
Answer with images and flow charts whenever needed
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Finding Sources
All four questions are answered comprehensively. Here's a quick guide to what's covered:
What's Included
Q.1 (30 marks) - Laparoscopic Surgery Pathophysiology
- Cardiovascular, respiratory, renal, neurological, metabolic, and DVT effects of pneumoperitoneum
- Flowcharts for each system showing the cascade of changes
- Detailed prevention table covering every major complication
Q.2 (30 marks) - Anal Canal Anatomy + Fistula-in-Ano
- Full surgical anatomy of the anal canal with the dentate line as the central landmark
- Above-vs-below dentate line comparison table (blood supply, drainage, innervation)
- Sphincter anatomy (IAS/EAS/Puborectalis)
- Parks Classification diagram (from Sabiston Textbook) showing all 4 types with incidence percentages
- Goodsall's Rule
- Treatment algorithm flowchart from simple fistulotomy to VAAFT
Q.3 (20 marks) - Professional Hazards + Informed Consent
- Classified hazards: physical (radiation, sharps), biological (HIV/HBV/HCV), chemical, ergonomic, psychological
- All 4 elements of valid informed consent
- Types of consent, exceptions, and medicolegal significance
Q.4 (20 marks) - Esophageal Motility + Neonatal Abdominal Wall Defects
- Step-by-step motility physiology (UES → peristalsis → LES relaxation via VIP/NO)
- Anti-reflux LES mechanism with factors affecting tone
- Omphalocele vs Gastroschisis comparison (sac, location, associations, management)
- Management algorithm from antenatal detection to surgical repair and staged silo closure
Answer according to marks with figures
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
I now have all the content and figures needed. Let me write the full mark-calibrated answers.
MS General Surgery Year 1 - January 2025
Model Answers (Mark-Calibrated)
Q.1 — Pathophysiological Changes in Laparoscopic Surgery and Prevention of Complications
[30 Marks — Long Answer: write ~6 pages worth of depth]
Introduction (2 marks)
Laparoscopic surgery involves creation of a pneumoperitoneum (usually with CO₂ at 12–15 mmHg IAP) and patient positioning. These trigger complex physiological changes across multiple organ systems through two primary mechanisms:
- Direct mechanical effects of raised intra-abdominal pressure (IAP)
- Neuroendocrine stimulation via autonomic pathways and humoral mediators
(Barash Clinical Anesthesia 9e, p.3805)
Pathophysiological Changes (20 marks)
1. CARDIOVASCULAR SYSTEM (5 marks)
Table 44-4 (Barash): Causes of Hemodynamic Changes During Laparoscopy
| Determinant | Effect on Blood Pressure |
|---|---|
| IVC compression (preload) | ↑ or no change |
| Trendelenburg position (preload) | ↑ |
| Reverse Trendelenburg (preload) | ↓ |
| Sympathetic activation (afterload) | ↑↑ |
| CO₂ absorption/hypercarbia | ↑ SVR, tachycardia |
| Vagal stimulation (peritoneal stretch) | ↓ HR, bradycardia |
CARDIOVASCULAR EFFECTS OF PNEUMOPERITONEUM
↑ IAP (12–15 mmHg)
│
┌────┴─────────────────┐
▼ ▼
IVC compression Peritoneal stretch
↓ Venous return │
│ Autonomic activation
│ ┌────────┴────────────┐
▼ ▼ ▼
↓ Preload Sympathetic Parasympathetic
│ (predominates) (vagus nerve)
│ │ │
▼ ▼ ▼
↓ Cardiac ↑ Catecholamines Bradycardia
output ↑ Vasopressin (if peritoneal
│ ↑ Renin-Angiotensin stretch severe)
│ │
▼ ▼
Compensatory ↑ SVR, ↑ MAP,
↑ Heart rate ↑ Afterload
↑ Myocardial O₂ demand
CO₂ Effects on CVS:
