H pylori infection symptoms
Reading File
Finding Sources
Searching the Web
H pylori infection symptoms clinical presentation
Searching PubMed
"Helicobacter pylori" AND symptoms
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Here is a thorough overview of H. pylori infection symptoms based on multiple authoritative medical textbooks.
Helicobacter pylori Infection - Symptoms & Clinical Presentation
The Most Important Point: Most Infections Are Asymptomatic
The majority of people infected with H. pylori never develop symptoms. The organism colonises the gastric mucosa and triggers chronic inflammation, but overt disease only develops in a subset of those infected. Symptoms that do appear are largely the result of gastritis, peptic ulcer disease, or - in rare cases - gastric cancer or MALT lymphoma.
Common Symptoms (When Present)
Upper abdominal / epigastric pain
- A burning, gnawing, or dull ache in the upper abdomen (epigastric region) is the hallmark symptom
- Pain is often worse on an empty stomach and may temporarily improve after eating (duodenal ulcer pattern) or worsen with meals (gastric ulcer pattern)
- Waking at night with abdominal pain is characteristic
Dyspepsia
- A broad term covering upper abdominal discomfort, bloating, early satiety, and indigestion
- H. pylori gastritis is the cause of dyspepsia in a subset of patients - a reliable indicator is that successful eradication produces sustained symptomatic remission
- Per Goldman-Cecil Medicine: if eradication of H. pylori resolves dyspeptic symptoms, the diagnosis is reclassified as H. pylori gastritis rather than functional dyspepsia
Nausea and vomiting
- Common accompaniments, especially during acute flares or when ulcers develop
Bloating and belching
- Disruption of the gastric mucosal barrier and altered gastric motility can cause a sense of fullness and excess gas
Loss of appetite and unintentional weight loss
- More common when there is significant gastritis or ulceration
Alarm / Red-Flag Symptoms (Require Urgent Evaluation)
These symptoms suggest complicated peptic ulcer disease (bleeding, perforation) or malignancy and need immediate medical attention:
| Symptom | What it may indicate |
|---|---|
| Vomiting blood (haematemesis) | Bleeding ulcer or Mallory-Weiss tear |
| Black, tarry stools (melaena) | Upper GI haemorrhage |
| Bright red blood in stools | Lower GI bleed or massive upper GI bleed |
| Severe, sudden epigastric pain | Perforated ulcer |
| Progressive dysphagia | Gastric cancer |
| Persistent vomiting | Pyloric obstruction |
| Significant unintentional weight loss | Gastric malignancy |
Mechanisms Behind the Symptoms
H. pylori produces urease, which breaks down urea into ammonia. Ammonia is a strong alkali that:
- Disrupts the gastric mucous barrier
- Stimulates antral G-cells to release gastrin, causing inappropriate hypergastrinaemia and acid hypersecretion
- Triggers a classical inflammatory response with neutrophil migration and macrophage/lymphocyte accumulation in the gastric epithelium
Some strains produce cytotoxins (CagA and VacA), which are specifically associated with the more severe outcomes of gastritis, peptic ulceration, and gastric cancer.
