Describe lingual thyroid and its investigations and management in detail for 50 marks with diagram and flow charts from Scott Brown, Cummings, stell and marans, Zakir Hussain, dhingra, hazarika and related articles with recent advances according to rguhs university
"lingual thyroid" management diagnosis
PMID: 41127496
"lingual thyroid" "radioiodine" OR "transoral robotic surgery" OR "laser"
lingual thyroid RGUHS ENT exam 50 marks recent advances management 2024
https://pmc.ncbi.nlm.nih.gov/articles/PMC10909054
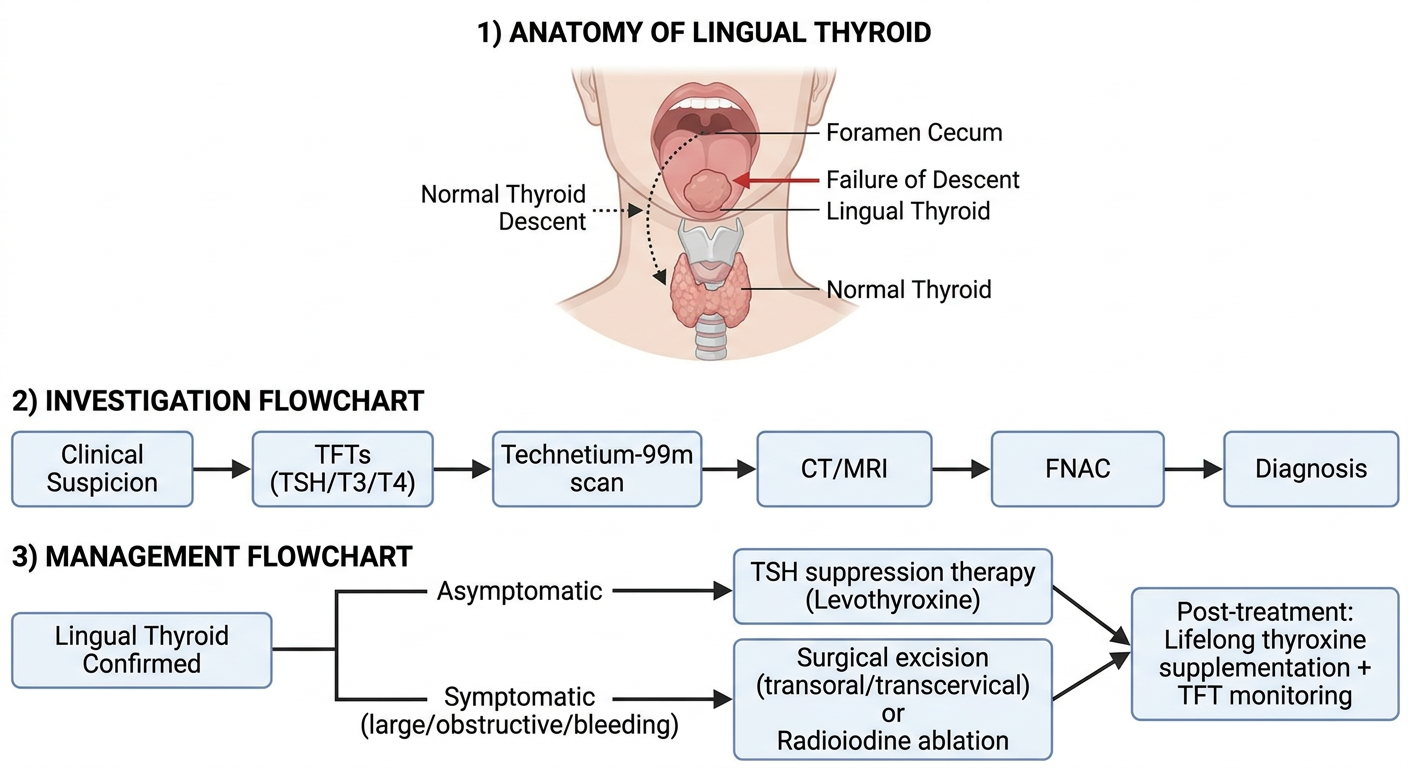
A comprehensive medical diagram showing lingual thyroid: 1) Anatomy diagram showing normal thyroid descent from foramen cecum to neck, with arrow showing failure of descent resulting in lingual thyroid at base of tongue, 2) A flowchart for investigation of lingual thyroid: Clinical suspicion → TFTs (TSH/T3/T4) → Technetium-99m scan → CT/MRI → FNAC → Diagnosis, 3) A management flowchart: Lingual thyroid confirmed → Asymptomatic: TSH suppression therapy (Levothyroxine), Symptomatic (large/obstructive/bleeding): Surgical excision (transoral/transcervical) or Radioiodine ablation, Post-treatment: Lifelong thyroxine supplementation + TFT monitoring. Medical textbook style, clean white background, labelled arrows and boxes.