- Mild hypercarbia (PaCO₂ 45–50 mmHg): minimal hemodynamic change
- Severe hypercarbia (PaCO₂ 55–70 mmHg): myocardial depression, dysrhythmias, pulmonary vasoconstriction → ↑ RV afterload
- Sympathetic activation simultaneously causes tachycardia, ↑ MAP, ↑ SVR
Net cardiovascular effect: ↑ MAP, ↑ SVR, ↑ PVR, ↑ myocardial O₂ demand, ↑ risk of arrhythmias
2. RESPIRATORY SYSTEM (5 marks)
Table 44-5 (Barash): Pulmonary Changes During Laparoscopy
| Anatomic Displacement | V/Q Mismatch | Altered Lung Mechanics |
|---|---|---|
| Cephalad diaphragm displacement | Lung volume reduction | ↓ Lung compliance |
| Diaphragm elevation | ↑ A-a O₂ gradient | ↑ Lung resistance |
| Risk of endobronchial intubation | ↑ Airway pressure | ↑ Pleural pressure |
CO₂ PNEUMOPERITONEUM
│
┌────┴────────────────────────────┐
▼ ▼
MECHANICAL EFFECTS CO₂ ABSORPTION
│ │
↑ IAP pushes diaphragm CO₂ enters bloodstream
cephalad into thorax │
│ ↑ PaCO₂
┌────┴──────────────┐ (Hypercarbia)
▼ ▼ │
↓ FRC Carina shifts ↑ Minute ventilation
↓ Tidal volume cephalad → required to compensate
↑ Peak airway Risk of endo-
pressure bronchial
│ intubation
▼
↓ Lung compliance
Atelectasis at lung bases
V/Q mismatch
Intrapulmonary shunt
↓ PaO₂ (hypoxemia)
- Steep Trendelenburg further reduces lung compliance by nearly 50%
- Ventilator adjustments (↑ minute ventilation, PEEP) are required intraoperatively
3. RENAL SYSTEM (3 marks)
↑ IAP + ↑ Sympathetic tone + ↑ Vasopressin/ADH
↓
Renal artery vasoconstriction
Renal vein compression
↓
↓ Renal blood flow
↓ GFR
↓ Urine output (oliguria intraoperatively)
↓
Renin-Angiotensin system activated
→ Sodium and water retention
↓
[Reversible after desufflation]
Prolonged/high IAP → Risk of AKI
4. NEUROLOGICAL / ICP EFFECTS (2 marks)
- Trendelenburg position + CO₂-induced cerebral vasodilation → ↑ Intracranial pressure
- Intraocular pressure also rises in steep Trendelenburg (risk of ocular ischemia in robotic surgery)
- Contraindication: Pre-existing raised ICP (head injury, intracranial mass)
5. ENDOCRINE AND METABOLIC EFFECTS (2 marks)
- Stress response: ↑ Cortisol, ↑ Catecholamines, ↑ ADH, ↑ Glucagon
- Hyperglycemia from stress response
- CO₂ absorption → Respiratory acidosis (↓ pH, ↑ PaCO₂)
- Thermal loss: CO₂ gas cools the peritoneal cavity → hypothermia
6. VENOUS THROMBOEMBOLISM RISK (3 marks)
↑ IAP + Trendelenburg/Reverse Trendelenburg
↓
Femoral venous flow velocity ↓ up to 50%
↓
VIRCHOW'S TRIAD ACTIVATED:
┌────────────────────────────────────┐
│ 1. STASIS: Venous pooling in legs │
│ 2. ENDOTHELIAL INJURY: Trocar │
│ manipulation, CO₂ irritation │
│ 3. HYPERCOAGULABILITY: Stress, │
│ immobility, dehydration │
└────────────────────────────────────┘
↓
DVT → Pulmonary Embolism
Prevention of Complications (8 marks)
PREVENTION STRATEGY FOR LAPAROSCOPIC COMPLICATIONS
PREOPERATIVE INTRAOPERATIVE POSTOPERATIVE
│ │ │
┌────┴──────┐ ┌──────┴──────┐ ┌────┴──────┐
▼ ▼ ▼ ▼ ▼ ▼
Patient Consent Technical Monitoring DVT Follow-up
selection care prophylaxis
Specific Prevention Strategies:
| Complication | Prevention |
|---|---|
| Vascular injury | Hasson open technique (preferred); Veress needle - saline drop test; check position before insufflation |
| Bowel/visceral injury | Direct visualization during trocar insertion; identify landmarks; reduce IAP if needed |
| Cardiac arrhythmias | Adequate pre-oxygenation; atropine for bradycardia; desufflate if persistent arrhythmia |