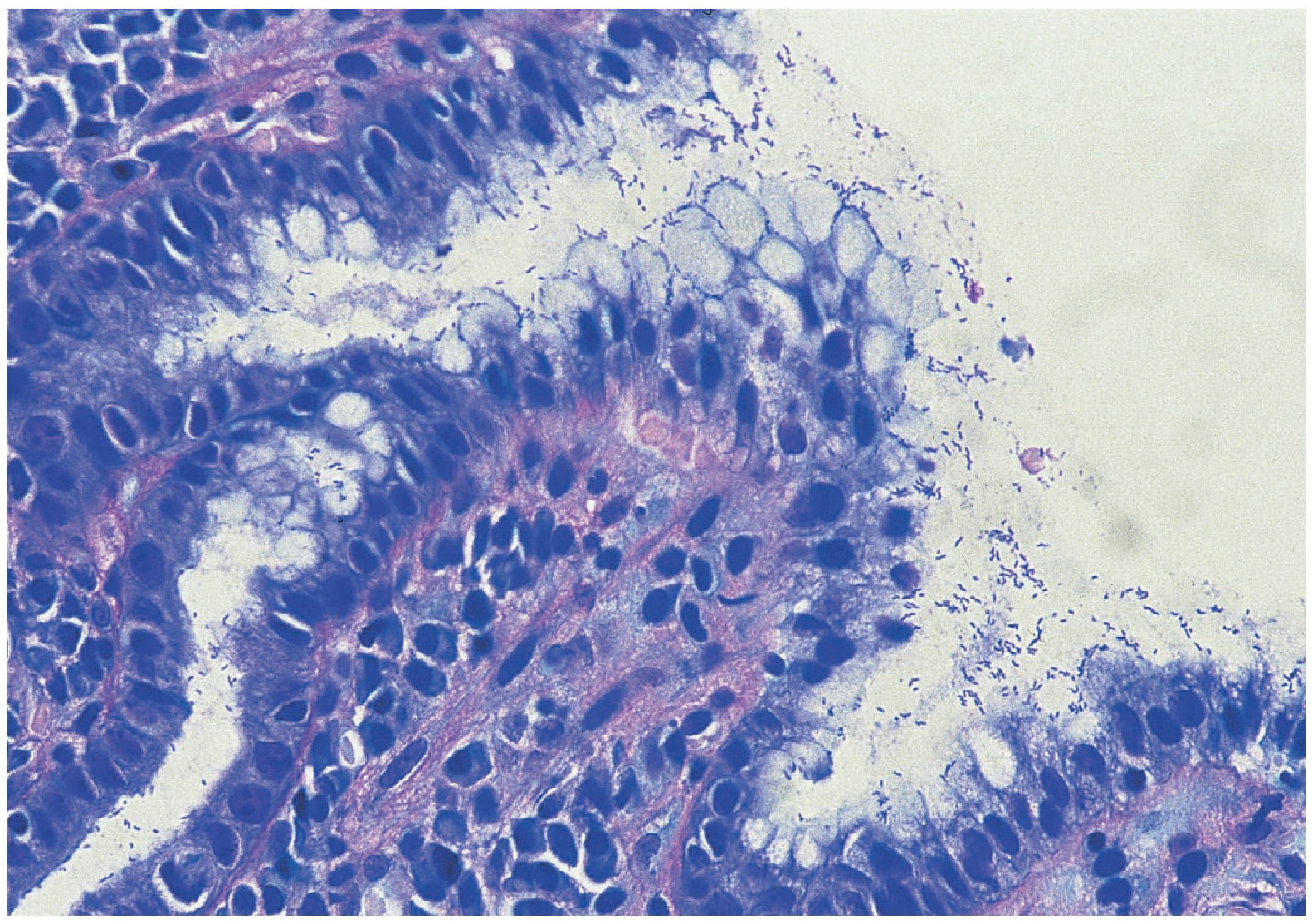
Antral mucosa showing colonisation with H. pylori (modified Giemsa stain) - Bailey & Love's Short Practice of Surgery, 28th Ed.
Conditions Caused by H. pylori (With Associated Symptoms)
| Condition | Key Symptoms |
|---|---|
| Chronic gastritis (Type B) | Often asymptomatic; mild epigastric discomfort, nausea |
| Duodenal ulcer | Epigastric pain relieved by food/antacids, nocturnal pain |
| Gastric ulcer | Epigastric pain worsened by food, weight loss, nausea |
| Gastric MALT lymphoma | Dyspepsia, epigastric pain, weight loss, fatigue |
| Gastric adenocarcinoma | Weight loss, dysphagia, early satiety, anaemia |
H. pylori is associated with ~90% of duodenal ulcers and is responsible for the most common chronic bacterial infection in humans. - Textbook of Family Medicine 9e; Bailey & Love's Short Practice of Surgery 28th Ed.
