Per cutaneous tracheotomy in detail
Reading File
Finding Sources
Finding Sources
Searching PubMed
percutaneous tracheostomy technique complications
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the information needed for a thorough, detailed answer. Here it is:
Percutaneous Tracheotomy - A Detailed Review
1. Definition and Historical Background
Percutaneous tracheotomy (also called percutaneous dilational tracheotomy/tracheostomy, PDT) is a minimally invasive bedside procedure for establishing a surgical airway via progressive dilation of a stoma through the anterior tracheal wall, without formal open neck dissection. It uses the Seldinger technique as its basis.
-
First described by Toye and Weinstein in 1969 using the Seldinger technique
-
Popularized by Ciaglia in 1985 with his dilational percutaneous technique
-
Now the most commonly performed alternative airway procedure in ICU patients on prolonged mechanical ventilation
-
Cummings Otolaryngology Head and Neck Surgery
-
Scott-Brown's Otorhinolaryngology Head & Neck Surgery
2. Indications
| Indication | Notes |
|---|---|
| Prolonged mechanical ventilation (>7-10 days anticipated) | Most common indication |
| Airway protection (neurological injury, obtunded patient) | |
| Facilitation of weaning from ventilator | |
| Severe obstructive sleep apnea / upper airway obstruction | |
| Pulmonary toilet (copious secretions) | |
| Failed or anticipated difficult intubation |
PDT offers a logistical advantage over open surgery: in one series of 368 tracheotomies, the average time from consultation to procedure was 7.4 days for PDT vs. 14 days for open surgery, saving >$400 per procedure and reducing transport-related adverse events (serious events occur in ~8.9% of ICU transports).
3. Contraindications
Absolute
- Children / pediatric age group - the collapsible, mobile trachea is difficult to stabilize; bronchoscope management through a pediatric ETT is impractical
- Severe clinical instability - when bronchoscopy is not tolerated
Relative (favor open technique)
- Midline neck masses - obscure landmarks
- Uncorrectable coagulopathy (PT/PTT >1.5x control, platelets <50,000/mm³) - hemostasis cannot be achieved as in open surgery
- High respiratory support (FiO2 >70%, high PEEP) - deoxygenation risk during bronchoscopy
- Morbid obesity - BMI >30 kg/m² is an independent risk factor; landmark palpation difficult; 80% of accidental decannulations occur in this group
- Cervical spine instability - neck extension required
- High-riding innominate artery or aberrant vasculature
- Previous neck surgery / radiation - distorted anatomy
- Suspected cervical tracheal pathology (stenosis, tumor)
- Fishman's Pulmonary Diseases and Disorders; Current Surgical Therapy 14e
