false-positive nuchal rigidity. When meningitis is the cause, the neck resists flexion but can be rotated side-to-side (unlike cervical arthritis, where all movements are restricted)
2. Kernig's Sign
How to elicit:
- Patient lies supine
- Flex the thigh on the abdomen (hip flexed to 90°), with the knee also flexed to 90°
- Attempt to passively extend the knee
- Positive sign: Pain and resistance to knee extension (due to traction on inflamed lumbosacral nerve roots / meninges)
Mechanism: Inflamed nerve roots passing through the inflamed meninges are stretched when the knee is extended with the hip flexed.
3. Brudzinski's Sign
How to elicit:
- Patient lies supine
- Place one hand behind the patient's head and the other on the chest
- Passively flex the neck (bring chin toward chest)
- Positive sign: Reflex spontaneous flexion of both hips and knees
Mechanism: Passive neck flexion stretches the inflamed meninges and spinal cord, causing reflex hip and knee flexion to relieve tension.
Sensitivity note (Goldman-Cecil): Kernig's sign, Brudzinski's sign, and neck stiffness each have sensitivities of ~30% or lower in adults - their absence does NOT rule out meningitis. Both may be absent in very young children, elderly, immunocompromised, or patients with severely depressed consciousness.
4. Jolt Accentuation Test (newer sign)
- Patient rotates head horizontally at 2-3 times per second
- Positive: Worsening of headache
- Higher sensitivity than Kernig/Brudzinski for meningitis
Full Symptom and Sign Profile
Symptoms (in order of frequency - Goldman-Cecil data):
| Symptom | Frequency |
|---|---|
| Headache | 87% |
| Neck stiffness | 83% |
| Nausea | 74% |
| Fever | 77% |
| Altered mental status / confusion | >75% |
| Photophobia | Common |
| Phonophobia | Common |
| Vomiting | Common |
| Myalgia / backache | Common (esp. meningococcal) |
| Seizures | 15-40% |
Signs on Examination:
| Sign | Description |
|---|---|
| Nuchal rigidity | Neck resists passive flexion |
| Kernig's sign | Pain/resistance on knee extension with hip flexed |
| Brudzinski's sign | Reflex hip-knee flexion on passive neck flexion |