| CO₂ embolism | Low-flow initial insufflation (1 L/min initially); confirm intraperitoneal placement; avoid large venous entry |
| Hypercarbia | Continuous EtCO₂ monitoring; ↑ minute ventilation; limit IAP; deflate at intervals in long cases |
| Hypoxia | PEEP, ↑ FiO₂, careful positioning; deflate diaphragm; check endobronchial intubation |
| DVT/PE | TED stockings, pneumatic compression devices, LMWH (UFH 5000u SC pre-op), early ambulation |
| Hypothermia | Warm humidified CO₂, warm IV fluids, active warming blanket (Bair Hugger) |
| Port-site hernia | Close fascia for all ports >10 mm |
| Subcutaneous emphysema | Confirm trocar positions; limit IAP to ≤15 mmHg; avoid prolonged surgery |
| Shoulder-tip pain | Remove CO₂ at end (low-pressure venting); inject bupivacaine under diaphragm |
| Raised ICP | Avoid steep Trendelenburg; maintain normocarbia; screen head injury patients |
Q.2 — Surgical Anatomy of Anal Canal + Types and Treatment of Fistula-in-Ano
[30 Marks — Long Answer: write ~6 pages worth of depth]
Part A: Surgical Anatomy of the Anal Canal (15 marks)
Overview
The anal canal is the terminal 4 cm (3–4 cm in adults, longer in males) of the gastrointestinal tract. It extends from the anorectal junction (where the rectum passes through the pelvic diaphragm) to the anal verge (perianal skin).
Figure 80.1 — Anatomy of the Anal Canal (Bailey & Love, 28th ed.)
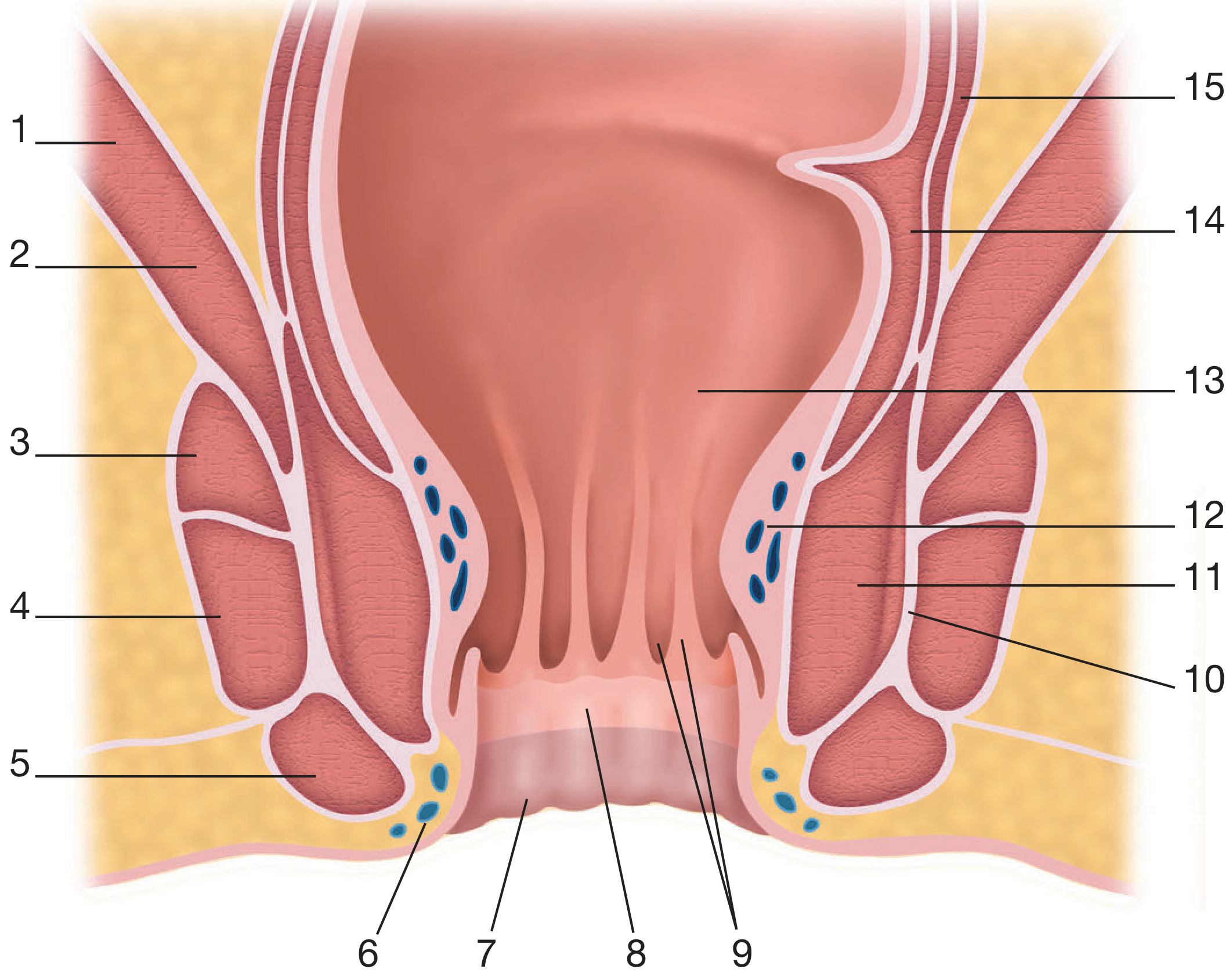
Key numbered structures:
- Levator ani (iliococcygeal)
- Levator ani (puborectalis) 3–5. External anal sphincter (deep, superficial, subcutaneous)
- Inferior hemorrhoidal plexus
- Perianal skin
- Anoderm
- Anal columns and crypts
- Conjoined longitudinal muscle
- Internal anal sphincter
- Superior hemorrhoidal plexus
- Anorectal junction
- Circular rectal muscle
- Longitudinal rectal muscle
The Dentate (Pectinate) Line — Central Landmark
ANORECTAL JUNCTION (palpable as anorectal ring)
│
│ ← 2 cm of columnar-lined canal
▼
═══════════════════════════════════
DENTATE LINE
(embryological junction: ectoderm/endoderm)
═══════════════════════════════════
│
│ ← 2 cm of squamous-lined canal (anoderm)
▼
ANAL VERGE
Above vs Below Dentate Line
| Feature | Above Dentate Line | Below Dentate Line |
|---|---|---|
| Epithelium | Columnar → transitional | Stratified squamous (anoderm) |
| Sensation | Visceral (distension only) | Somatic (pain, touch, temperature) |
| Arterial supply | Superior rectal artery (IMA) | Inferior rectal artery (internal pudendal) |
| Venous drainage | Superior rectal vein → IMV → Portal | Inferior rectal vein → internal pudendal → Systemic |
| Lymph drainage | Internal iliac nodes | Superficial inguinal nodes |
| Hemorrhoids | Internal (painless) | External (painful) |
| Pain from surgery | No pain (visceral) | Painful (somatic) |
This portosystemic anastomosis is clinically important in portal hypertension (anorectal varices).
Columns of Morgagni and Anal Crypts
- 8–12 vertical mucosal folds above the dentate line = Columns of Morgagni
- At the base of each column lies an anal crypt (crypt of Morgagni)
- Anal glands (4–8 in number) open into these crypts
- These glands penetrate the internal sphincter into the intersphincteric space — this is the source of cryptoglandular infection and fistula formation
Sphincter Complex
Figure 80.2 — Puborectalis Muscle (Bailey & Love, 28th ed.)
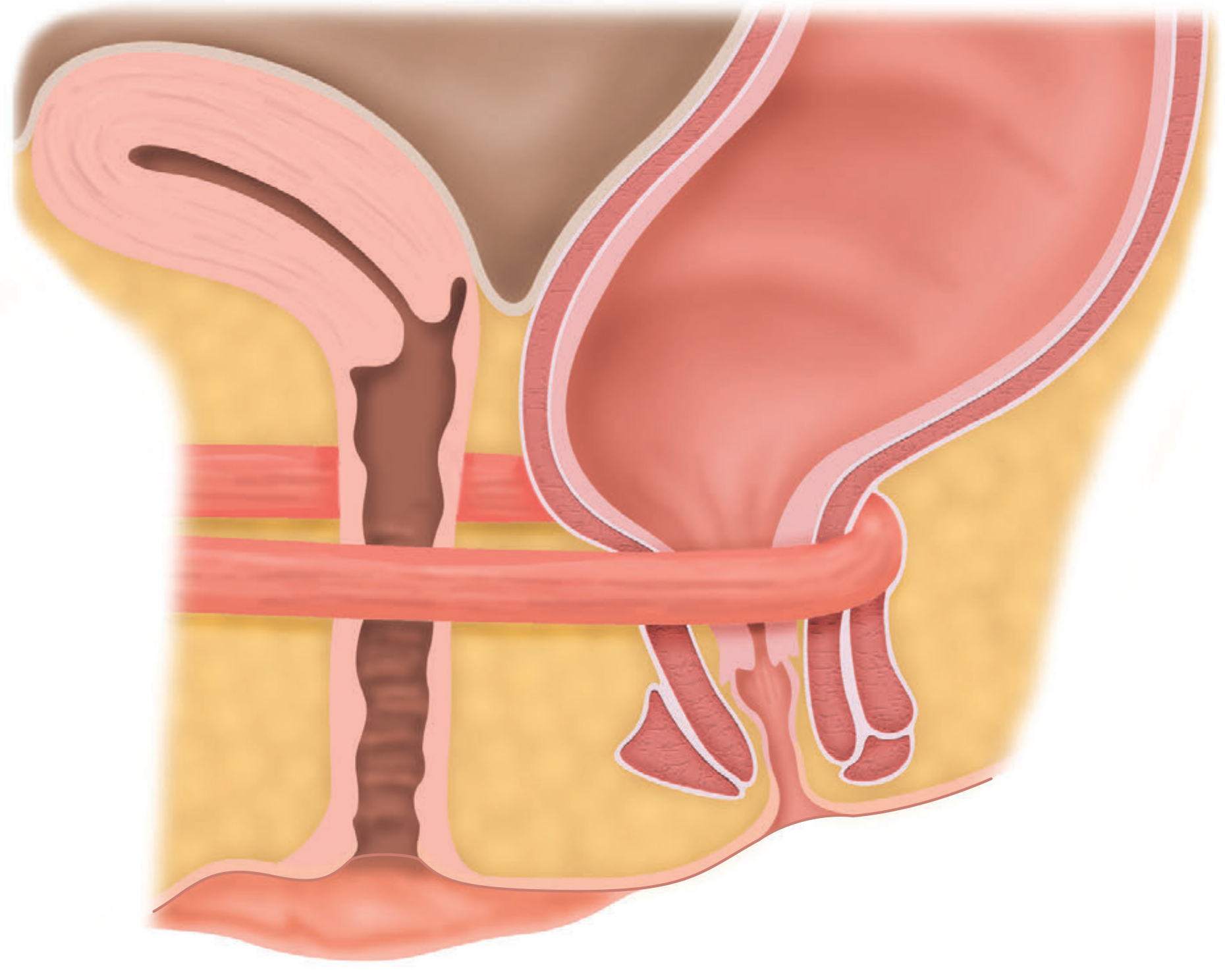
The puborectalis maintains the anorectal angle (~90°), which is the key mechanism for continence.