LINGUAL THYROID
A Complete 50-Mark Answer for RGUHS ENT Examination
DEFINITION
- Cummings Otolaryngology Head and Neck Surgery, p. 1641
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol. 2, p. 516
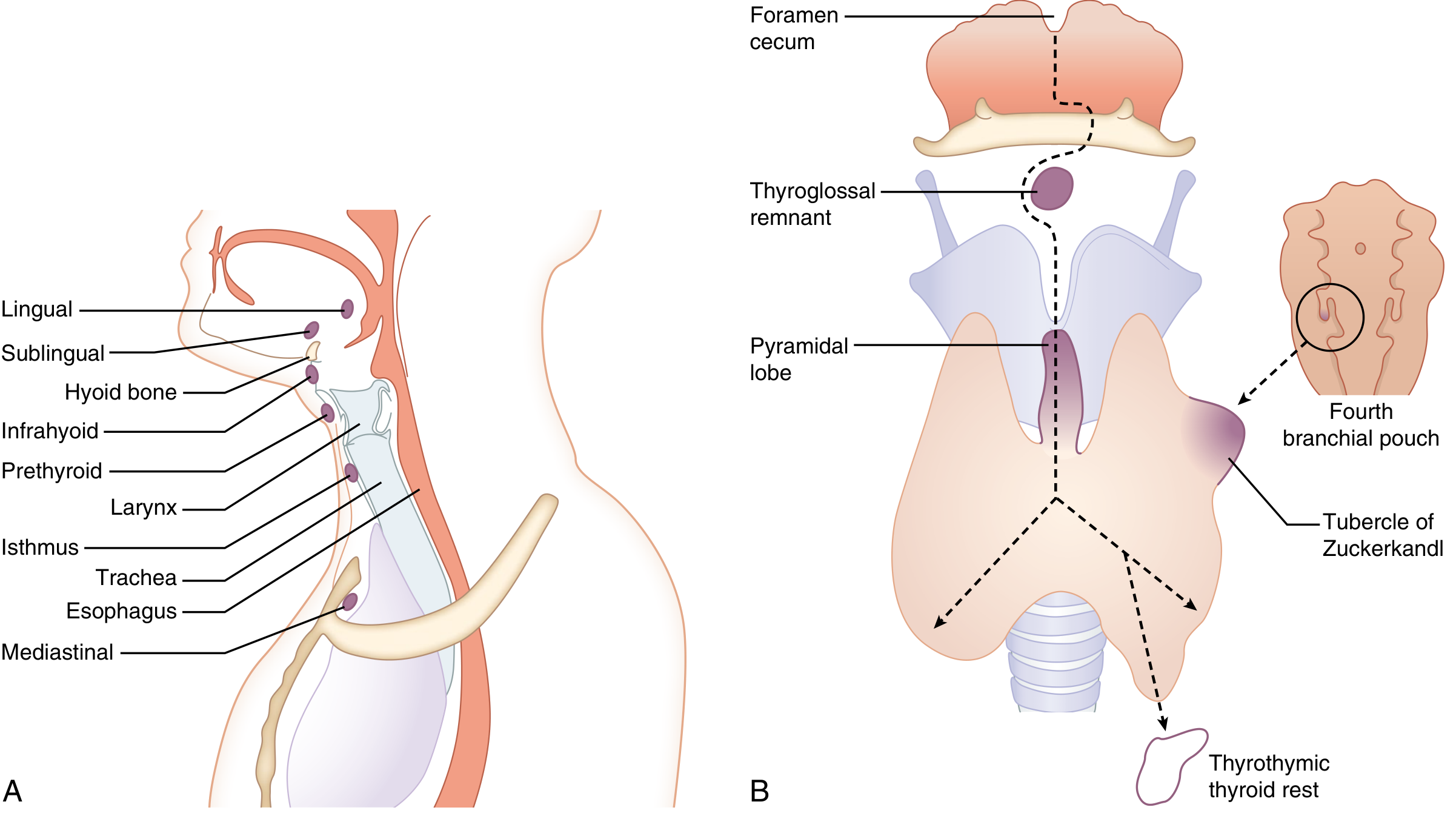
EMBRYOLOGY AND PATHOGENESIS
Normal Thyroid Development
Pathogenesis of Lingual Thyroid
- Defects in TSH receptor signalling
- Mutations in thyroid transcription factor genes (TTF-1/NKX2.1, TTF-2/FOXE1, PAX8)
- Hormonal factors - the condition is more common in females (3:1 to 7:1 female predominance), suggesting a hormonal influence
INCIDENCE AND EPIDEMIOLOGY
| Parameter | Data |
|---|---|
| Prevalence | 1 : 100,000 (general population); 1 : 18,000-1 : 100,000 neonates |
| Gender | Females >> Males (3:1 to 7:1) |
| Age at presentation | Usually at puberty, pregnancy, or menopause |
| Only thyroid tissue | In 70-80% of cases, lingual thyroid is the ONLY thyroid tissue present |
| Hypothyroidism | Up to 1/3 to 70% of patients |
| Malignant transformation | Rare; ~1% (same risk as orthotopic thyroid tissue) |
- Scott-Brown's Vol. 2, p. 516; Cummings, p. 1642; Schwartz's Principles of Surgery, p. 1654
ANATOMY OF LINGUAL THYROID
- Located in the midline at the base of tongue, at or posterior to the circumvallate papillae, near or at the foramen caecum
- Appears as a smooth, reddish-brown, lobulated mass
- Ranges from a few mm to several centimetres
- Covered by normal lingual mucosa
- Has a good blood supply from branches of the lingual artery
- May be the sole functioning thyroid tissue in 70-80% of cases - hence, surgery MUST be preceded by imaging to confirm absence of cervical thyroid
CLASSIFICATION
- Lingual - at/near foramen caecum (most common)
- Sublingual - below the foramen caecum, above hyoid
- Ectopic cervical - along the thyroglossal duct path
- Type 1: Lingual (most superior)
- Type 2: Sublingual
- Type 3: Prelaryngeal (most inferior, pre-tracheal)
CLINICAL FEATURES
Presentation
Symptoms (ABCDE - mnemonic)
B - Bleeding/haemorrhage from the mass
C - Choking sensation / globus pharyngeus
D - Dysphagia (difficulty swallowing)
E - Endocrine dysfunction (hypothyroidism - lethargy, weight gain, cold intolerance, constipation)
- Dysphonia / change in voice (muffled "hot potato" voice)
- Obstructive sleep apnea
- Cough
- Sensation of a lump in the throat
Aggravating Factors (Periods of Increased TSH Demand)
- Puberty
- Pregnancy
- Menopause
- Periods of increased metabolic demand
- Cummings, p. 1642; K J Lee's Essential Otolaryngology, p. 521