4. Equipment
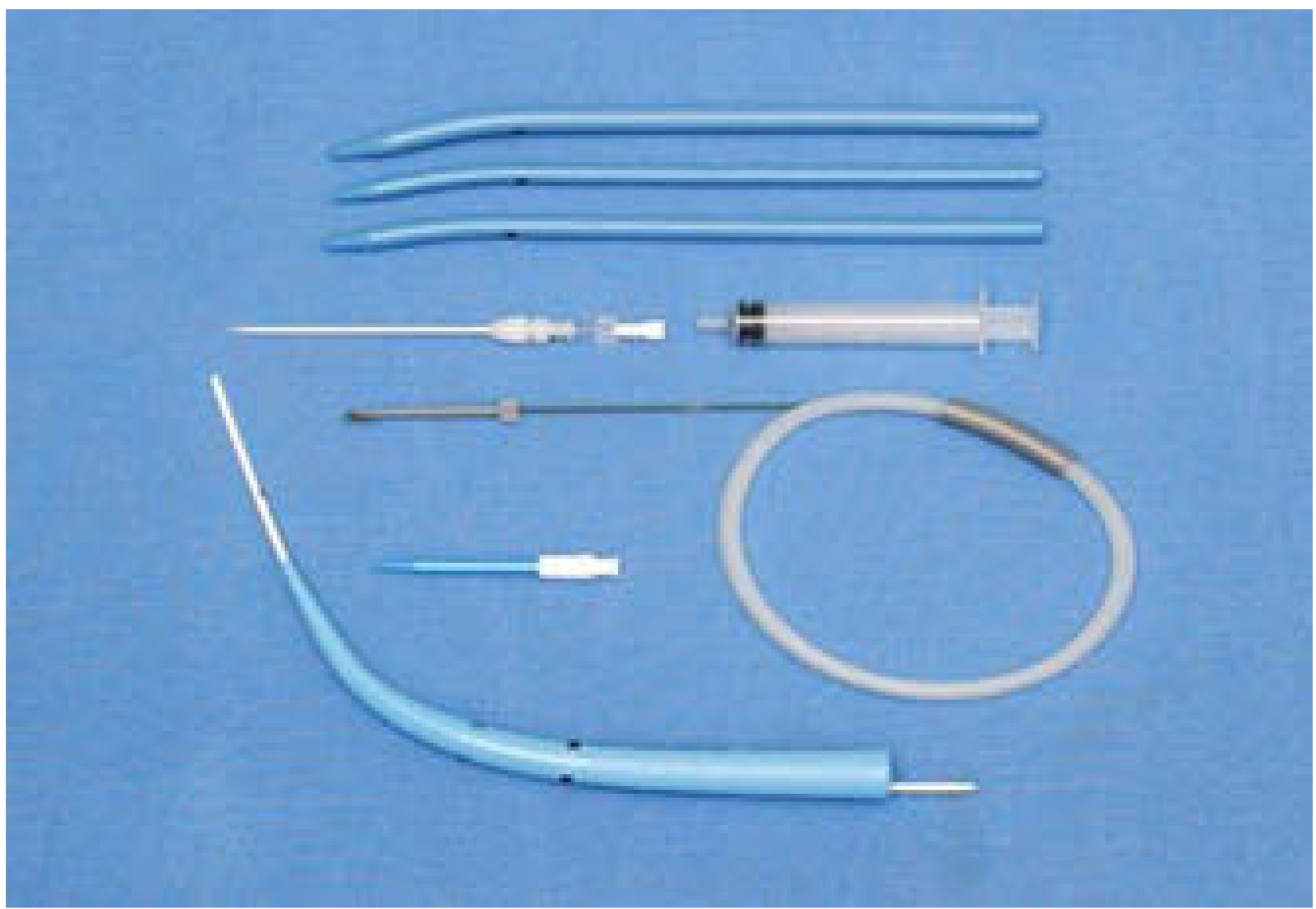
Percutaneous tracheostomy set (from Scott-Brown's Otorhinolaryngology) - showing serial dilators (blue), 14-gauge introducer needle with syringe, J-tipped guidewire, and tracheostomy tube with obturator.
Standard components of a PDT kit (e.g., Ciaglia Blue Rhino, Cook Medical):
- 14-gauge (or 22-gauge seeker) introducer needle with syringe
- J-tipped guidewire
- 12-Fr short dilating catheter (initial dilator)
- Single tapered hydrophilic-coated dilator (Blue Rhino - replaced older serial dilators)
- Appropriately sized tracheostomy tube loaded on loading dilator
- Flexible videobronchoscope
- 1% lidocaine with 1:100,000 epinephrine
5. Pre-Procedure Evaluation
- History and respiratory status review - FiO2, PEEP, ventilator settings
- Physical examination - palpate thyroid cartilage, cricoid, tracheal rings 1-3; inspect for midline vessels
- Review existing CT imaging - assess vascular anatomy, particularly high-riding innominate artery or aberrant vessels
- Ultrasound assessment - increasingly recommended to evaluate vasculature overlying the puncture path
- Laboratory studies - platelet count, PT, PTT, BUN (uremia requires DDAVP pretreatment)
- Staffing - anesthesiologist or airway-trained physician at head of bed to manage ETT, perform bronchoscopy, and administer sedation; scrub nurse as non-sterile circulator
- Current Surgical Therapy 14e
6. Step-by-Step Technique (Ciaglia PDT - Standard Method)
Setup
- Place shoulder roll to extend the neck (unless contraindicated)
- Increase FiO2 to 1.0
- Administer sedation, analgesia, and short-acting paralysis to minimize coughing
- Prep and drape in sterile fashion
- Identify landmarks: hyoid, thyroid cartilage, cricoid cartilage, tracheal rings
Incision and Dissection
- Inject 1% lidocaine with 1:100,000 epinephrine (up to 10 cc) into skin and subcutaneous tissue
- Make a 1-2 cm horizontal incision below the inferior border of the cricoid toward the sternal notch
- Bluntly dissect with a hemostat in the midline through subcutaneous tissue until tracheal rings are palpable
Bronchoscopic Guidance
- Advance bronchoscope through the ETT - position it at the distal end of the tube
- Withdraw the ETT to the level of the vocal cords - the bronchoscopist uses transillumination through the anterior neck incision to gauge how far to retract
- Deflate the ETT cuff
Needle Entry
- Insert a 14-gauge (or 22-gauge seeker) needle on a saline-filled syringe between tracheal rings 1-2 or 2-3 (ideal entry zone is between 10 and 2 o'clock on the anterior tracheal wall)
- Confirm placement by:
- Aspiration of air (or air bubbling through saline)
- Direct bronchoscopic visualization of needle entering the tracheal lumen midline, away from the posterior membrane
