A complete guide to wernickes encephalopathy and korsakoff’s psychosis
Reading File
Finding Sources
Finding Sources
Searching PubMed
"Wernicke encephalopathy"[MeSH Terms] AND "thiamine"[MeSH Terms]
Searching the Web
Wernicke encephalopathy Korsakoff psychosis clinical guide 2024 2025
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Searching Images
Wernicke encephalopathy MRI brain mammillary bodies thalamus
I now have comprehensive data from multiple authoritative sources. Let me compile the complete guide.
Wernicke's Encephalopathy & Korsakoff's Psychosis: A Complete Guide
1. Overview & Historical Context
Wernicke's encephalopathy (WE) and Korsakoff's syndrome (KS) represent two ends of a single disease spectrum — Wernicke-Korsakoff syndrome (WKS) — both caused by thiamine (vitamin B1) deficiency. WE is the acute, potentially reversible phase; KS is the chronic, largely irreversible amnestic state that follows.
- WE was first described by Gayet (French ophthalmologist) in 1875, and independently by Carl Wernicke (German neurologist) in 1881.
- "Korsakoff psychosis" is an older term; modern neurology prefers Korsakoff syndrome or amnesic state, as psychosis is not the dominant feature. — Adams and Victor's Principles of Neurology, 12th ed.
2. Thiamine Biochemistry & Pathophysiology
Thiamine (B1), as thiamine pyrophosphate (TPP), is a critical cofactor in energy metabolism:
- Pyruvate dehydrogenase — entry into the TCA cycle
- α-ketoglutarate dehydrogenase — TCA cycle intermediate step
- Transketolase — pentose phosphate pathway
Deficiency of α-ketoglutarate dehydrogenase activity in astrocytes leads to microglial activation and glutamatergic toxicity, the key mechanism of WE neuronal injury. — Goldman-Cecil Medicine
Because thiamine is required to metabolize glucose, administration of IV glucose before thiamine replacement can precipitate or worsen WE — a critical clinical pitfall. — Maudsley Prescribing Guidelines, 15th ed.
Total body thiamine stores are depleted within 2–3 weeks of inadequate intake.
3. Causes & Risk Factors
Primary Cause
- Chronic alcohol use disorder — the most common cause in Western countries (both reduced dietary intake and impaired intestinal absorption)
Non-alcoholic Causes
| Category | Examples |
|---|---|
| Prolonged vomiting | Hyperemesis gravidarum, cyclical vomiting, chemotherapy |
| Malabsorption | Bariatric surgery (especially gastric bypass), inflammatory bowel disease |
| Refeeding syndromes | Parenteral nutrition without thiamine supplementation |
| Systemic illness | AIDS/HIV, cancer, cachexia |
| Dialysis | Thiamine lost during hemodialysis (33% prevalence of deficiency in symptomatic dialysis patients) — Bradley & Daroff's Neurology |
| Eating disorders | Anorexia nervosa, bulimia nervosa |
| Prolonged fasting | Hunger strikes, extreme diets |
| Digitalis poisoning |
Risk Factors in Alcohol Dependence (Maudsley Guidelines)
- Acute withdrawal
- Malnourishment / low BMI (<18)
- Decompensated liver disease
- Emergency department attendance or acute hospitalization
- Homelessness
- Memory disturbance or peripheral neuropathy
- Previous episode of WE
4. Neuropathology
Affected Brain Regions
WE preferentially affects regions with the highest thiamine-dependent metabolic demand:
- Mammillary bodies (most characteristic; bilaterally affected)
- Periaqueductal gray matter
- Medial thalami (anterior and centromedian nuclei; dorsomedial thalamic nucleus lesions best correlate with memory disturbance in KS)
- Floor of the fourth ventricle
- Superior and inferior colliculi
- Hypothalamus (occasionally)
- Cerebral cortex (rarely, in severe cases)
Microscopic Changes
- Neuronal swelling and microscopic hemorrhages (early)
- Gliosis (later)
- Resolution of necrosis → cystic spaces with hemosiderin-laden macrophages
In Korsakoff syndrome, damage is concentrated in the limbic system: mammillary bodies, amygdala, dorsomedial thalamus, and anterior thalamus. Cortical involvement in KS may relate to direct alcohol neurotoxicity rather than thiamine deficiency per se. — Robbins & Kumar Basic Pathology; Goldman-Cecil Medicine
5. Clinical Presentation
Wernicke's Encephalopathy: Classic Triad
| Feature | Description |
|---|---|
| Mental status changes | Ranges from mild inattention and memory impairment to delirium and coma; often with apathy or abulia |