| Papilledema | Suggests raised ICP |
| Sixth (VI) nerve palsy | False localizing sign of raised ICP |
| Altered consciousness | Lethargy to coma |
| Focal neurological deficits | 33% - aphasia (23%), hemiparesis (7%) |
| Seizures | 15-40%; focal or generalized |
| Cushing's reflex | Bradycardia + hypertension + irregular respirations = impending herniation |
| Decerebrate posturing | Late sign of severe raised ICP |
Organism-Specific Signs
| Organism | Specific Sign |
|---|---|
| Neisseria meningitidis (meningococcal) | Diffuse erythematous maculopapular rash rapidly becoming petechial/purpuric on trunk, lower limbs, mucous membranes; non-blanching (classic exam Q!) |
| Listeria monocytogenes | Rhombencephalitis - ataxia, cranial nerve palsies |
| TB meningitis | Subacute onset, cranial nerve palsies (III, VI, VII), lymphocytic CSF, low glucose |
| Cryptococcal meningitis | Immunocompromised (HIV), raised ICP, india ink positivity |
| Herpes encephalitis / meningoencephalitis | Temporal lobe features - olfactory hallucinations, personality change, temporal seizures |
Signs of Raised ICP in Meningitis (>90% have CSF opening pressure >180 mmH₂O)
- Deteriorating/reduced level of consciousness
- Papilledema
- Dilated poorly reactive pupils
- Sixth nerve palsy (CN VI - false localizing)
- Decerebrate posturing
- Cushing's reflex (bradycardia, hypertension, irregular breathing)
Pathophysiology Diagram (Harrison's)
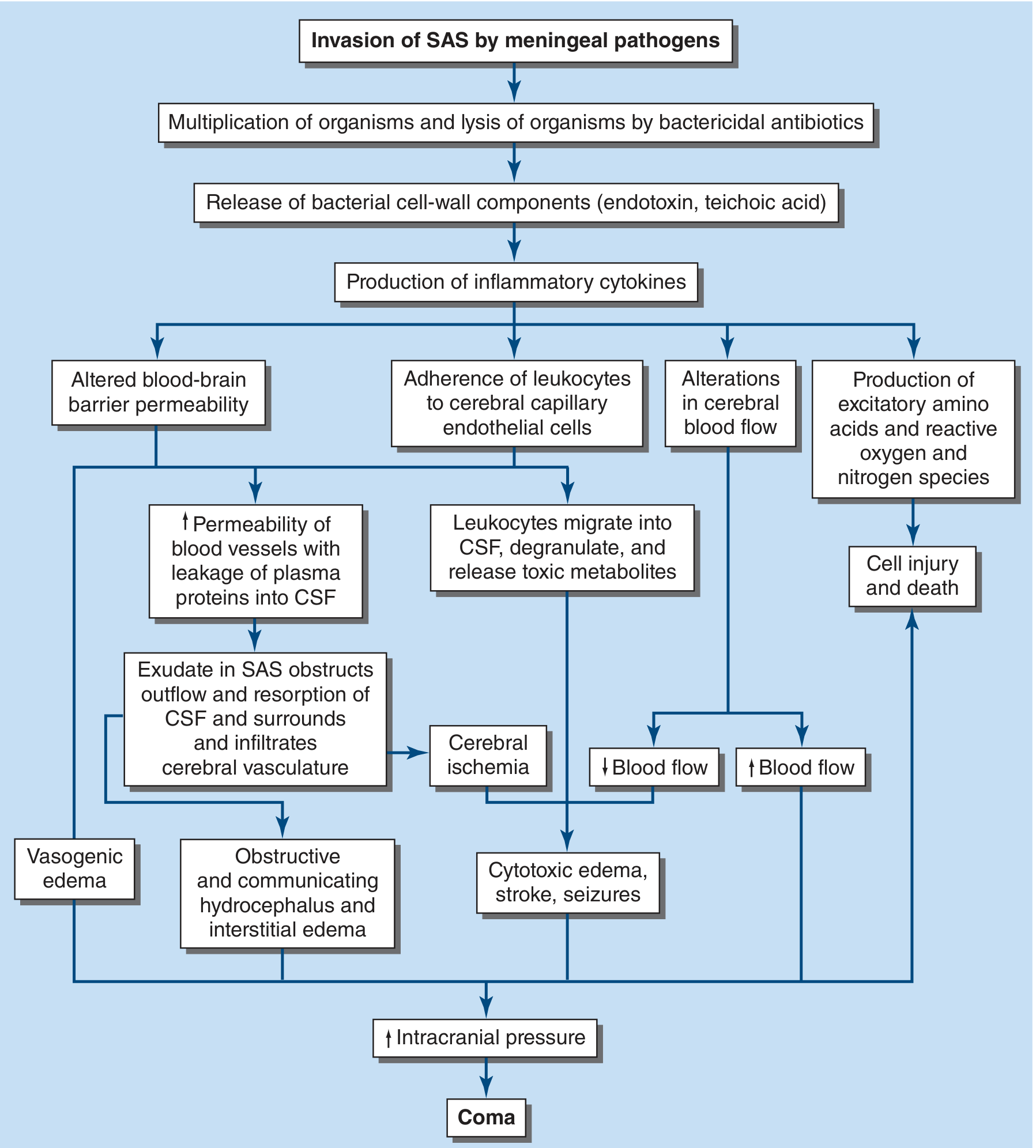
Invasion of subarachnoid space (SAS) -> inflammatory cytokines -> BBB disruption, vasogenic edema, hydrocephalus, raised ICP -> coma
CSF Profiles (Bonus for MBBS - always paired with signs)
| Condition | WBC /mm³ | Protein mg/dL | Glucose mg/dL |
|---|---|---|---|
| Normal | <5-10 (lymphocytes) | 15-45 | 50-100 |
| Bacterial meningitis | 100-5000 (PMNs) | 100-1000 (high) | <40 (low) |
| Viral meningitis | 10-300 (lymphocytes) | 50-100 | Normal |
| TB / Fungal | 10-200 (lymphocytes) | 100-200 | Low (<50) |
| Herpes encephalitis | 0-500 (lymphocytes) | 50-100 | Normal/low |
CSF glucose is abnormal if < 50% of simultaneous serum glucose (important rule).