Seldinger Technique - Wire and Dilation
- Remove syringe while holding needle steady; advance J-tipped guidewire toward the carina through the needle
- Remove needle/catheter, leaving guidewire in place
- Pass the short 12-Fr dilating catheter (guiding catheter) over the wire for initial dilation
- Load the tracheostomy tube onto the single tapered Blue Rhino dilator; advance the entire assembly over the guidewire under continuous bronchoscopic visualization - the dilator passes through the stoma while stretching the tracheal wall
Tube Placement and Confirmation
- Once in the tracheal lumen, remove the guidewire, guiding catheter, and loading dilator while holding the tracheostomy tube in place
- Inflate the cuff of the tracheostomy tube
- Confirm position by:
- Bronchoscopy through the ETT (confirm tube is below cords in lumen)
- Bronchoscopy through the tracheostomy tube itself
- Return of tidal volumes from ventilator once circuit connected
- Secure with suture through flanges and neck ties
- Remove ETT once tracheostomy is confirmed functional
- Cummings Otolaryngology Head & Neck Surgery (Box 7.3); Current Surgical Therapy 14e
7. Alternative Percutaneous Techniques
| Technique | Description |
|---|---|
| Ciaglia Blue Rhino (standard) | Single tapered hydrophilic dilator over guidewire - replaced serial dilation; faster with less instrumentation |
| Griggs (Portex) | Guidewire dilating forceps spread through anterior neck tissue into trachea; tube fed over guidewire |
| Fantoni Translaryngeal Tracheostomy | Retrograde method - guidewire passed antegrade from trachea, pulled out through mouth, cuffed cannula pulled through larynx and out through anterior wall |
| PercuTwist (Rusch-Teleflex) | Screw-shaped single dilator twisted clockwise over wire, engaging and pulling the tracheal wall anteriorly while dilating; 9.0 tube placed with insertional dilator |
Note: All except Ciaglia Blue Rhino are not currently commercially available in the United States.
8. Bronchoscopic Guidance
Bronchoscopic guidance is now standard of care for PDT:
- Without guidance: overall complication rate ~16.8%
- With bronchoscopic guidance: complication rate ~8.3%
Primary function is to protect the posterior membranous tracheal wall from perforation. If the patient has minimal respiratory demands, a laryngeal mask airway (LMA) can replace the ETT to improve bronchoscopic visualization.
A 2026 systematic review (PMID: 41845239) confirmed the safety benefit of bronchoscopic guidance in PDT. Additionally, a 2025 meta-analysis (PMID: 40281422) found ultrasound-guided PDT superior to landmark-guided PDT in reducing complications, supporting the use of ultrasound for pre-procedural vascular mapping.