SPHINCTER ANATOMY
PUBORECTALIS (part of levator ani)
• Origin: pubic symphysis → sling around rectum
• Maintains anorectal angle ~90° at rest
• Relaxes during defecation → straightens angle to ~110–130°
• Nerve: sacral somatic nerves (S3, S4)
INTERNAL ANAL SPHINCTER (IAS)
• Thickened (2–5 mm) distal circular smooth muscle of rectum
• Involuntary (autonomic)
• Pearly white on direct inspection
• Responsible for ~80% of resting anal tone
• Lower border = intersphincteric groove (palpable externally)
• Relaxes via nitric oxide released by non-adrenergic,
non-cholinergic (NANC) intrinsic nerve fibres
EXTERNAL ANAL SPHINCTER (EAS)
• Striated voluntary muscle (red color on inspection)
• Three parts: subcutaneous / superficial / deep
• Nerve: pudendal nerve (S2, S3, S4)
• Responsible for squeeze pressure (voluntary continence)
• Fuses superiorly with puborectalis
CONJOINED LONGITUDINAL MUSCLE
• Between IAS and EAS
• Continuation of outer longitudinal smooth muscle of rectum
• Splits into septa → inserts into perianal skin
• Role: anchor and stabilize anal canal
Blood Supply
- Arteries: Superior rectal a. (branch of IMA) + Middle rectal a. (internal iliac) + Inferior rectal a. (internal pudendal)
- Veins: Superior rectal v. → IMV → portal; Inferior rectal v. → systemic
- Lymphatics: Above dentate line → internal iliac nodes; below → inguinal nodes
- Nerve supply: IAS → autonomic (sympathetic L1/L2, parasympathetic S2–4); EAS → pudendal nerve (S2–4)
Continence Mechanism
CONTINENCE depends on:
1. Intact IAS (resting tone ~80%)
2. Intact EAS (squeeze pressure)
3. Intact puborectalis (anorectal angle)
4. Intact sensory mucosa above and below dentate line
5. Normal stool consistency
6. Normal rectal reservoir compliance
Part B: Types and Treatment of Fistula-in-Ano (15 marks)
Pathogenesis
Normal anal gland
↓ (blocked crypt opening)
Infection in intersphincteric space
↓
PERIANAL ABSCESS
(intersphincteric / ischiorectal / supralevator)
↓ (50% develop fistula after drainage)
FISTULA-IN-ANO
= Chronic epithelialized track between:
INTERNAL OPENING (at dentate line, in anal crypt)
↕
EXTERNAL OPENING (perianal skin)
Parks Classification (with incidence)
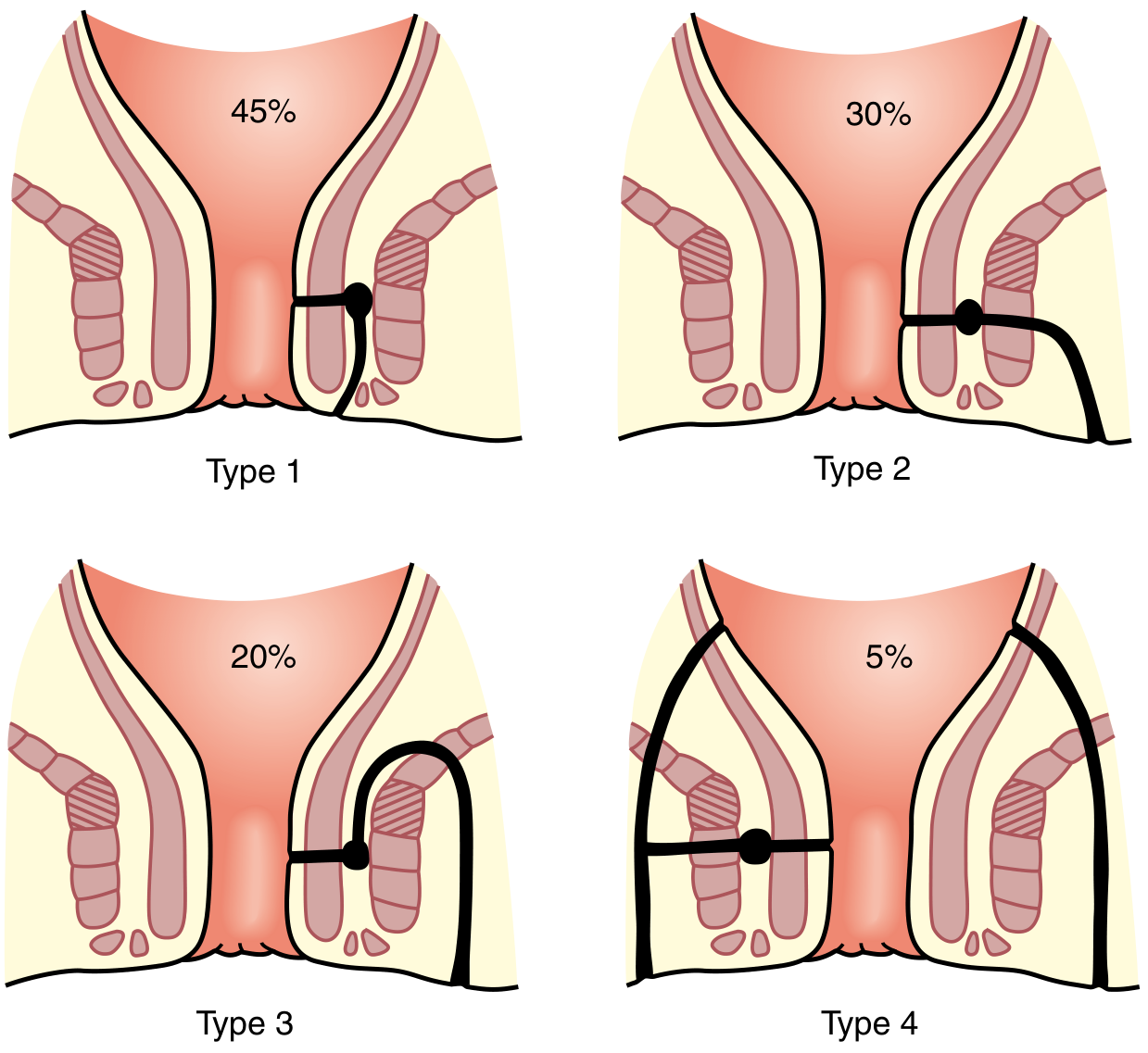
(FIGURE 97.16 — Sabiston Textbook of Surgery, 21st ed.)