Sources:
- Harrison's Principles of Internal Medicine, 22e, Ch. 143 - Bacterial Meningitis
- Goldman-Cecil Medicine, Ch. 381 - Bacterial Meningitis
- Neuroanatomy through Clinical Cases, 3e, Table 5.6 & 5.7
- Frameworks for Internal Medicine, Ch. 30 - Meningitis
All conditions leading to blurring of vison and headache
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Finding Sources
I now have comprehensive material from multiple authoritative textbooks covering all major conditions. Let me compile the complete answer.
Conditions Causing Blurred Vision + Headache
This combination is a high-yield clinical pairing because it signals raised intracranial pressure, vascular emergencies, or ocular emergencies until proven otherwise. Here is a systematic, organ-system based breakdown:
EMERGENCY / LIFE-THREATENING CAUSES (Rule Out First)
1. Raised Intracranial Pressure (Raised ICP) - Any Cause
- Headache: Dull, worsening with Valsalva, coughing, lying down; worst in morning
- Blurred vision: Due to papilledema (disc swelling compresses retinal nerve fibres)
- Other features: Nausea/vomiting, diplopia (CN VI palsy - false localizing sign), reduced consciousness
- Causes of raised ICP themselves include:
- Intracranial tumors (primary or metastatic)
- Brain abscess
- Subdural / extradural hematoma
- Hypertensive encephalopathy
- Cerebral venous sinus thrombosis (CVST)
- Hydrocephalus (obstructive or communicating)
2. Subarachnoid Hemorrhage (SAH)
- Headache: "Thunderclap" - sudden onset, "worst headache of my life"
- Blurred vision / visual disturbance: Subhyaloid (pre-retinal) hemorrhage on fundoscopy is pathognomonic; raised ICP causes papilledema
- Other features: Meningism, loss of consciousness, CN III palsy (posterior communicating artery aneurysm)
3. Hypertensive Emergency (Malignant Hypertension)
- BP: >180/120 mmHg with end-organ damage
- Headache: Severe occipital/generalized
- Blurred vision: Hypertensive retinopathy (flame haemorrhages, AV nicking, papilledema = Grade IV retinopathy)
- Other features: Encephalopathy, confusion, focal neurological signs, pulmonary edema, heart failure
- Goldman-Cecil: "obtundation, confusion, focal neurologic signs, seizures, heart failure, pulmonary edema, blurred vision, severe retinopathy confirms hypertensive emergency"
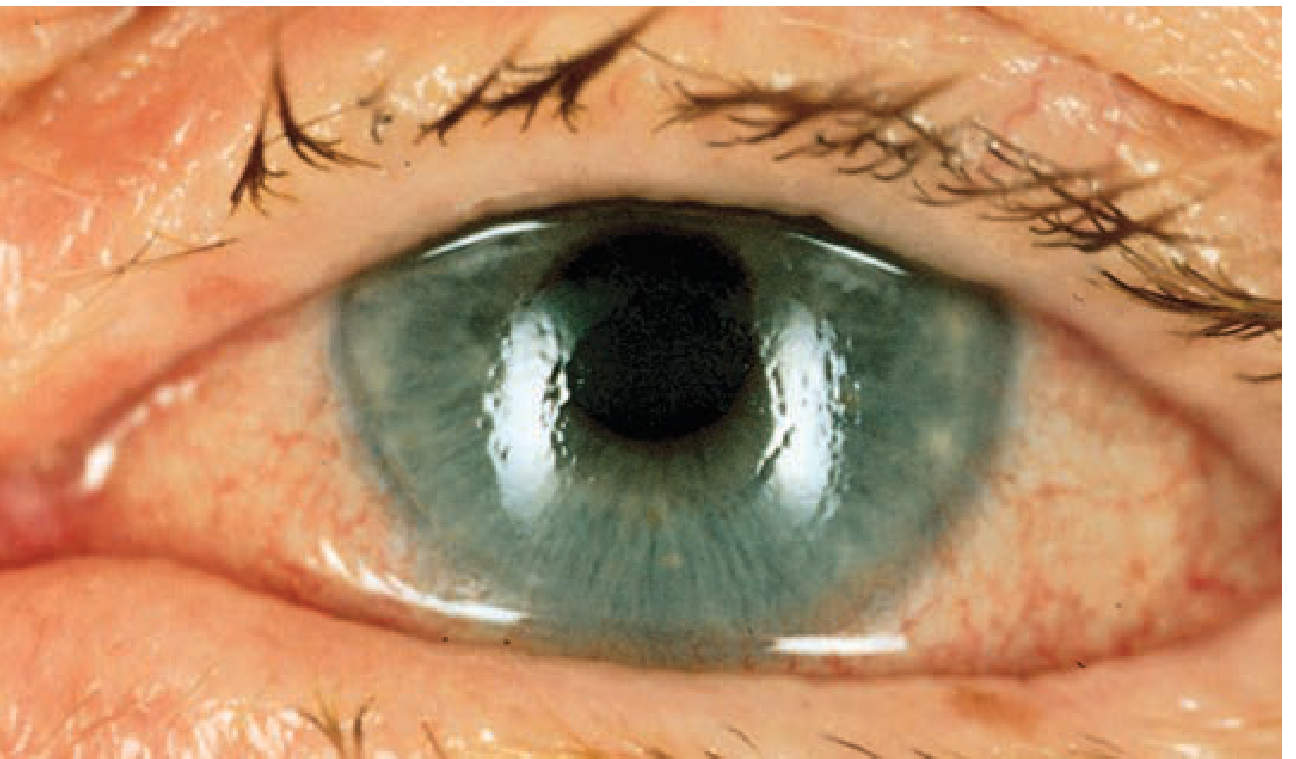
4. Acute Angle-Closure Glaucoma
- Headache: Sudden severe eye pain OR frontal/supraorbital headache
- Blurred vision: Corneal oedema causes hazy vision + coloured halos around lights
- Other features: Red eye, nausea/vomiting, fixed mid-dilated pupil, rock-hard globe
- Intraocular pressure: Can exceed 60-80 mmHg (normal 10-20 mmHg)
- Often misdiagnosed as migraine - key differentiator is the red eye and fixed mid-dilated pupil
5. Giant Cell (Temporal) Arteritis
- Age: >50 years (usually >60)
- Headache: Temporal, scalp tenderness, tender temporal artery on palpation
- Blurred vision / visual loss: Anterior ischemic optic neuropathy (AION) - can cause sudden permanent monocular visual loss (ophthalmological emergency)
- Other features: Jaw claudication, polymyalgia rheumatica, elevated ESR (>50), elevated CRP, weight loss, fever