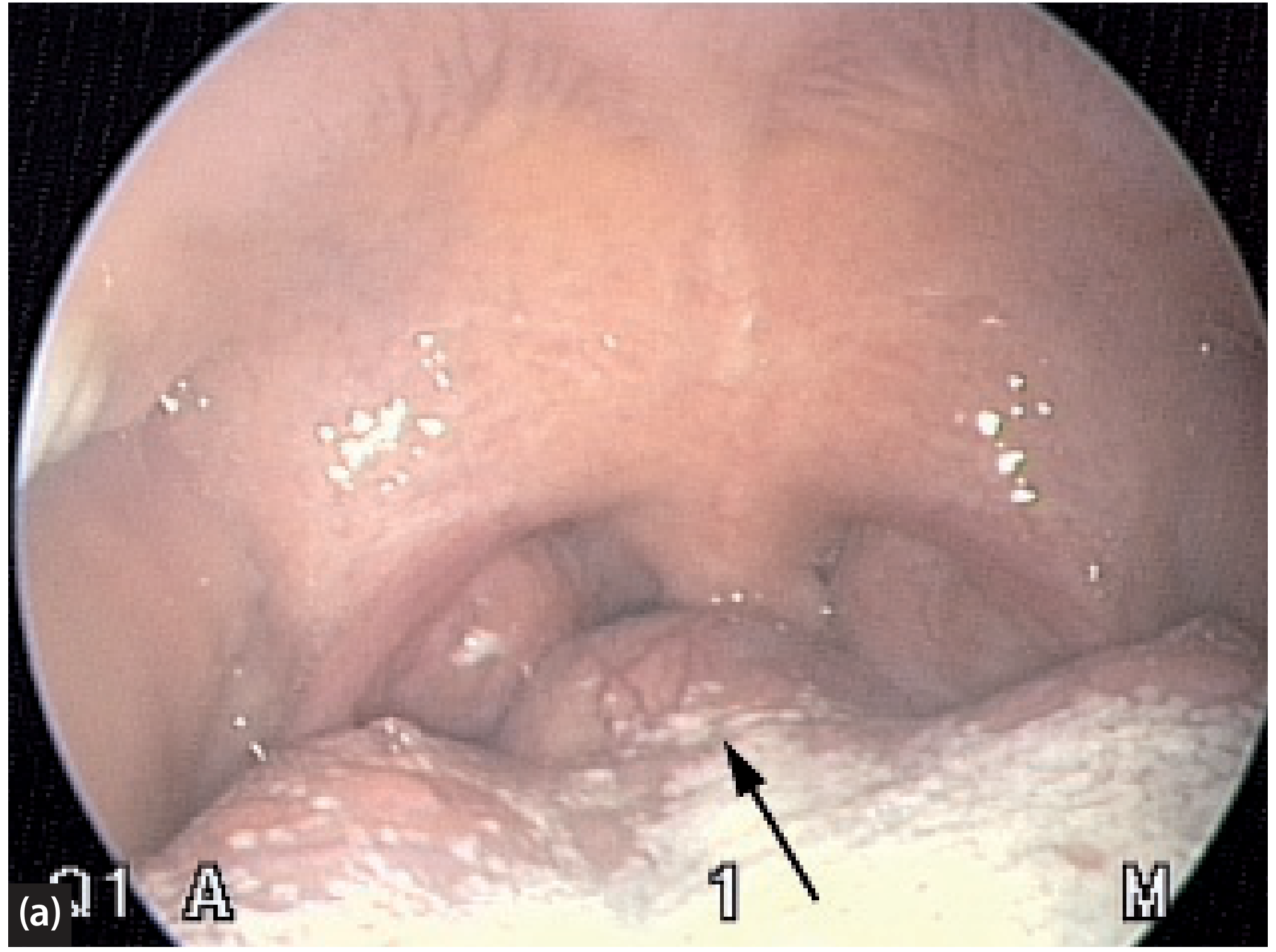
Signs on Examination
- Smooth, red/bluish-red, midline mass at the base of tongue near the foramen caecum
- Surface may be lobulated
- Bleeds easily on probing
- Pulsatile in some cases (vascular supply)
- Absence of thyroid gland in the normal pretracheal position (important!)
- No thyroid palpable in the neck
INVESTIGATIONS
FLOWCHART: Investigation Algorithm
CLINICAL SUSPICION
(Base of tongue mass + absent cervical thyroid)
|
↓
THYROID FUNCTION TESTS
(TSH, Free T3, Free T4)
- Hypothyroid (30-70%), Euthyroid, rarely Hyperthyroid
|
↓
RADIONUCLIDE SCAN (Tc-99m Pertechnetate or I-123)
- Confirms functioning thyroid tissue at tongue base
- Shows NO uptake in normal cervical position
- GOLD STANDARD for confirming lingual thyroid
|
↓
IMAGING: CT SCAN (unenhanced) / MRI
- CT: Hyperdense midline tongue base mass (due to iodine content)
- MRI: Preferred (no radiation); sagittal views most informative
- Identifies if cervical thyroid is present or absent
|
↓
ULTRASOUND NECK
- Confirms absence/presence of orthotopic thyroid
- Can characterize mass
|
↓
FINE NEEDLE ASPIRATION CYTOLOGY (FNAC)
- Only if malignancy suspected
- Shows thyroid follicular cells
|
↓
BLOOD TESTS
- Complete blood count
- Serum calcium (assess PTH/parathyroid)
|
↓
DEFINITIVE DIAGNOSIS
Details of Each Investigation
1. Thyroid Function Tests (TFTs)
- TSH, Free T3, Free T4
- TSH is elevated in hypothyroidism (most common - up to 70%)
- T3/T4 low in hypothyroidism
- Hyperthyroidism is rare
- Baseline TFTs mandatory before any treatment
2. Radionuclide Thyroid Scintigraphy (MOST IMPORTANT)
- Technetium-99m (Tc-99m) pertechnetate scan is the investigation of choice
- Tc-99m is taken up by metabolically active thyroid tissue
- In lingual thyroid: Uptake at base of tongue, NO uptake in cervical position
- Can also use I-123 or I-131 scanning
- This is the gold standard for:
- Confirming that the mass is thyroid tissue
- Establishing whether cervical thyroid tissue exists (critical before surgery)
- Assessing functional status
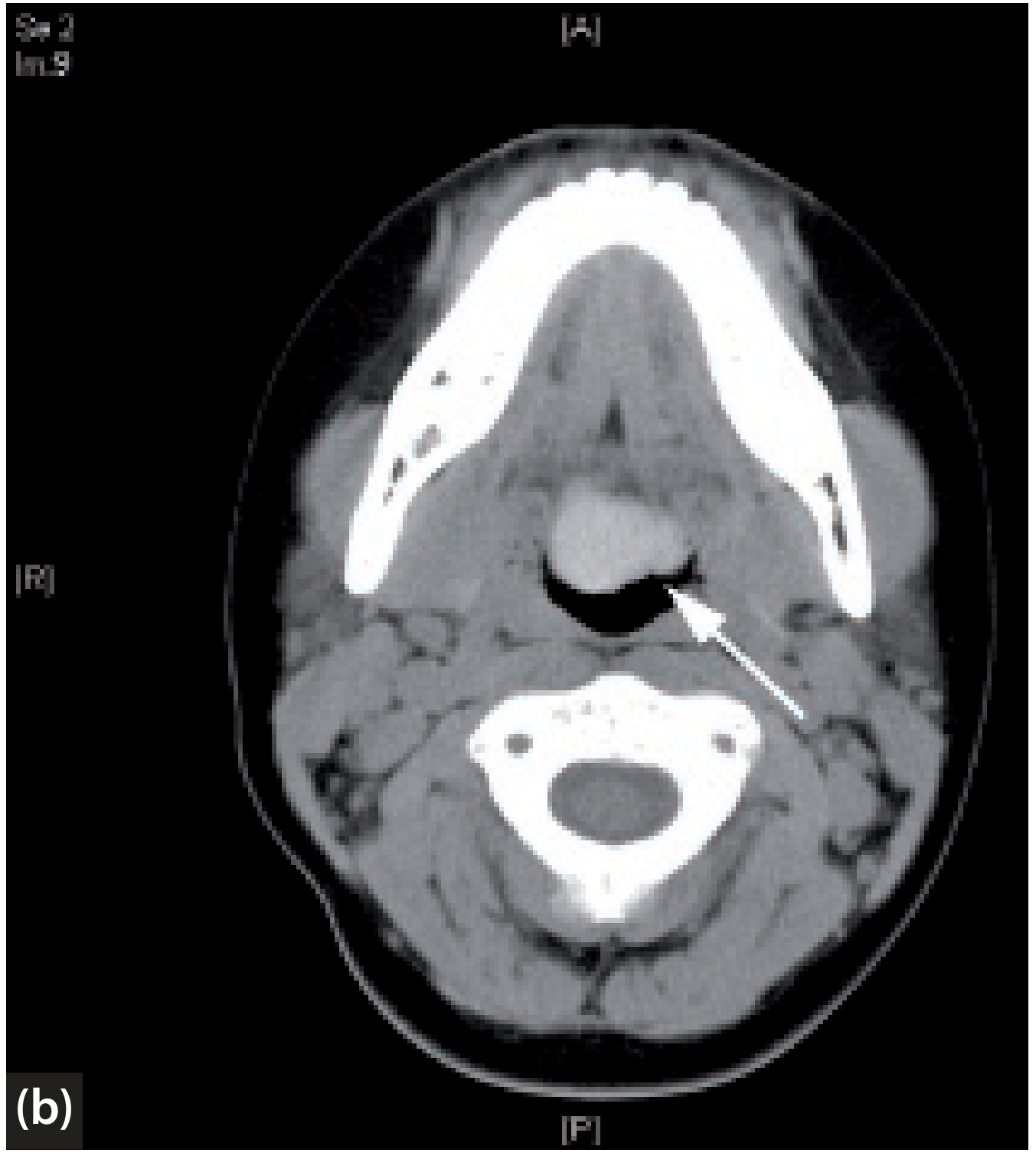
3. CT Scan (Computed Tomography)
- Unenhanced CT is preferred - lingual thyroid appears hyperdense compared to surrounding tongue musculature (due to high iodine content)
- Contrast-enhanced CT is an alternative but may obscure density differences
- Sagittal and axial views helpful
- Delineates size, extent, relationship to adjacent structures
- Identifies any cervical thyroid tissue
