Capnography and capnometry full details for md exam answer 15 marks from fishman and Murray only
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
Loading Image
Loading Image
Reading File
I now have rich content from both textbooks with the capnogram images. I have enough material to write a comprehensive 15-mark MD exam answer. Let me compose it now.
Capnography and Capnometry — Comprehensive MD Examination Answer (15 Marks)
Sources: Fishman's Pulmonary Diseases and Disorders (5e) & Murray & Nadel's Textbook of Respiratory Medicine (7e)
1. Definitions and Distinction
Capnometry is the quantitative measurement of carbon dioxide (CO₂) concentration during the respiratory cycle, expressed as a numeric value (PCO₂ in mm Hg or %). Capnography is capnometry combined with a continuous graphical display of that CO₂ waveform over time — the tracing produced is called a capnogram. A device measuring only numbers (no waveform) is a capnometer; one that also displays the waveform is a capnograph.
"The measurement of carbon dioxide during the respiratory cycle is called capnometry, and the display of the analog waveform is called a capnogram." — Murray & Nadel's Textbook of Respiratory Medicine, p. 738
2. Physiological Basis
During expiration, exhaled gas passes through the airway in a predictable sequence:
- Dead-space gas (anatomic dead space, no CO₂) exits first
- Mixed gas (dead space + alveolar gas) follows
- Pure alveolar gas exits last
This produces the characteristic three-phase capnogram. CO₂ is continuously produced by cellular metabolism, transported as dissolved CO₂, carbamino compounds, and bicarbonate in the blood, and eliminated by the lungs. The end-tidal PCO₂ (PETCO₂) under normal physiologic conditions approximates alveolar PCO₂, which in turn approximates arterial PaCO₂ (normally PaCO₂ – PETCO₂ ≈ 2–5 mm Hg).
"Under normal physiologic conditions, alveolar PCO₂ is the same as PaCO₂ and can be estimated by measuring end-tidal CO₂ (PETCO₂)." — Fishman's Pulmonary Diseases and Disorders, p. 2596
3. Instrumentation and Methods
A. Infrared Spectrometry (Most Common)
CO₂ absorbs infrared light at a wavelength of 4.3 µm. The sensor measures the difference in infrared absorbance between a reference cell and the sample cell. This technique is accurate, rapid, and widely available. Care must be taken to:
- Calibrate regularly
- Avoid interference by nitrous oxide, acetylene, and carbon monoxide (all absorb similar wavelengths)
B. Mass Spectrometry
Can measure all respiratory gases (CO₂, O₂, N₂) and anesthetic gases simultaneously. Very rapid but expensive. Used in pulmonary/exercise laboratories and operating rooms where gases from multiple patients may be tested in sequence.
C. Colorimetric Devices
Qualitative, color-change devices that detect a range of PETCO₂ (e.g., 0–10 mm Hg vs. >35 mm Hg) rather than an exact number. Useful for confirming endotracheal tube placement; accuracy is comparable to quantitative capnography for this purpose.
D. Sampling Configurations
- Sidestream: Gas aspirated from airway via a thin catheter to a remote sensor. Allows use with non-intubated patients; slight delay.
- Mainstream (in-line): Sensor placed directly in the airway circuit. Faster response; adds dead space.