| Type | Name | Track Path | Incidence |
|---|---|---|---|
| Type 1 | Intersphincteric | Between IAS and EAS; exits perianal skin | 45% |
| Type 2 | Transsphincteric | Crosses both IAS and EAS; through ischioanal fossa | 30% |
| Type 3 | Suprasphincteric | Goes up over puborectalis, curves down through levator | 20% |
| Type 4 | Extrasphincteric | From rectal wall, bypasses sphincter mechanism entirely | 5% |
Also: Superficial/subcutaneous - below both sphincters; most easily treated.
Goodsall's Rule (predicts internal opening location)
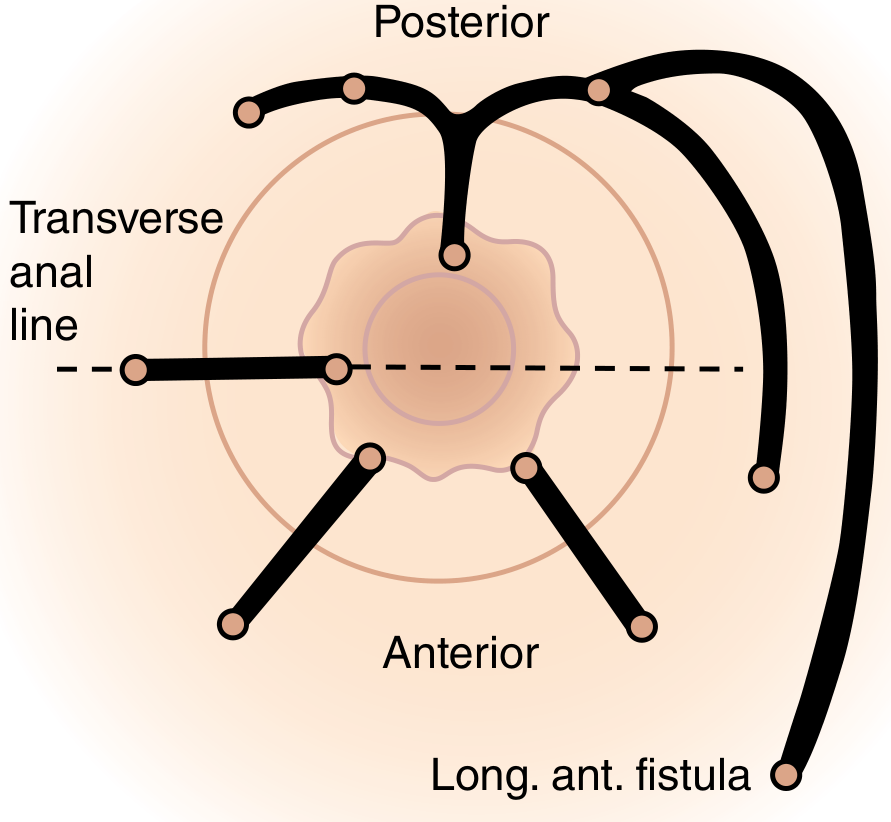
(FIGURE 97.17 — Sabiston Textbook of Surgery, 21st ed.)
Rule:
- Posterior external opening → Curved track → Internal opening at 6 o'clock (posterior midline)
- Anterior external opening → Straight/radial track → Internal opening directly behind it
- Exception: Long anterior fistula (>3 cm from anal verge) = behaves like a posterior fistula (curved track)
Clinical Assessment
- History: Cyclical pain, swelling, spontaneous drainage with relief
- Examination: Cordlike tract palpable in perianal skin; single or multiple external openings
- "Watering can perineum" (multiple openings) → Crohn's disease
- MRI with fistula protocol: gold standard for complex/recurrent fistulas (T2-weighted shows track as hyperintense)
- Examination under anesthesia (EUA): definitive assessment + treatment
MRI of Anal Fistula
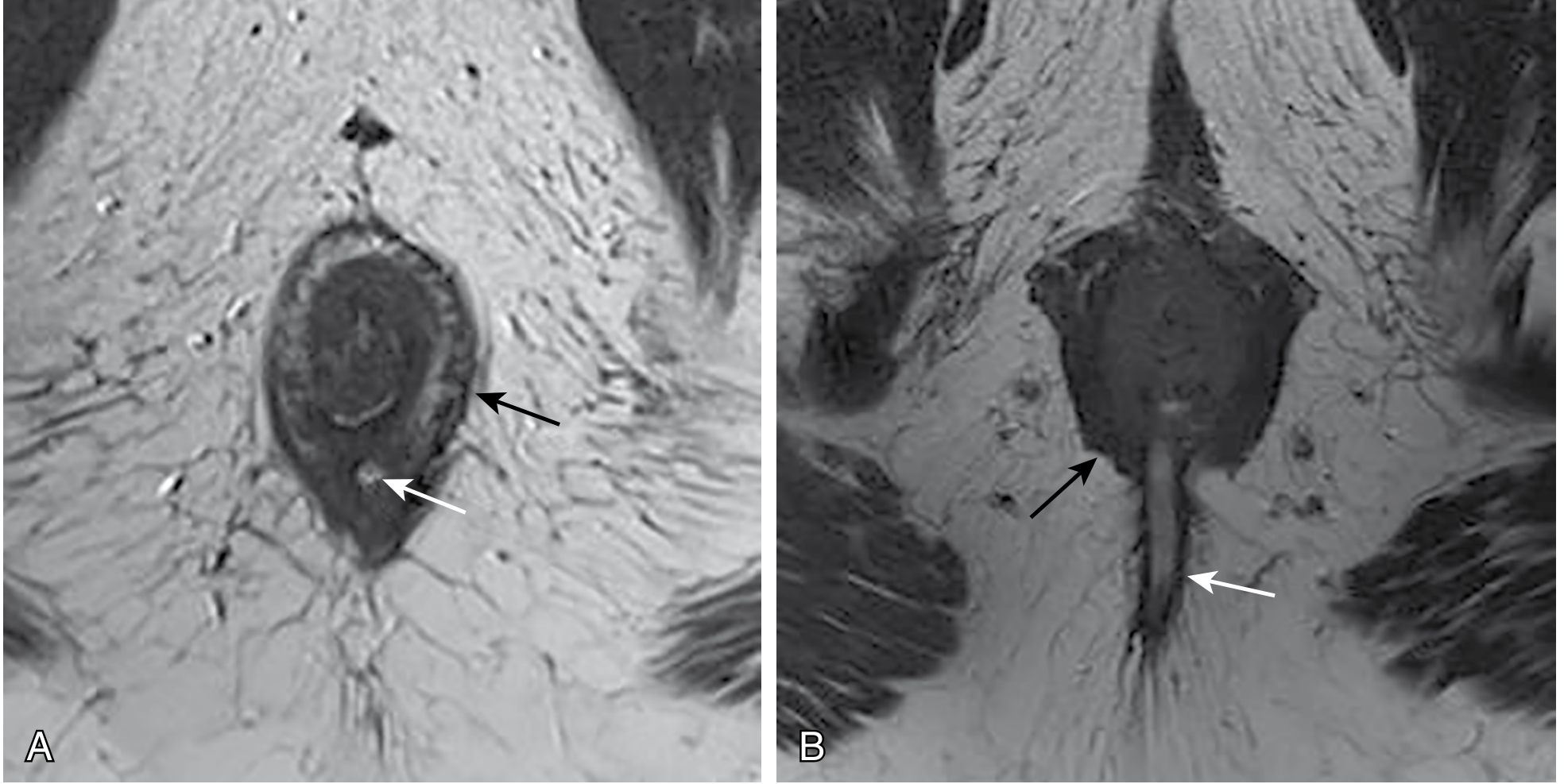
(FIGURE 97.15 — Sabiston: A = intersphincteric fistula; B = transsphincteric fistula)
Treatment — Goals
- Treat any undrained infection
- Define fistula anatomy
- Remove/ablate epithelialized tract
- Avoid/minimize fecal incontinence (most important)
- Prevent recurrence
Treatment Algorithm
FISTULA-IN-ANO TREATMENT ALGORITHM
│
┌─────────┴────────────────────────┐
▼ ▼
SIMPLE FISTULA COMPLEX FISTULA
(<30% EAS involved) (>30% EAS; suprasphincteric;
Low intersphincteric extrasphincteric; recurrent;
Superficial Crohn's; anterior in female)
│ │
▼ ┌─────┴───────────────────┐
FISTULOTOMY ▼ ▼
(lay-open) STAGE 1: SPHINCTER-
│ DRAINING SETON PRESERVING
▼ (silastic loop) TECHNIQUE
Healing by │ (primary)
secondary ▼ │
intention Inflammation settles ┌─────┴──────────┐
(4–6 weeks) Tract matures ▼ ▼
Recurrence rate │ Mucosal LIFT
2–8% ┌──────────┴──────────┐ Advancement procedure
▼ ▼ Flap
STAGE 2: CUTTING
Definitive SETON
repair (gradual
tightening)
Detailed Treatment Options
| Procedure | Indication | Sphincter Division | Incontinence Risk |
|---|---|---|---|
| Fistulotomy | Low simple fistula (<1/3 EAS) | Yes (but minimal) | <5% |
| Draining seton | High/complex; staging; Crohn's | No | Minimal (drainage only) |
| Cutting seton | After staging; gradual division | Yes (slow) | Similar to fistulotomy |
| Mucosal advancement flap | High transsphincteric | No | 0–10% |
| LIFT (Ligation of Intersphincteric Fistula Tract) | Intersphincteric component | No | Very low |
| Fibrin glue / Anal fistula plug | Complex; poor surgical risk | No | Very low (high recurrence ~50%) |
| VAAFT (Video-assisted) | Complex/recurrent | No | Minimal |
Key principle: The higher the fistula = the more sphincter at risk = the more sphincter-preserving the approach must be.
Q.3 — (A) Professional Hazards of Surgeon (B) Informed Consent