4. MRI (Magnetic Resonance Imaging)
- Preferred over CT (no ionizing radiation - especially important in children and young women)
- Sagittal views are particularly helpful
- Lingual thyroid: Isointense on T1, high signal on T2 (relative to muscle)
- Better soft tissue detail
- Delineates airway compromise
5. Ultrasonography (USG Neck)
- Confirms absence of thyroid gland in normal cervical position
- Can characterize the mass (echogenicity, vascularity on Doppler)
- Non-invasive, no radiation, widely available
- Less useful than CT/MRI for tongue base, but valuable for neck assessment
6. Fine Needle Aspiration Cytology (FNAC)
- Reserved for cases where malignancy is suspected
- Shows thyroid follicular cells, colloid
- Malignancy reported in ~1% of cases (usually papillary thyroid cancer)
- Must be done cautiously - risk of bleeding given vascularity
7. Laryngoscopy / Nasopharyngoscopy
- Direct visualization of the mass
- Assess airway
- Evaluate degree of obstruction
Summary Table of Investigations
| Investigation | Purpose | Key Finding |
|---|---|---|
| TFTs (TSH, T3, T4) | Endocrine status | ↑TSH in 70% |
| Tc-99m scan | Confirm thyroid tissue; Gold standard | Uptake at tongue base, none in neck |
| I-123 scan | Functional assessment | Similar to Tc-99m |
| Unenhanced CT | Anatomical detail | Hyperdense midline mass |
| MRI | Preferred imaging | Sagittal views; no radiation |
| USG neck | Orthotopic thyroid check | Absent thyroid in neck |
| FNAC | Malignancy exclusion | Follicular cells, colloid |
| Nasopharyngoscopy | Direct visualization | Red-brown base of tongue mass |
DIFFERENTIAL DIAGNOSIS
| Condition | Distinguishing Feature |
|---|---|
| Thyroglossal duct cyst | Moves with swallowing and tongue protrusion; cystic on imaging |
| Lingual tonsil hypertrophy | Bilateral; no iodine uptake on scan |
| Vascular tumour / haemangioma | Brighter on MRI; no Tc-99m uptake |
| Vallecular cyst | Cystic; no thyroid scintigraphy uptake |
| Teratoma | Mixed solid-cystic; heterogeneous |
| Squamous cell carcinoma | Infiltrative; irregular margins; no scan uptake |
| Lymphoma | Diffuse; night sweats; no scan uptake |
| Minor salivary gland tumour | No Tc-99m uptake |
| Benign/malignant tongue tumours | No Tc-99m uptake; biopsy diagnostic |
MANAGEMENT
FLOWCHART: Management Algorithm
LINGUAL THYROID CONFIRMED
(By Tc-99m scan + TFTs + imaging)
|
┌───────┴───────┐
| |
ASYMPTOMATIC SYMPTOMATIC
Euthyroid (Obstructive symptoms /
Hypothyroidism /
Haemorrhage /