"Quantitative devices measure the precise PETCO₂ as either a number (capnometry) or a number and a waveform (capnography)." — Roberts & Hedges
4. The Normal Capnogram — Waveform Analysis
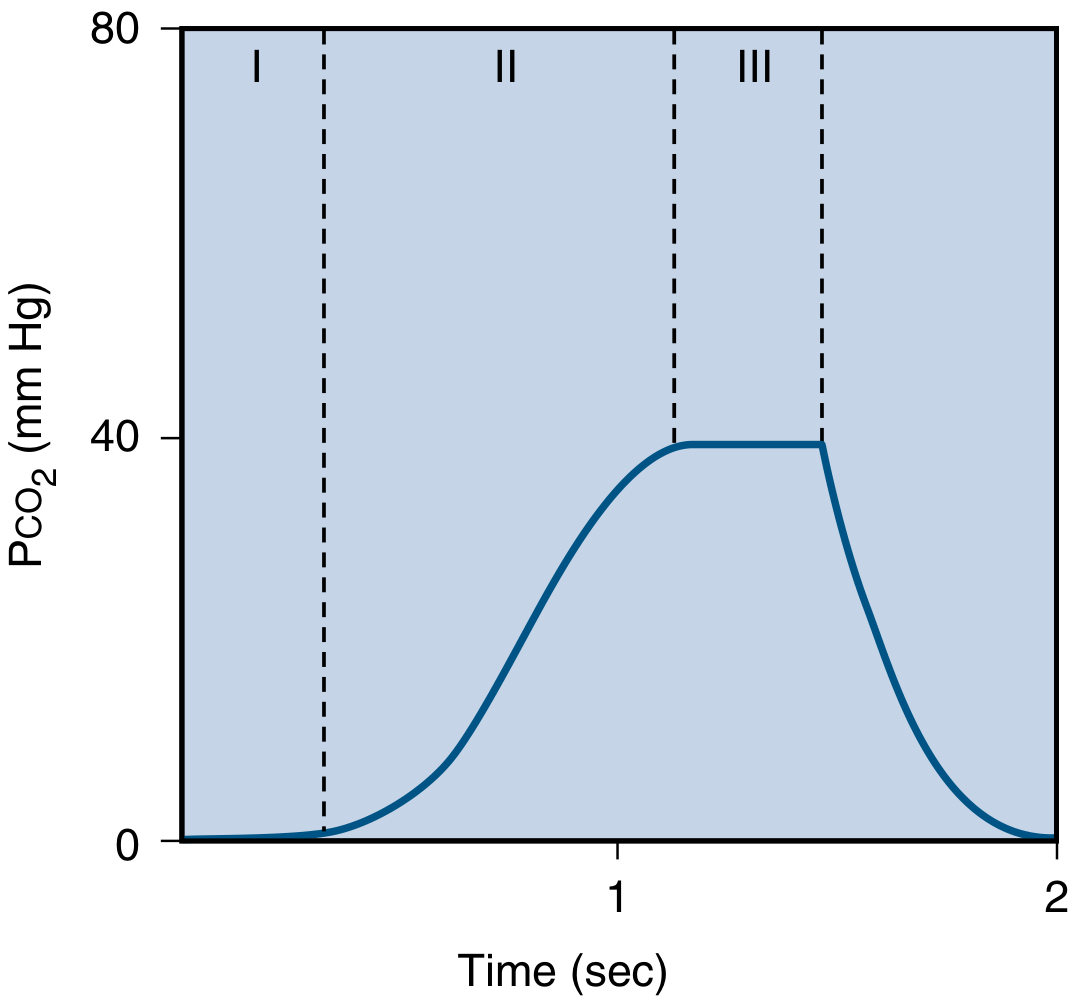
Normal capnogram from Murray & Nadel, eFig. 31.23. During inspiration, PCO₂ = 0. Three expiratory phases are shown.
The waveform has three expiratory phases analogous to the single-breath nitrogen washout:
| Phase | Equivalent in N₂ washout | Physiological basis | PCO₂ |
|---|---|---|---|
| Phase I (baseline) | Phase I | Dead-space gas (anatomic dead space); no CO₂ | 0 mm Hg |
| Phase II (rising slope) | Phase II | Mixing of dead-space and alveolar gas; rapid CO₂ rise | Rising |
| Phase III (alveolar plateau) | Phase III | Gas entirely from CO₂-containing alveoli; near-flat plateau | ~38–42 mm Hg |
| End-tidal point | — | PCO₂ at end of plateau = PETCO₂ | ~38–40 mm Hg |
| Phase 0 (inspiration) | — | Fresh gas inspiration; CO₂ falls rapidly to zero | Returns to 0 |
"The PCO₂ at the end of the 'alveolar plateau' is called the end-tidal PCO₂ (comparable to phase III in the single-breath nitrogen washout test)." — Murray & Nadel, eFig. 31.23 legend
Normal PETCO₂: 35–45 mm Hg (approximately 5% of atmospheric pressure = 38 mm Hg).
5. The PaCO₂ – PETCO₂ Gradient
Normally, PETCO₂ is 2–5 mm Hg lower than PaCO₂. This gradient increases whenever dead space increases:
Conditions that increase the PaCO₂ – PETCO₂ gradient:
- Increased anatomic dead space (added ventilator tubing, tracheostomy)
- Increased alveolar dead space — units ventilated but not perfused:
- Pulmonary embolism
- Pulmonary vascular disease
- Low cardiac output states
- ARDS (acute respiratory failure)
- Abnormally high respiratory rate — insufficient time for equilibration
"This relationship does not hold true in states with significant physiologic dead space, such as ARF, pulmonary embolism, pulmonary vascular disease, or low cardiac output states, during which PETCO₂ may underestimate PaCO₂." — Fishman's Pulmonary Diseases and Disorders, p. 2596
6. Dead Space Calculation Using Capnography
The modified Bohr equation allows dead space fraction calculation:
$$\frac{V_D}{V_T} = \frac{PaCO_2 - P\bar{E}CO_2}{PaCO_2}$$
Where:
- V_D/V_T = dead space to tidal volume ratio
- PaCO₂ = arterial PCO₂ (from blood gas)
- PēCO₂ = mean expired PCO₂ (measured by capnography or metabolic monitor)
This can be calculated in mechanically ventilated patients using capnography to measure mean expired CO₂, avoiding the need for complex metabolic monitors.