[20 Marks — Short Answer: 10 marks each]
3A. Professional Hazards of a Surgeon (10 marks)
Surgeons face unique occupational risks that can be classified into:
PROFESSIONAL HAZARDS OF SURGEONS
│
┌───────────┼─────────────────────┐
▼ ▼ ▼
PHYSICAL/ BIOLOGICAL/ PSYCHOLOGICAL/
ERGONOMIC CHEMICAL OCCUPATIONAL
│ │ │
▼ ▼ ▼
• Radiation • Bloodborne • Burnout
• Sharps injury pathogens • Sleep deprivation
• Musculo- • Surgical smoke • Depression/suicide
skeletal • Latex allergy • Medicolegal stress
• Noise • Anesthetic • Work-life imbalance
• Laser gases
• Fatigue
A. Physical / Ergonomic Hazards
| Hazard | Specific Risk | Prevention |
|---|---|---|
| Radiation (fluoroscopy, C-arm) | Cataracts, thyroid cancer, leukemia, reproductive effects | Lead apron, thyroid collar, dosimeter badge, distance (inverse square law), minimize exposure time |
| Sharps/Needlestick injuries | HIV (0.3%), HBV (30%), HCV (3%) per exposure | No-touch/no-pass technique, double gloving, blunt suture needles, sharps bin disposal |
| Musculoskeletal strain | Back/neck pain, shoulder injury (esp. laparoscopic surgery with awkward posture) | Ergonomic table height, monitor positioning, posture training, instrument design |
| Laser injury | Retinal/corneal burns, skin burns | Appropriate wavelength-specific eyewear, warning signs, interlocks |
| Surgical smoke (electrocautery, laser) | Carcinogens, viral particles (HPV DNA found), respiratory irritants | Smoke evacuator, high-filtration masks (N95) |
| Noise | Hearing loss (chronic exposure to OR equipment alarms) | Hearing protection, sound insulation |
B. Biological / Chemical Hazards
| Hazard | Risk | Prevention |
|---|---|---|
| HIV | 0.3% seroconversion per percutaneous exposure | Universal precautions; PEP (antiretroviral) within 72 hours |
| Hepatitis B | 30% per exposure (unvaccinated) | Mandatory vaccination; HBIg + booster if exposed and unvaccinated |
| Hepatitis C | 3% per exposure; no vaccine | Surveillance; treat with direct-acting antivirals if infected |
| Latex allergy | Contact dermatitis → anaphylaxis | Latex-free gloves; allergy testing; latex-safe environment |
| Anesthetic gases (N₂O, volatile agents) | Reproductive toxicity, hepatotoxicity, neurotoxicity (chronic exposure) | Properly maintained gas scavenging systems; regular OR ventilation monitoring |
| Chemical disinfectants | Skin/respiratory sensitization (formaldehyde, glutaraldehyde) | PPE, adequate ventilation |
C. Psychological / Occupational Hazards
- Burnout: High workload, emotional burden from adverse outcomes, performance pressure
- Sleep deprivation: Long duty hours → impaired cognition, ↑ error rates, motor impairment
- Depression and suicide: Surgeons have higher suicide rates than general population (especially female surgeons)
- Medicolegal stress: Fear of litigation, impact of complaints on career
- Compassion fatigue: Repeated exposure to patient suffering
3B. Informed Consent (10 marks)
Definition
Informed consent is the process by which a competent patient, after receiving adequate and comprehensible information, voluntarily authorizes a proposed medical intervention. It is both a legal requirement and an ethical obligation founded on the principle of patient autonomy.