When to Test for H. pylori
Testing is indicated in patients with:
- Active or previously documented peptic ulcer disease
- Uninvestigated dyspepsia without alarm features (test-and-treat strategy)
- History of gastric MALT lymphoma (MALToma)
- Significant dyspepsia or gastritis on endoscopy
- Early gastric cancer
Key Takeaway
H. pylori infection itself is often silent. Symptoms only emerge once the organism causes gastritis or peptic ulceration. The classic triad to recognise is: epigastric pain + nausea + dyspepsia, especially if symptoms occur at night or on an empty stomach. Alarm symptoms (bleeding, severe pain, weight loss) always warrant urgent investigation.
How is H. pylori infection diagnosed and tested?
Finding Sources
Searching the Web
H pylori diagnosis testing methods urea breath test stool antigen serology endoscopy 2024
Searching PubMed
"Helicobacter pylori" AND diagnosis AND testing
Reading File
Finding Sources
Reading File
Reading File
Reading File
I have rich, detailed content from multiple authoritative textbooks. Here is the complete answer:
H. pylori Infection - Diagnosis and Testing
Tests fall into two broad categories: non-invasive (no endoscopy needed) and invasive (require upper endoscopy and biopsy). The choice depends on whether the patient needs endoscopy for another reason, their age, alarm symptoms, and whether you're confirming eradication or making an initial diagnosis.
Quick Reference: Test Accuracy Summary
(From Harrison's Principles of Internal Medicine 22E)
| Test | Sensitivity / Specificity | Key Notes |
|---|---|---|
| Rapid urease test | 80-95% / 95-100% | False negative with recent PPIs, antibiotics, bismuth |
| Histology | 60-90% / >95% | Provides tissue diagnosis; requires pathologist |
| Culture | 76-90% / 100% | Time-consuming; best for antibiotic susceptibility |
| Urea breath test (UBT) | >95% / >95% | Gold standard for confirmation of cure; detects active infection |
| Stool antigen test | >90% / ~100% | Inexpensive; good for initial Dx and post-treatment confirmation |
| Serology (IgG) | 74% / 59% | Cannot distinguish active vs. past infection; NOT for post-treatment use |
Non-Invasive Tests
1. Urea Breath Test (UBT) - Preferred
The patient ingests urea labeled with either ¹³C or ¹⁴C. If H. pylori is present, its urease breaks the labeled urea down to ammonia + labeled CO₂. The CO₂ is absorbed into the bloodstream and exhaled - it is then measured in a collected breath sample.
- Sensitivity and specificity both >95%
- Detects active, viable infection only
- Considered the gold standard for confirming eradication after treatment
- Provides a more global assessment of the whole stomach than biopsy-based methods
- False negatives occur if taken within 2 weeks of antibiotics, bismuth, or PPIs - hold these before testing
2. Stool Antigen Test (SAT)
Detects H. pylori antigens in stool by immunoassay (monoclonal antibody-based ELISA).
- Sensitivity >90%, specificity approaching 100%
- Accurate for both initial diagnosis and post-eradication confirmation (not earlier than 4 weeks after completing therapy)
- Widely available, inexpensive, and non-invasive
- False negatives with recent antibiotics, PPIs, or bismuth
- A rapid on-site version is now available for point-of-care testing
- AGA and ACG guidelines prefer stool antigen or UBT over serology for active infection
3. Serology (IgG Antibody Testing)
Detects IgG antibodies to H. pylori antigens in blood.
- Sensitivity ~88%, specificity only 70-80%
- Cannot distinguish current from past infection - antibody titers decline slowly after eradication and may persist for years
- Not recommended for confirming eradication success
- Still has a role in low-resource settings or for its strong negative predictive value (a negative test effectively rules out infection)
- Useful in areas of high H. pylori prevalence (>20%) as a cheap first-line screen
- Whole-blood finger-stick tests are less accurate than venipuncture serum tests
Invasive Tests (Endoscopy + Biopsy Required)
These are used when the patient is undergoing upper endoscopy (EGD) anyway - e.g., for alarm symptoms, ulcer follow-up, or suspected malignancy.