Malignancy suspected)
| |
↓ ┌─────┴──────────────┐
OBSERVATION | |
+ TFT | |
Monitoring HYPOTHYROID EUTHYROID
| with Symptoms
↓ |
LEVOTHYROXINE ↓
(TSH Suppression) Large/Obstructive?
- Reduces size |
over months ┌───┴──────┐
| | |
Size reduced? RADIOIODINE SURGICAL
| ABLATION EXCISION
YES: Continue (I-131) (See below)
| followed
NO: Consider by LT4
surgical/RAI replacement
SURGICAL EXCISION OPTIONS:
├── Transoral routes (preferred for small-moderate):
│ ├── Transoral coblation-assisted excision (NEW - Recent Advance)
│ ├── Transoral CO2 laser excision
│ ├── Transoral robotic surgery (TORS) - Recent Advance
│ └── Transoral with tongue splitting
└── External (transcervical) routes (for large lesions):
├── Transhyoid pharyngotomy
├── Lateral pharyngotomy
├── Combined transoral + transcervical
└── ± Tracheostomy (for massive lesions)
POST-TREATMENT:
- ALL patients: LIFELONG thyroxine (LT4) replacement
- TFT monitoring 3-6 monthly
- Paediatric endocrinology review (children)
- Annual surveillance imaging if residual tissue
A. CONSERVATIVE MANAGEMENT
1. Observation
- For small, asymptomatic, euthyroid lingual thyroid
- Regular TFT monitoring every 6 months
- Annual imaging to assess size change
2. Thyroid Hormone Suppression (TSH Suppression Therapy)
- Levothyroxine (LT4) - the mainstay of medical management
- Mechanism: Exogenous T4 suppresses pituitary TSH secretion; reduced TSH drive leads to regression/non-growth of the lingual thyroid
- Indication: Small asymptomatic lingual thyroid with or without hypothyroidism
- Reduction in size is often slow; dramatic results should not be expected
- Also corrects hypothyroidism
- Paediatric endocrinology input is essential for children
- Dose: 1.6-2 mcg/kg/day, adjusted to keep TSH in low-normal or suppressed range
- Scott-Brown's Vol. 2; Cummings, p. 1642
B. RADIOIODINE ABLATION (I-131)
- Indication: Symptomatic lingual thyroid in adult patients unfit for surgery, or when surgery is refused
- Mechanism: I-131 is selectively taken up by thyroid tissue and destroys follicular cells by beta radiation
- Advantage: Non-surgical, effective at reducing mass size
- Disadvantage:
- Destroys the ONLY functioning thyroid tissue in 70-80% of patients - patient becomes permanently hypothyroid
- Requires lifelong LT4 supplementation post-ablation
- Generally avoided in children (risk of radiation-induced malignancy)
- Multiple doses may be needed
- Pre-treatment: Confirm no cervical thyroid on scan