Four Essential Elements
┌─────────────────────────────────────────────┐
│ VALID INFORMED CONSENT │
│ │
│ 1. DISCLOSURE (Information) │
│ • Diagnosis & indication for surgery │
│ • Nature of proposed procedure │
│ • Expected benefits │
│ • Material risks & complications │
│ • Available alternatives (incl. none) │
│ • Consequences of refusal │
│ │
│ 2. CAPACITY (Competence) │
│ Patient must be able to: │
│ • Understand information given │
│ • Retain it long enough to decide │
│ • Weigh up pros and cons │
│ • Communicate a clear decision │
│ │
│ 3. VOLUNTARINESS │
│ Decision must be free from: │
│ • Coercion or duress │
│ • Undue influence (from family, │
│ doctor, or institution) │
│ │
│ 4. AUTHORIZATION │
│ • Patient actively agrees │
│ • Written signature preferred │
│ for surgical procedures │
└─────────────────────────────────────────────┘
Types of Consent
| Type | Description | Surgical Context |
|---|---|---|
| Written (expressed) | Signed consent form | All elective operations |
| Verbal (expressed) | Patient verbally agrees | Minor procedures, change of plan in OR |
| Implied | Consent inferred from behavior | Presenting for procedure (e.g. blood draw) |
| Emergency | Life-threatening situation; patient incapacitated; assumed consent | Trauma, unconscious patient |
| Proxy/Surrogate | Next of kin/legal guardian decides | Children, mentally incapacitated adults |
Standards of Disclosure
- Bolam standard (professional/doctor-centric): what a reasonable body of medical practitioners would disclose
- Rogers v Whitaker standard (patient-centric): what a reasonable patient would consider significant — now the legally preferred standard
- Sidaway (UK) / Montgomery v Lanarkshire (2015): shifted to patient standard — ALL material risks must be disclosed
Exceptions to Consent
- Emergency - immediate life threat with no time for consent process
- Incompetence - legally incapacitated patient; proxy/court-appointed guardian required
- Waiver - patient voluntarily waives right to information
- Therapeutic privilege - disclosure would cause significant psychological harm (very limited; controversial)
Medicolegal Consequences of Failure
INADEQUATE INFORMED CONSENT
↓
Patient suffers complication
that was NOT disclosed
↓
Medicolegal action
↓
┌───────┴──────────┐
▼ ▼
CIVIL liability DISCIPLINARY action
(negligence/ by Medical Council
battery) (license suspension)
Compensation
Q.4 — (A) Physiology of Esophageal Motility (B) Neonatal Abdominal Wall Defects
[20 Marks — Short Answer: 10 marks each]
4A. Physiology of Esophageal Motility (10 marks)
Structure
The esophagus is a muscular tube ~25 cm long. Its wall has two muscle layers:
- Upper 1/3 → Striated muscle (voluntary)
- Middle 1/3 → Mixed (striated + smooth)
- Lower 1/3 → Smooth muscle (involuntary)
Two sphincters:
- Upper Esophageal Sphincter (UES) = cricopharyngeus muscle; resting pressure ~60 mmHg
- Lower Esophageal Sphincter (LES) = smooth muscle; resting pressure 15–25 mmHg (higher than stomach = anti-reflux)
Step-by-Step Motility Physiology (Costanzo Physiology 7e, p.356)
ESOPHAGEAL MOTILITY — SEQUENTIAL STEPS
STEP 1: SWALLOWING REFLEX INITIATED
Bolus in pharynx
↓
Nucleus tractus solitarius (medulla) activated
↓
Coordinated: soft palate elevation + larynx closure
+ inhibition of respiration
STEP 2: UES OPENS
Cricopharyngeus (UES) relaxes
↓
Bolus enters upper esophagus
↓
UES closes → prevents pharyngeal reflux
STEP 3: PRIMARY PERISTALSIS
Swallowing reflex triggers sequential circular contractions
↓
High-pressure zone BEHIND bolus pushes it distally
Speed: 2–4 cm/sec
Complete transit: 8–10 seconds
Mediated by: Vagal efferents → Acetylcholine (excitatory)
↓
Bolus approaches LES...