9. Complications
Intraoperative / Early Complications
| Complication | Notes |
|---|---|
| Posterior tracheal wall perforation | 50/10,000 in PDT vs. 6/10,000 in open surgery; prevented by bronchoscopic guidance |
| Desaturation / hypoxemia | From bronchoscope dead space or prolonged procedure |
| Hypotension | Sedation, vasovagal, or hemorrhage related |
| Bleeding | Less than surgical in most series; vessel ligation not possible in PDT |
| False passage | Extraluminal passage of dilator |
| Pneumothorax | Rare; post-procedure CXR mandatory |
| Pneumomediastinum | Rare |
| Cardiorespiratory arrest | 149/10,000 in PDT vs. 86/10,000 in open surgery in one meta-analysis |
| Subcutaneous emphysema | |
| Esophageal injury/puncture | Rare; prevented by bronchoscopic visualization |
Late Complications
| Complication | Notes |
|---|---|
| Accidental decannulation | Most common catastrophic event; more frequent in obese patients; accounts for ~34% of catastrophic events |
| Tube obstruction | Most frequent cause of tracheotomy emergencies; managed with suctioning |
| Tracheoinnominate artery fistula (TIF) | >90% of major bleeding events; more common in pediatric population; presents as sentinel bleed then massive hemorrhage |
| Tracheal stenosis | Higher incidence if cricothyroid membrane involved; risk from high-pressure cuff |
| Tracheoesophageal fistula | Rare but catastrophic; presents with dysphagia/aspiration post-op |
| Wound infection | Less common in PDT than open surgery |
| Tracheocutaneous fistula | Long-term complication; prevented by stepwise decannulation technique |
| Aspiration | Tracheostomy tethers larynx; reduces cough reflex by limiting subglottic pressure |
A survey of the American Academy of Otolaryngology found ~1000 catastrophic tracheostomy events per year, with ~50% causing death or permanent morbidity. The vast majority occurred >7 days after procedure.
- Fishman's Pulmonary Diseases and Disorders
10. PDT vs. Open (Surgical) Tracheostomy
| Parameter | PDT | Open Surgical |
|---|---|---|
| Setting | ICU bedside | Operating room (preferred) |
| Time to procedure | Shorter (avg. 7.4 days) | Longer (avg. 14 days) |
| Cost | Lower (~$400 savings) | Higher |
| Wound infection | Less | More in some studies |
| Bleeding | Less in most series | More (but better hemostasis control) |
| Posterior wall injury | Higher (50 vs. 6 per 10,000) | Lower |
| Serious perioperative events | Higher in some series | Lower in some series |
| Hemostasis control | Limited | Full (ligation, cautery) |
| Complex anatomy | Less suitable | Preferred |
| Coagulopathy | Relative contraindication | Preferred approach |
| Obesity | Relative contraindication | Preferred (can use Björk flap) |
| Late complications | Similar | Similar |
Meta-analytic evidence is equivocal overall, with different studies favoring one technique for specific endpoints. A 17-RCT meta-analysis (1212 patients) showed fewer infections and less bleeding with PDT; however, an earlier observational meta-analysis (65 trials by Dulguero et al.) found serious perioperative events (cardiorespiratory arrest, pneumothorax, pneumomediastinum) were significantly more common in PDT (149 vs. 86 per 10,000).
- Current Surgical Therapy 14e
11. Post-Procedure Care
- Post-procedure chest X-ray mandatory in all patients (pneumothorax)
- Confirm correct tube position clinically and radiographically
- Cuffed tube used initially to protect airway from secretions; can be changed to uncuffed after 3-4 days
- Cuff pressure monitoring - must stay below mucosal capillary occlusion pressure to prevent subglottic stenosis
- Tube secured with neck ties (tied with head in flexion) or flanges sutured to skin
- Stepwise decannulation: downsize tube, cap tube, tape stoma, instruct patient on occlusion during speech and coughing
- Tracheocutaneous fistula if persistent requires staggered three-layer local tissue repair
12. Special Considerations
- Obesity (BMI >30): independent risk factor; 15% complication rate vs. 8% in non-obese; 80% of accidental decannulations occur in this group - consider open Björk flap
- Uremia: PDT can be performed safely but pretreat with DDAVP
- COVID-19 / aerosol-generating procedures: tracheotomy is an aerosol-generating procedure (AGP); requires full PPE, negative pressure room, minimal staff, bronchoscopy protocol modifications
- Children: PDT is contraindicated - mobile, collapsible trachea; inadequate ventilation during bronchoscopy through pediatric ETT
Sources:
- Cummings Otolaryngology Head and Neck Surgery (Chapters on Percutaneous Tracheotomy)
- Current Surgical Therapy, 14th Edition (Percutaneous Dilatational Tracheostomy)
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery
- Bailey and Love's Short Practice of Surgery, 28th Edition
- Fishman's Pulmonary Diseases and Disorders
- Dong X et al. (2026) - PDT with vs. without bronchoscopic guidance PMID: 41845239
- Wen D et al. (2025) - Ultrasound- vs. landmark-guided PDT meta-analysis PMID: 40281422
This is a shared conversation. Sign in to Orris to start your own chat.