"The modified Bohr equation allows calculation of the dead space to tidal volume (VD/VT) ratio... The latter can be measured using a metabolic monitor that collects expired gas or using capnography in mechanically ventilated patients." — Fishman's Pulmonary Diseases and Disorders, p. 2596
7. Clinical Applications
A. Confirmation of Endotracheal Tube (ETT) Placement
This is the most critical immediate application. Esophageal intubation produces no CO₂ signal (or only a few breaths of gastric CO₂ that rapidly disappear). A sustained PETCO₂ signal confirms tracheal placement. Methods include capnography, capnometry, and colorimetric devices.
"ETT placement can be confirmed... by determining the presence of PETCO₂, using capnography or capnometry." — Fishman's Pulmonary Diseases and Disorders, p. 2597
B. Monitoring During Cardiopulmonary Resuscitation (CPR)
PETCO₂ serves as a real-time indicator of CPR quality:
- During cardiac arrest, CO₂ delivery to the lungs depends entirely on cardiac output generated by chest compressions
- Higher PETCO₂ during CPR correlates with better cardiac output and survival
- Sudden rise in PETCO₂ indicates return of spontaneous circulation (ROSC)
- PETCO₂ <10 mm Hg despite optimal CPR predicts poor prognosis
"Evidence exists to support the use of PETCO₂ in cardiac arrest, as a measure of cardiopulmonary resuscitation (CPR) quality, to identify return of spontaneous circulation (ROSC), and to help guide prognosis." — Fishman's Pulmonary Diseases and Disorders, p. 2596
C. Detecting Ventilator Problems and Life-Threatening Events
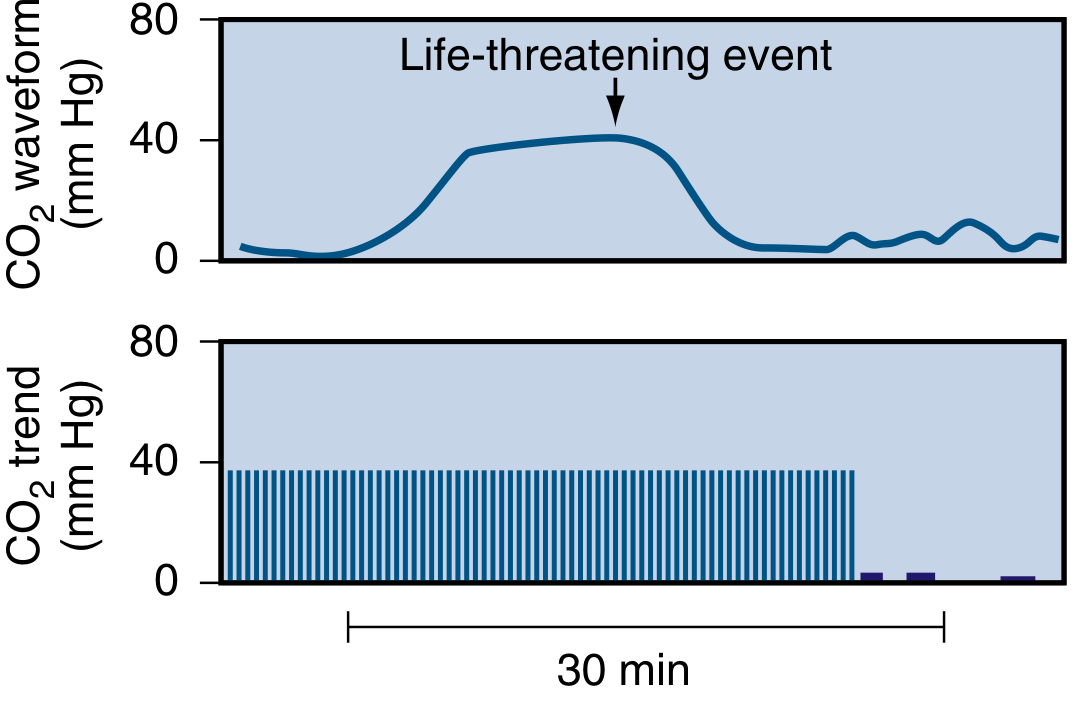
Murray & Nadel, eFig. 31.24: Sudden loss of CO₂ signal after a life-threatening event (disconnected airway, ventilator malfunction).