- Risk: Permanent blindness if steroids not started immediately
6. Cerebral Venous Sinus Thrombosis (CVST)
- Headache: Progressive, can be thunderclap
- Blurred vision: Papilledema from raised ICP
- At-risk populations: Women on OCP, peripartum, hypercoagulable states
- Other features: Focal deficits, seizures, altered consciousness
7. Pituitary Apoplexy
- Headache: Sudden severe headache
- Blurred vision + visual field defects: Bitemporal hemianopia (chiasmal compression) or acute diplopia (CN III, IV, VI palsy)
- Other features: Nausea, vomiting, meningism, hypopituitarism, reduced consciousness
NEUROLOGICAL CAUSES
8. Migraine with Aura
- Headache: Unilateral, throbbing, moderate-severe, with nausea/vomiting/photophobia
- Blurred vision / Visual aura (precedes headache by 20-60 min):
- Scintillating scotoma (zigzag lines)
- Fortification spectra
- Visual field defects
- Flashing lights (photopsia)
- Subtypes with visual features:
- Migraine with typical aura
- Retinal migraine (monocular visual symptoms)
- Migraine with brainstem aura (diplopia, vertigo, tinnitus)
- Hemiplegic migraine
9. Idiopathic Intracranial Hypertension (IIH) / Pseudotumor Cerebri
- Who: Obese women of childbearing age (incidence 19-21 per 100,000 in this group)
- Headache: Dull, pressure-like, fluctuating, often occipital; worsens with Valsalva
- Blurred vision: Transient visual obscurations (seconds, coincide with peak headache), papilledema (uni or bilateral), enlarged blind spot, peripheral field loss
- Other features: Horizontal diplopia (CN VI palsy), self-audible pulsatile tinnitus, shoulder/neck pain, face numbness
- CSF pressure: 250-450 mmHg₂O (LP is both diagnostic and therapeutic)
- No mass on imaging; normal CSF composition
- Risk of permanent visual loss if untreated
10. Intracranial Tumors (Primary or Secondary)
- Headache: Dull, worse in morning or on bending/coughing; progressive
- Blurred vision: Due to papilledema from raised ICP; or direct visual pathway involvement
- Other features: Focal deficits, seizures, personality change, cognitive decline
11. Stroke / TIA (Posterior Circulation)
- Sudden headache + visual disturbance
- Types of visual disturbance:
- Homonymous hemianopia (occipital cortex)
- Diplopia (brainstem)
- Transient monocular blindness = amaurosis fugax (ICA disease / retinal artery)
- Other features: Vertigo, ataxia, dysphagia, dysarthria (posterior circulation)
OPHTHALMIC CAUSES
12. Uveitis (Anterior / Posterior)
- Headache: Periorbital pain, photophobia
- Blurred vision: Cells and flare in anterior chamber
- Red eye (anterior uveitis), associated with systemic conditions (AS, sarcoidosis, IBD, reactive arthritis)
13. Optic Neuritis
- Headache/Pain: Pain on eye movement
- Blurred vision: Unilateral visual loss; RAPD (relative afferent pupillary defect)
- Associated with: Multiple sclerosis
- Central scotoma on visual field testing
14. Scleritis
- Severe boring orbital/periorbital pain (can radiate as headache)
- Blurred vision: Secondary to uveitis or scleral inflammation
- Associated with RA, vasculitis, SLE
SYSTEMIC / METABOLIC CAUSES
15. Preeclampsia / Eclampsia
- Pregnant woman (>20 weeks) or postpartum