- Post-treatment: Mandatory lifelong thyroxine replacement
C. SURGICAL MANAGEMENT
Indications for Surgery
- Significant obstructive symptoms (dysphagia, airway obstruction, dysphonia)
- Recurrent or severe haemorrhage
- Failed conservative/medical therapy
- Suspected or confirmed malignancy
- Cystic degeneration
- Patient preference
Pre-operative Preparation
- TFT optimization (correct hypothyroidism)
- Crossmatch blood (highly vascular)
- Nasotracheal intubation
- Consent for tracheostomy if indicated
- Endocrinology consultation
Surgical Approaches
I. TRANSORAL APPROACHES (Preferred for small to moderate lesions)
- Puxeddu et al. first described this for lingual thyroid
- Excellent haemostasis, precise cutting
- Shorter hospital stay
- Suitable for moderate-sized lesions
- Da Vinci robotic system used
- Excellent visualization of tongue base
- Magnified, three-dimensional view
- Good haemostasis
- Reduced postoperative pain
- No external scar
- Gaining popularity as preferred approach (D'Andrea et al., 2022, PMID: 33843266)
- Recent Advance: TORS is now considered by many as the best surgical approach for lingual thyroid
- Coblation = Controlled Ablation using radiofrequency energy in a saline medium
- Operates at low temperatures (40-70°C) unlike monopolar cautery (>400°C)
- Advantages:
- Minimal bleeding (excellent haemostasis)
- No external incision
- Less postoperative pain
- Shorter hospital stay
- No need for tracheostomy in most cases
- Quick recovery
- A prospective study of 12 cases from Government ENT Hospital, Hyderabad (2016-2023) showed excellent results with coblation-assisted transoral excision
- Disadvantage: Difficult exposure for very large lesions
- (PMC 10909054 - Indian J Otolaryngol Head Neck Surg, 2024)
- Useful for larger transoral access
- Associated with longer recovery
II. EXTERNAL (TRANSCERVICAL) APPROACHES (For large/deep lesions)
- Access through the hyothyroid membrane
- Good exposure for large tongue base lesions
- Risk: damage to hypoglossal nerve, superior laryngeal nerve
- Access through lateral pharynx
- Less common; for laterally placed lesions
- For very large lesions requiring maximum exposure
- Usually requires tracheostomy
- Mandatory for large masses where post-operative swelling/bleeding could obstruct the airway
- Also required when nasotracheal intubation is not possible
Surgical Complications
- Haemorrhage (primary/reactionary/secondary) - most feared
- Airway compromise/oedema
- Hypothyroidism (if only tissue; permanent)
- Infection