4. Rapid Urease Test (CLO Test) - Most Common Biopsy-Based Test
A biopsy is placed into a gel/tablet containing urea and a pH indicator. Urease from H. pylori converts urea to ammonia, raising the pH and causing a colour change from yellow to red, often within 30 minutes.
- Sensitivity 80-95%, specificity 95-100%
- Easy, inexpensive, results within hours
- False negatives with recent PPIs, antibiotics, bismuth, or if biopsy is from the wrong site
- Can be used for both initial diagnosis and post-treatment confirmation
5. Histology - The Gold Standard for Tissue Assessment
Gastric biopsy specimens are processed and stained. Special stains include:
- Modified Giemsa (most common)
- Warthin-Starry silver stain
- Diff-Quik
- Immunohistochemistry
Haematoxylin & eosin (H&E) alone is less sensitive.
- Requires 3-5 biopsies from antrum, corpus, and angularis for reliable results
- Sensitivity 60-90% (depends heavily on number of biopsies, staining, and pathologist experience)
- Specificity >95%
- Unique advantage: directly assesses severity of gastritis, intestinal metaplasia, atrophy, dysplasia, and cancer
- Residual lymphocytic infiltrate may persist after eradication and should not be misinterpreted as ongoing infection
Antral mucosa showing H. pylori colonisation - modified Giemsa stain
6. Culture
Biopsy is plated onto selective media and incubated at 37°C with 5% CO₂ for up to 10 days.
- Specificity 100%, sensitivity 76-90%
- Not routine - reserved for recurrent infection and antibiotic susceptibility testing when second-line therapy has failed
- Time-consuming and expensive; requires specialist lab conditions
7. PCR
Detects H. pylori-specific DNA sequences in gastric tissue, juice, saliva, or stool.
- High sensitivity (93%) and specificity (100%)
- Detects as few as 10 colony-forming units
- Cannot confirm viable organisms - a positive result only means DNA is present
- Risk of false positives from contaminated endoscopes or lab contamination
- Currently a research tool, not standard clinical practice
Utility Table by Clinical Use
(Based on Yamada's Textbook of Gastroenterology, 7th Ed.)
| Test | Primary Diagnosis | Confirms Eradication | Detects Viable Bacteria |
|---|---|---|---|
| Histology | ✓ | ✓ | ✗ |
| Rapid urease test | ✓ | ✓ | ✓ |
| Culture | +/- | +/- | ✓ |
| PCR | ✗ | ✗ | ✗ |
| Urea breath test | ✓ | ✓ | ✓ |
| Serology | ✓ | ✗ | ✗ |
| Stool antigen test | ✓ | ✓ | ✗ |
Practical Approach: Who Gets What Test?
- No alarm symptoms, age <60, no endoscopy planned → Urea breath test or stool antigen test (AGA/ACG guidelines; serology is not recommended)
- Alarm symptoms / suspected malignancy / failure of therapy → Upper endoscopy + rapid urease test + histology (± culture if antibiotic resistance suspected)
- Confirming eradication after treatment → UBT or stool antigen test at least 4 weeks after completing antibiotics and 2 weeks after stopping PPIs
- High H. pylori prevalence area, low resources → Serology acceptable as initial screen due to its good negative predictive value
- Antibiotic resistance / second-line treatment failure → Culture for susceptibility testing
Sources: Schwartz's Principles of Surgery 11e; Harrison's Principles of Internal Medicine 22e; Yamada's Textbook of Gastroenterology 7e; Textbook of Family Medicine 9e; Bailey & Love's Short Practice of Surgery 28e; Robbins & Kumar Pathologic Basis of Disease
This is a shared conversation. Sign in to Orris to start your own chat.