- Headache + blurred vision are warning symptoms of severe preeclampsia (alongside epigastric pain)
- Other features: Hypertension, proteinuria, oedema, can progress to seizures (eclampsia)
16. Diabetic Maculopathy / Hypertensive Retinopathy
- Chronic blurred vision + headache from underlying HTN/DM
- Fundoscopy shows retinal changes
17. Carbon Monoxide Poisoning
- Headache (most common symptom), blurred vision, confusion, nausea
- History of exposure (indoor heating, fires)
18. Anemia (Severe)
- Throbbing headache from hyperdynamic circulation
- Visual symptoms including visual disturbance, spots
19. Hypoglycemia
- Headache, visual blurring, confusion, sweating, palpitations
- In diabetics on insulin/sulfonylureas
20. Multiple Sclerosis
- Headache uncommon, but optic neuritis (painful monocular visual loss) + other demyelinating episodes
OCULAR / REFRACTIVE CAUSES (Benign - More Common)
21. Uncorrected Refractive Errors (Myopia, Hypermetropia, Astigmatism)
- Blurred vision + eye strain headache (frontal, after prolonged reading/screen use)
- Accommodative spasm in young patients
22. Convergence Insufficiency / Accommodative Spasm
- Blurred vision on near-far shift + frontal headache; common in teenagers under stress
23. Presbyopia (Age-related)
- Near blur + headache with near work in >40 years
Quick Summary Table
| Condition | Headache Type | Vision Change | Key Clue |
|---|---|---|---|
| Raised ICP (any cause) | Dull, morning, Valsalva | Papilledema, blurring | Worse on coughing/bending |
| SAH | Thunderclap | Subhyaloid bleed, papilledema | "Worst headache of life" |
| Hypertensive emergency | Severe occipital | Retinopathy, papilledema | BP >180/120 + end-organ damage |
| Acute angle-closure glaucoma | Frontal/supraorbital | Halos, hazy vision | Red eye, fixed mid-dilated pupil |
| Giant cell arteritis | Temporal | Sudden monocular loss | Age >50, jaw claudication, high ESR |
| IIH/Pseudotumor cerebri | Dull pressure | Transient obscurations, papilledema | Obese young woman, no mass on imaging |
| Migraine with aura | Throbbing unilateral | Scintillating scotoma, zigzag lines | Visual aura precedes headache |
| Pituitary apoplexy | Sudden severe | Bitemporal hemianopia | Known pituitary adenoma |
| CVST | Progressive | Papilledema | OCP use, pregnancy, hypercoagulable |
| Optic neuritis | Pain on eye movement | Monocular visual loss, RAPD | MS association |
| Preeclampsia | Throbbing | Visual blurring | Pregnant, hypertension, proteinuria |
| Carbon monoxide | Throbbing | Blurring | Exposure history, cherry-red skin |
| Refractive error | Frontal, eye strain | Blurred near/distance | Normal fundus, corrects with glasses |
Sources:
- Adams & Victor's Principles of Neurology, 12e - Pseudotumor Cerebri
- Tintinalli's Emergency Medicine - Acute Angle-Closure Glaucoma
- Rosen's Emergency Medicine - Headache, IIH
- Goldman-Cecil Medicine - Hypertensive Emergency
- Bradley & Daroff's Neurology - Migraine, Headache Etiologies
- Wills Eye Manual - Ophthalmic conditions
- Creasy & Resnik's Maternal-Fetal Medicine - Preeclampsia
What if loss of conscious was also associated then diffentials would be?