Capnography detects:
- Obstructed ETT (absent or markedly reduced waveform)
- Disconnected airway (sudden loss of signal)
- Ventilator malfunction (absent signal)
- Severe pulmonary hypoperfusion (progressive decline in PETCO₂)
- Pulmonary embolism (characteristic waveform with progressively sloping plateau)
D. Pulmonary Embolism
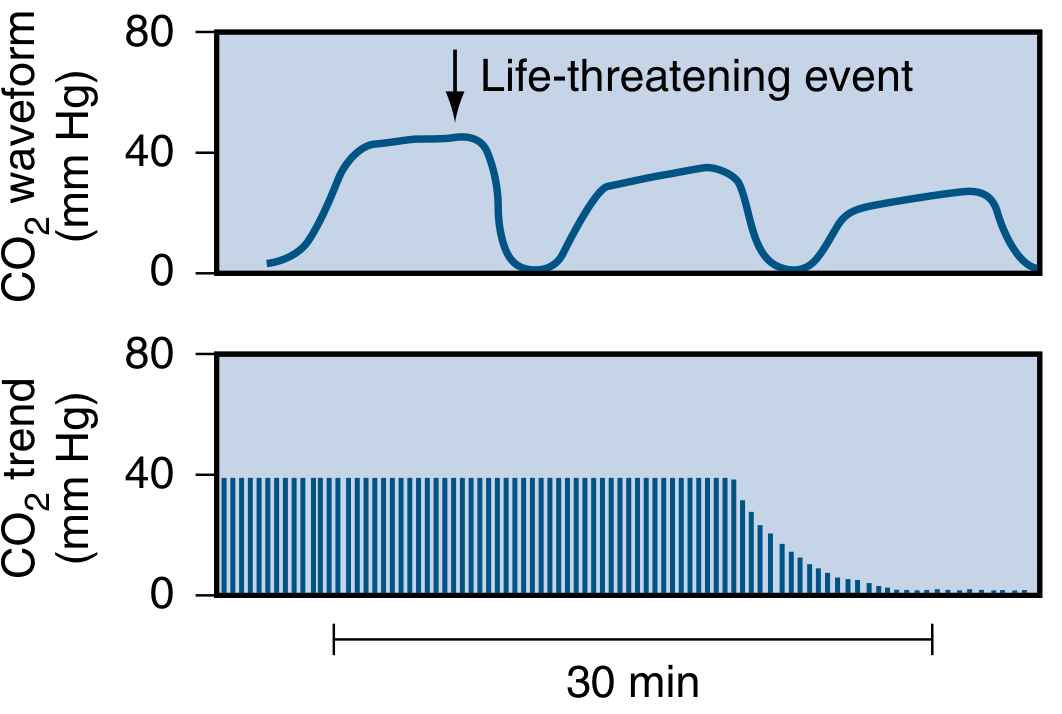
Murray & Nadel, eFig. 31.25: Progressively declining PETCO₂ with sloping plateau — pattern suggesting pulmonary vascular obstruction, cardiac arrest, or severe hypoperfusion.
"The shape of the waveform may be diagnostic of pulmonary vascular obstruction." — Murray & Nadel, p. 738
E. Monitoring Adequacy of Ventilation
Capnography provides breath-to-breath assessment of ventilation without arterial blood sampling. It is particularly useful in:
- Procedural sedation monitoring
- Transport of ventilated patients
- ICU monitoring
F. Nocturnal Hypoventilation in Neuromuscular Disease
End-tidal CO₂ (ETCO₂) monitoring during polysomnography (PSG) is a surrogate marker for PaCO₂ and is used to diagnose nocturnal alveolar hypoventilation in patients with neuromuscular disorders (ALS, muscular dystrophy, kyphoscoliosis).