STEP 4: LES RELAXES (receptive relaxation)
Peptidergic fibers in vagus nerve activated
↓
Release VIP (Vasoactive Intestinal Peptide) + Nitric Oxide
↓
LES smooth muscle relaxes
LES pressure drops from 15–25 mmHg → near zero
↓
SIMULTANEOUSLY: Orad stomach relaxes (receptive relaxation)
→ reduces gastric pressure → facilitates bolus entry
STEP 5: BOLUS ENTERS STOMACH
Bolus passes through LES → enters orad stomach
↓
LES immediately re-contracts → returns to high resting tone
→ PREVENTS GASTROESOPHAGEAL REFLUX
STEP 6: SECONDARY PERISTALSIS (if needed)
If primary wave fails to clear esophagus:
Local distension sensed by enteric nervous system
↓
Secondary peristaltic wave starts at point of distension
Travels downward (independent of swallowing reflex)
Neuromuscular Control Summary
| Event | Neural pathway | Mediator |
|---|---|---|
| UES relaxation | Vagus (IX, X cranial nerves) | Motor neurons to cricopharyngeus |
| Primary peristalsis | Vagal efferents | Acetylcholine (cholinergic excitation) |
| LES relaxation | Vagal peptidergic fibers | VIP + Nitric Oxide |
| LES re-contraction | Myogenic tone + cholinergic | Acetylcholine, Gastrin |
| Secondary peristalsis | Enteric nervous system (myenteric plexus) | Local distension reflex |
Anti-Reflux Function of LES
The esophagus sits in the thorax (negative intrathoracic pressure), while the stomach has positive intra-abdominal pressure. The LES maintains a pressure gradient to prevent acid reflux:
| Increases LES tone (anti-reflux) | Decreases LES tone (pro-reflux) |
|---|---|
| Gastrin, Motilin | Progesterone, Secretin, CCK |
| Acetylcholine, Metoclopramide | Fatty meals, Chocolate, Coffee |
| High protein diet | Smoking, Alcohol |
| Alkaline pH | Calcium channel blockers, Nitrates |
4B. Neonatal Abdominal Wall Defects (10 marks)
The two main congenital abdominal wall defects are Gastroschisis and Omphalocele (Exomphalos).
Clinical Photographs from Textbook
Omphalocele — intestines and liver visible inside translucent sac; umbilical cord attaches to sac:

(Figure 101.2 — Mulholland & Greenfield's Surgery, 7th ed.)
Comparison Table
| Feature | Gastroschisis | Omphalocele |
|---|---|---|
| Defect location | Right of umbilicus (paraumbilical) | Central — at umbilicus (midline) |
| Sac | No sac (bowel directly exposed) | Has a sac (peritoneum + amnion + Wharton's jelly) |
| Umbilical cord | Normal, left of defect | Inserts INTO the sac |
| Bowel appearance | Thickened, matted, edematous (exposed to amniotic fluid) | Normal (protected by sac) |
| Associated anomalies | Rare (~10%; intestinal atresia) | Common (50–70%; cardiac, chromosomal) |
| Chromosomal anomalies | Rare | Trisomy 13, 18, 21; Beckwith-Wiedemann syndrome |
| Incidence | 1 in 2,000–4,000 | 1 in 6,000–10,000 |
| Maternal age | Young mothers (teenage) | Older mothers |
| Liver herniation | Distinctly unusual | Common in giant omphalocele |
| Malrotation | Present | Present |
Embryology
Gastroschisis: Right umbilical vein resorption during development leaves a weakness in the abdominal wall → bowel evisceration through this defect. Considered a mechanical/vascular defect, NOT a global embryological failure.
Omphalocele: Failure of lateral body fold fusion at week 10 (when midgut normally returns from yolk sac). A defect in embryogenesis → global failure of anterior wall closure.
Management Algorithm
ANTENATAL DIAGNOSIS (USS at 12–20 weeks)
↓
┌──────────┴────────────────┐
▼ ▼
GASTROSCHISIS OMPHALOCELE
│ │
│ Karyotyping +
│ Fetal echo
│ (associated anomalies)
▼ ▼
DELIVERY (controlled, tertiary centre)
↓
AT BIRTH — IMMEDIATE MANAGEMENT:
• Airway, Breathing, Circulation
• NG tube (gastric decompression)
• IV access + fluid resuscitation
(gastroschisis: LARGE fluid losses from exposed bowel)
• Bowel protection:
GASTROSCHISIS → silastic bowel bag or
moist warm saline gauze
OMPHALOCELE → keep sac INTACT (do not rupture)
• Prevent hypothermia (warm environment)
• IV antibiotics
↓
SURGICAL REPAIR
┌──────────┴────────────────┐
▼ ▼
PRIMARY CLOSURE STAGED REPAIR
(if bowel fits & (if giant omphalocele or
no abdominal edematous/bulky bowel in
compartment syndrome) gastroschisis)
│ │
▼ ▼
Watch peak airway SILO reduction
pressure during closure (gravity-assisted
(↑ → abdominal daily reduction)
compartment syndrome) ↓
Definitive closure
when bowel fits
↓
POSTOPERATIVE CARE
• Ventilator support
• TPN (especially gastroschisis — bowel dysmotility for weeks)
• Monitor for bowel function return
• Treat sepsis
• Gastroschisis: bowel function may take 2–4 weeks to normalize
• Omphalocele: relatively prompt return of bowel function
Key Complications
| Complication | More in | Management |
|---|---|---|
| Abdominal compartment syndrome | Both | Monitor bladder pressure + peak airway pressure; stage the repair |
| Prolonged ileus / dysmotility | Gastroschisis | TPN; patience; bowel may take 4 weeks |
| Sepsis | Both | Broad-spectrum antibiotics |
| Short bowel syndrome | Gastroschisis (volvulus in utero) | TPN long-term; bowel lengthening procedures |
| Associated cardiac defects | Omphalocele | Echo; cardiac surgery if needed |
| Chromosomal anomalies | Omphalocele | Karyotyping; counseling |
Quick Revision Summary
| Q | Marks | Key headings to cover |
|---|---|---|
| Q1 Laparoscopic Surgery | 30 | CVS (5) + Respiratory (5) + Renal (3) + Neuro (2) + Metabolic (2) + DVT (3) + Prevention table (10) |
| Q2 Anal Canal + Fistula | 30 | Anatomy: dentate line, sphincters, blood supply (15) + Parks classification diagram, Goodsall's rule, treatment (15) |
| Q3A Professional Hazards | 10 | Physical, biological, chemical, psychological hazards with prevention |
| Q3B Informed Consent | 10 | 4 elements, types, exceptions, medicolegal implications |
| Q4A Esophageal Motility | 10 | UES → primary peristalsis → LES (VIP/NO) → secondary peristalsis; anti-reflux mechanism |
| Q4B Neonatal AWDs | 10 | Gastroschisis vs Omphalocele comparison table + management algorithm |
Sources: Sabiston Textbook of Surgery 21e; Bailey & Love 28e; Barash Clinical Anesthesia 9e; Mulholland & Greenfield 7e; Costanzo Physiology 7e
Role of AI in General surgery Recent advances
Searching PubMed
artificial intelligence general surgery clinical applications
Searching the Web
AI artificial intelligence general surgery recent advances 2024 2025
Finding Sources
Your credits are exhausted. You can purchase a top-up or subscribe to a plan to continue using Orris. If you're already subscribed, your daily credits will reset tomorrow.
This is a shared conversation. Sign in to Orris to start your own chat.