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
I have everything needed to build a focused, high-quality answer. Here it is:
Headache + Blurred Vision + Loss of Consciousness - Differentials
Adding loss of consciousness (LOC) to the previous two symptoms immediately narrows the list to serious, often life-threatening conditions. LOC indicates either:
- Diffuse cortical dysfunction (metabolic, toxic, raised ICP)
- Reticular activating system (RAS) disruption (brainstem, herniation)
- Transient cerebral hypoperfusion
This triad = neurovascular/raised ICP emergency until proven otherwise.
PRIORITY EMERGENCIES (Act First)
1. Subarachnoid Hemorrhage (SAH)
- Thunderclap headache ("worst headache of life") → visual disturbance (subhyaloid haemorrhage, papilledema) → LOC
- LOC at onset occurs in ~50% of cases; may be brief or prolonged
- Meningism (neck stiffness, photophobia), CN III palsy (posterior communicating artery aneurysm)
- Investigations: Non-contrast CT head (first), LP if CT negative (xanthochromia)
2. Hypertensive Encephalopathy / Malignant Hypertension
- BP severely elevated (>180/120 mmHg)
- Headache → blurred vision (hypertensive retinopathy, papilledema) → confusion → LOC/coma
- PRES (Posterior Reversible Encephalopathy Syndrome): Variant - occipital headache, cortical blindness, seizures, LOC; MRI shows bilateral posterior white matter oedema
- Other features: Seizures, focal deficits, papilledema
3. Cerebral Herniation (from any raised ICP cause)
- Progressive headache → papilledema/blurred vision → deteriorating consciousness → coma
- Cushing's triad (bradycardia + hypertension + irregular breathing) = impending uncal herniation
- CN III palsy (blown pupil = fixed dilated pupil) = uncal herniation compressing CN III
- Underlying causes: Expanding haematoma (extradural, subdural, intracerebral), tumour, abscess, massive infarct
4. Eclampsia
- In pregnant or postpartum women
- Preeclampsia prodrome: headache + blurred vision + epigastric pain + hypertension + proteinuria
- → LOC with tonic-clonic seizures = eclampsia
- Rosen's Emergency Medicine: "headache, visual abnormalities and confusion, as well as focal neurologic deficits" are key warning features before seizure and loss of consciousness
5. Pituitary Apoplexy
- Sudden haemorrhage/infarction into a pituitary adenoma
- Triad: Severe sudden headache + bilateral visual changes + ophthalmoplegia
- → Cardiovascular collapse and loss of consciousness in severe cases
- Other: Meningeal irritation, CN III/IV/VI palsies, bitemporal hemianopia (chiasmal compression)
- Harrison's: "Acute symptoms may include severe headache with signs of meningeal irritation, bilateral visual changes, ophthalmoplegia, and, in severe cases, cardiovascular collapse and loss of consciousness"
- Investigations: MRI pituitary (shows haemorrhage); urgent surgical decompression if LOC or visual loss
6. Meningoencephalitis
- Headache + photophobia/visual changes + progressive LOC/coma (indicates encephalitic component)
- Fever, neck stiffness, Kernig's/Brudzinski's signs
- Herpes encephalitis specifically causes temporal lobe features + LOC
- CSF examination is diagnostic
7. Massive Ischaemic Stroke / Basilar Artery Occlusion
- Basilar artery thrombosis = classic: diplopia/blurred vision (brainstem) + severe headache + progressive LOC → "locked-in" state or coma
- Posterior circulation TIA/stroke: visual disturbances + drop attacks (transient LOC)
- Rosen's: "Because this system supplies the reticular activating system... loss of consciousness with vomiting, visual changes, and cerebral ataxia may be seen"
8. Cerebral Venous Sinus Thrombosis (CVST)
- Progressive headache → papilledema (blurred vision) → seizures → LOC
- Risk groups: OCP, postpartum, dehydration, hypercoagulable states
- Can be subacute over days to weeks