- Diagnostic criterion: PaCO₂ (or surrogate ETCO₂/PtcCO₂) >55 mm Hg during sleep for ≥10 minutes, OR an increase ≥10 mm Hg from awake levels for ≥10 minutes
"Polysomnography (PSG) with end-tidal CO₂ (ETCO₂) or transcutaneous carbon dioxide monitoring (PtcCO₂), both surrogate markers for PaCO₂, is useful in diagnosing nocturnal alveolar hypoventilation." — Fishman's Pulmonary Diseases and Disorders, p. 2704
G. Cardiac Output and Fluid Responsiveness
There is growing interest in using capnography to predict fluid responsiveness and assess changes in cardiac output non-invasively in critically ill patients, though PETCO₂ correlates poorly with PaCO₂ in the ICU due to multiple confounding variables (ventilator settings, lung disease, cardiac output itself).
8. Abnormal Capnogram Patterns
| Pattern | Cause | Significance |
|---|---|---|
| No CO₂ signal | Esophageal intubation; disconnected airway | Immediate corrective action |
| Sudden disappearance | Ventilator disconnect; circuit leak | Life-threatening emergency |
| Progressive PETCO₂ decline | PE; decreasing cardiac output; cardiac arrest | Urgent evaluation |
| Elevated PETCO₂ | Hypoventilation; ↑ CO₂ production (fever, NaHCO₃ infusion) | Adjust ventilation |
| Sloping Phase III plateau | COPD; obstructive disease; V/Q mismatch | Suggests airflow obstruction |
| Elevated baseline (no return to zero) | Rebreathing (exhausted CO₂ absorber; incompetent valve) | Equipment problem |
"When wasted ventilation is increased because of regional increased ventilation relative to perfusion (e.g., restrictive or obstructive ventilatory defects, parallel dead space, or pulmonary vascular obstruction), differences between arterial and end-tidal carbon dioxide are also increased. In these situations the alveolar plateau is present but abnormally reduced." — Murray & Nadel, p. 738
9. Transcutaneous CO₂ Monitoring (PtcCO₂) — Related Technique
A complementary non-invasive method for CO₂ monitoring. A sensor (typically placed on the earlobe or forehead) is heated to 42°C to cause local vasodilation and enhance CO₂ diffusion. CO₂ is measured by pH changes in an electrolyte solution or by infrared photometry.
- Closely correlates with PaCO₂ in healthy subjects and stable patients
- Limitations: Long time constant; unreliable in poor perfusion, vasopressor use, peripheral vascular disease, edema, obesity
- Technology has improved, with better accuracy in critically ill patients including those with very high PCO₂
"Although TCO₂ monitoring is considered valid in routine respiratory care, its validity in critically ill patients has been challenged because poor perfusion, peripheral vascular disease, or vasopressors may confound measurements." — Fishman's Pulmonary Diseases and Disorders, p. 2597
10. Limitations of Capnography
- Overestimates PaCO₂ in states of high dead space — PETCO₂ may be several mm Hg lower than PaCO₂ in ARDS, PE, pulmonary vascular disease, and low cardiac output
- No plateau in rapid breathing — PETCO₂ unreliable when end-expiratory plateau is absent
- Misleading with supplemental oxygen or NIV — PETCO₂ reading not accurate in these settings
- Interference — nitrous oxide, acetylene, CO interfere with infrared spectrometry
- Requires calibration — regular calibration essential for accuracy
"End-tidal capnography does not provide accurate data in the presence of obstructive lung disease, in cases where there is no end-expiratory plateau, there is an increase in dead space, or during use of either NIV or supplemental oxygen." — Murray & Nadel, p. 2843
Summary Table
| Feature | Capnometry | Capnography |
|---|---|---|
| Output | Numeric PETCO₂ value | Numeric value + continuous waveform |
| Normal PETCO₂ | 35–45 mm Hg | 35–45 mm Hg |
| Waveform phases | Not displayed | Phase I, II, III, 0 |
| Primary method | Infrared spectrometry | Infrared spectrometry |
| Key clinical uses | ETT confirmation, ventilation monitoring | All of capnometry + CPR quality, PE detection, dead space calculation |
| Gradient (PaCO₂ – PETCO₂) | Normally 2–5 mm Hg | Increases with dead space ↑ |
Sources:
- Fishman's Pulmonary Diseases and Disorders, 5e — Chapter on Monitoring in Acute Respiratory Failure (pp. 2596–2597, 2704)
- Murray & Nadel's Textbook of Respiratory Medicine, 7e — Chapter 31: Noninvasive Monitoring of Gas Exchange, Carbon Dioxide section (pp. 738–739, eFigs. 31.23–31.25)
This is a shared conversation. Sign in to Orris to start your own chat.