- Dysphonia (if nerve injury)
- Dysphagia (temporary/permanent)
Post-operative Care
- Lifelong levothyroxine supplementation (mandatory, as lingual thyroid is ONLY tissue in 70-80%)
- Regular TFT monitoring
- Nasogastric feeding if significant swelling
- Tracheostomy care if performed
SPECIAL SITUATIONS
Lingual Thyroid in Pregnancy
- Lingual thyroid can enlarge significantly during pregnancy due to elevated TSH demand
- May cause acute airway obstruction
- Management: Careful airway monitoring; LT4 supplementation to suppress TSH
- Surgery if acute airway obstruction; planned caesarean if large mass
Lingual Thyroid in Children
- Presents at puberty with TSH demand
- Radioiodine generally avoided (radiation risk)
- Preferred treatment: LT4 suppression + surgical excision if indicated
- Paediatric endocrinology essential
Malignant Lingual Thyroid
- Risk approximately 1% (same as orthotopic thyroid)
- Usually papillary thyroid carcinoma
- FNAC confirms
- Treatment: Surgical excision + radioiodine + lifelong LT4
TRANSPOSITION PROCEDURE
RECENT ADVANCES
| Advance | Detail |
|---|---|
| TORS (Transoral Robotic Surgery) | Da Vinci robot; best surgical approach per recent systematic review (D'Andrea 2022, PMID 33843266); superior visualization, minimal morbidity |
| Coblation-assisted transoral excision | Radiofrequency at low temperature (40-70°C); minimal bleeding, no external incision, short hospital stay; prospective Indian study 2024 (PMC 10909054) |
| CO2 laser transoral excision | Long-established minimally invasive approach |
| Multimodal diagnostic approach | Combining USG + CT/MRI + Tc-99m scintigraphy + FNAC for accurate diagnosis (Aldawas & Ragab, Cureus 2025, PMID 41127496) |
| MDT approach | Multidisciplinary team (ENT + Endocrinology + Radiology + Nuclear Medicine) for individualized management |
| Molecular genetics | TTF-1, TTF-2, PAX8 mutations implicated; may guide future targeted therapies |
| Airway management protocols | Standardized protocols for lingual thyroid causing acute airway obstruction (Nisa et al., 2022, PMID 35201391) |
PROGNOSIS
- With appropriate management, prognosis is generally good
- Lifelong thyroxine supplementation is required in most patients post-surgery/radioiodine
- Malignancy is rare but must be excluded
- Surveillance is lifelong
SUMMARY CHART: Lingual Thyroid at a Glance
┌────────────────────────────────────────────────────────────┐
│ LINGUAL THYROID │
├────────────────┬───────────────────────────────────────────┤