- MRI + MR venography is investigation of choice
9. Acute Subdural / Extradural Haematoma
- Extradural (EDH): Classic "lucid interval" - brief LOC, recovery, then rapid deterioration with headache + blown pupil + hemiparesis → coma (middle meningeal artery rupture)
- Subdural (SDH): Headache + blurred vision from raised ICP + gradual LOC; may occur with trivial trauma in elderly/anticoagulated patients
10. High-Altitude Cerebral Oedema (HACE)
- Headache + visual changes → ataxia + altered consciousness (hallmarks)
- Harrison's: "hallmarks are ataxia and altered consciousness with diffuse cerebral involvement... Papilledema and, more commonly, retinal haemorrhages"
- History of recent ascent to high altitude
METABOLIC / TOXIC CAUSES (LOC + Headache + Visual Symptoms)
11. Severe Hypoglycaemia
- Headache + visual disturbances → drowsiness → LOC/coma if untreated
- Washington Manual: "fatigue, dizziness, headache, visual disturbances, drowsiness...inability to concentrate, abnormal behavior, confusion, and ultimately loss of consciousness or seizures"
- History: diabetic on insulin/sulfonylurea, missed meal
12. Carbon Monoxide Poisoning
- Headache (most common symptom) + visual blurring + confusion → LOC/coma
- Cherry-red skin (unreliable sign), COHb levels diagnostic
- History: indoor fire, faulty heating, others in same location affected
13. Hyperventilation Syndrome / Hypocapnia
- Headache + visual disturbances + perioral tingling + carpopedal spasm → LOC (syncope)
- Bradley & Daroff: "lightheadedness, perioral paresthesias, visual disturbances, headache, unsteadiness... and loss of consciousness"
- Anxiety/panic attack precipitant; CO₂ low on ABG
14. Wernicke's Encephalopathy (Thiamine deficiency)
- Triad: Ophthalmoplegia/nystagmus (blurred/double vision) + ataxia + confusion/altered consciousness
- Headache may be present
- History: alcoholism, malnutrition, prolonged vomiting (hyperemesis)
- Emergency: IV thiamine before glucose
Differentiating the LOC
| Type of LOC | Suggests |
|---|---|
| Sudden LOC at onset of headache | SAH, cardiac arrhythmia, massive haemorrhage |
| Brief LOC then lucid interval then deterioration | Extradural haematoma |
| Progressive drowsiness → LOC over hours/days | Subdural, raised ICP, meningoencephalitis, CVST |
| LOC with seizures | Eclampsia, hypertensive encephalopathy, PRES, meningoencephalitis |
| LOC with postural/exertional trigger | Colloid cyst of 3rd ventricle (sudden obstructive hydrocephalus) |
| LOC with metabolic prodrome (sweating, palpitations) | Hypoglycaemia |
| LOC at high altitude | HACE |
Red Flag Summary - "HEADACHE + BLURRED VISION + LOC" Approach
LOC sudden at onset of headache?
→ SAH (CT head stat), cardiac arrhythmia
LOC with fever + neck stiffness?
→ Meningoencephalitis (LP after CT)
LOC with very high BP + seizures?
→ Hypertensive encephalopathy / Eclampsia (if pregnant)
LOC with blown pupil (fixed dilated) + hemiparesis?
→ Transtentorial herniation - Extradural/Subdural haematoma (CT head stat)
LOC with ophthalmoplegia + severe headache?
→ Pituitary apoplexy (MRI sella)
LOC with ataxia at high altitude?
→ HACE (descend immediately + dexamethasone)
LOC with headache + visual symptoms in diabetic?
→ Hypoglycaemia (BGL stat)
LOC with CO exposure history?
→ Carbon monoxide poisoning (COHb levels, 100% O₂)
Key principle (Tintinalli's): Any headache with altered consciousness or papilledema is a red flag requiring urgent neuroimaging before anything else. Never do LP before CT if raised ICP is suspected (risk of coning).
Sources: Harrison's Principles 22e, Rosen's Emergency Medicine, Tintinalli's Emergency Medicine, Plum & Posner's Diagnosis of Stupor and Coma, Bradley & Daroff's Neurology, Washington Manual
This is a shared conversation. Sign in to Orris to start your own chat.