│ Definition │ Ectopic thyroid at base of tongue │
│ Embryology │ Failure of descent from foramen caecum │
│ Prevalence │ 1:100,000; F:M = 3-7:1 │
│ Only tissue │ 70-80% of cases │
│ Presentation │ Dysphagia, dyspnea, hypothyroidism │
│ Key Inv. │ Tc-99m scan (Gold Standard) + TFTs │
│ Imaging │ Unenhanced CT / MRI (sagittal preferred) │
│ Medical Rx │ Levothyroxine (TSH suppression) │
│ Surgical Rx │ Transoral (TORS/Coblation/CO2 laser) │
│ Radioiodine │ Adults; NOT in children │
│ Post-treatment │ LIFELONG LT4 + TFT monitoring │
└────────────────┴───────────────────────────────────────────┘
REFERENCES
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol. 2 (9781138094634) - Chapter 41: LINGUAL THYROID, pp. 515-516
- Cummings Otolaryngology Head and Neck Surgery (9780323612173) - Chapter 90: Lingual Thyroid, p. 1641-1642
- Schwartz's Principles of Surgery, 11th Edition (9781259835346) - Developmental Abnormalities: Lingual Thyroid, p. 1654
- Sabiston Textbook of Surgery, 21st Edition (9780443124341) - Chapter 73: Ectopic Thyroid Tissue, p. 1485-1486
- K J Lee's Essential Otolaryngology (9781260122237) - Normal Variants Mimicking Disease, p. 521
- Dhingra's Diseases of Ear, Nose and Throat - Ectopic Thyroid, Chapter on Neck Swellings
- Hazarika's Textbook of ENT and Head & Neck Surgery - Lingual Thyroid
- Zakir Hussain's Manual of ENT - Lingual Thyroid
- Stell and Maran's Head and Neck Surgery - Ectopic Thyroid
- D'Andrea G, Vairel B, Vandersteen C. Is Transoral Robotic Surgery the Best Surgical Treatment for Lingual Thyroid? A Case-Report and Literature Review. Ann Otol Rhinol Laryngol. 2022 Jan. [PMID: 33843266]
- Aldawas G, Ragab S. A Review of Thyroid Rests: From Embryology to Clinical Management. Cureus. 2025 Oct. [PMID: 41127496]
- Nisa L, Morrison S, Levi E. Airway management in patients with lingual thyroid: a case report and review of the literature. Eur Arch Otorhinolaryngol. 2022 Jul. [PMID: 35201391]
- Coblation study: Advances in Lingual Thyroid Management Using Coblation Technology: A Case Series Study. Indian J Otolaryngol Head Neck Surg. 2024;76(1):938-43. [PMC 10909054] - Government ENT Hospital, Hyderabad
RGUHS Exam Tip: For a 50-mark answer, the key areas examiners look for are:
- Embryology (5 marks)
- Clinical features (5 marks)
- Investigations with emphasis on Tc-99m scan (10 marks)
- Management - Medical, Radioiodine, Surgical approaches (20 marks)
- Recent advances - TORS, Coblation (5 marks)
- Diagrams and flowcharts (5 marks)