| Ocular abnormalities | Nystagmus, dysconjugate gaze, horizontal/vertical gaze palsies, ophthalmoplegia |
| Ataxia | Affects legs > arms > trunk; gait ataxia prominent |
⚠️ The full triad is present in only ~30% of cases. Up to 75% of cases are undiagnosed at the time of death (only ~25% detected before death). — Goldman-Cecil Medicine
Additional Features
- Autonomic dysfunction: bradycardia, hypothermia, hypotension (can be life-threatening)
- Papilledema, optic neuropathy
- Seizures, myoclonus
- Peripheral neuropathy
- Signs of chronic alcoholism (gynecomastia, palmar erythema, Dupuytren's contractures, ascites)
Maudsley Guidance: Presume WE in Any Detoxification Patient with ANY of:
- Ataxia
- Hypothermia or hypotension
- Confusion or memory disturbance
- Ophthalmoplegia / nystagmus
- Unconsciousness / coma
6. Korsakoff's Syndrome
Core Features
Korsakoff syndrome develops in up to 80% of patients surviving WE. It is more likely to follow WE in the setting of alcoholism than in pure nutritional deficiency — likely due to synergistic mechanisms including repeated alcohol withdrawal causing glutamate neurotoxicity compounded by thiamine deficiency. — Goldman-Cecil Medicine
Three cardinal features (Adams & Victor):
- Retrograde amnesia — impaired recall of events established before onset
- Anterograde amnesia — inability to form new memories or learn new information
- Impaired temporal localization of past experience
What Is Preserved
- Alertness and attention
- Language comprehension and expression
- Spatial organization
- Procedural (motor) memory
- Immediate recall (digit span) — a measure of registration/attention, not memory encoding
- Social interaction
"Equally important in the definition of the Korsakoff syndrome is this integrity of certain aspects of behavior and mental function." — Adams & Victor's Principles of Neurology
Confabulation
- Momentary confabulation: partial memories inaccurately localized in time, provoked by questions
- Fantastic confabulation: spontaneous elaborate false narratives; more common in the initial confused phase
- Confabulation is not obligate for diagnosis; it typically lessens over time as a compensatory mechanism — Adams & Victor
Neuropsychological Profile
- Anterograde > retrograde amnesia severity
- Remote (early life) memories relatively preserved vs. recent (Ribot's Rule)
- Mild executive dysfunction (frontal lobe involvement)
- Patients are typically unaware of their memory impairment (anosognosia)
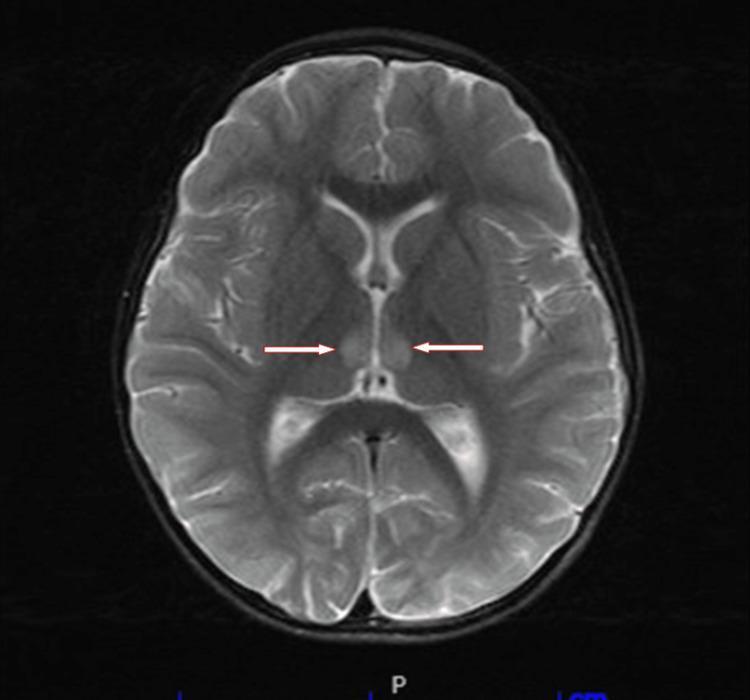
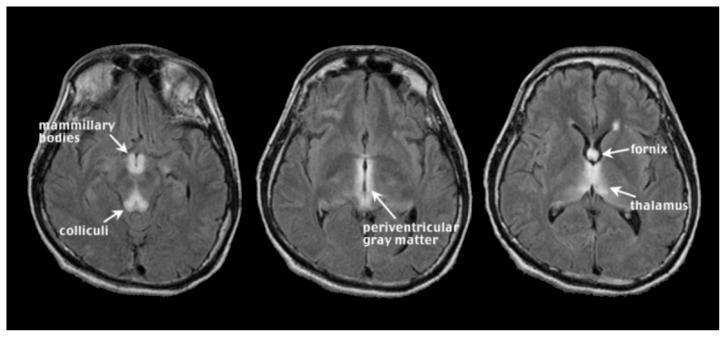
7. Neuroimaging
MRI Findings in Acute WE
T2-weighted/FLAIR sequences show bilateral and symmetrical hyperintensities in:
- Mammillary bodies
- Periaqueductal gray matter
- Medial thalami / periventricular regions of the 3rd ventricle
- Floor of the 4th ventricle / pons / medulla
- Basal ganglia (less commonly)
- Cortex (rare; implies severe disease)
Special MRI Findings
- DWI: restricted diffusion (cytotoxic edema); may show vasogenic component (increased ADC)
- Microbleeds on T1/GRE in thalami and mammillary bodies → poor outcome marker
- Contrast enhancement of mammillary bodies: present in ~80% of cases, even before T2 changes are visible — considered highly specific — Grainger & Allison's Diagnostic Radiology
- Periaqueductal contrast enhancement: ~50% of cases
MRI in Chronic Korsakoff Syndrome
- T2 signal changes become less prominent
- Diffuse brain atrophy, most pronounced in the mesencephalon and mammillary bodies
MRI can be normal in symptomatic WE — a normal MRI does not exclude the diagnosis.
8. Laboratory Investigations
| Test | Finding |
|---|---|
| Serum thiamine | Low (<50 nmol/L); may be normal in ~10% |
| RBC transketolase activity | Reduced (most sensitive functional test) |
| Serum lactate & pyruvate | Elevated (disrupted carbohydrate metabolism) |
| MCV, LFTs, GGT | Signs of chronic alcohol use |
| Magnesium | Often deficient; critical to replace (required for thiamine utilization) |
| Sodium | May be low; must be replaced carefully |
9. Diagnosis
WE is a clinical diagnosis — do not wait for labs or MRI before treating.
The Caine criteria (operational diagnostic criteria used in clinical practice) require any 2 of:
- Dietary deficiency
- Oculomotor abnormalities
- Cerebellar dysfunction
- Either altered mental status or mild memory impairment
A presumptive diagnosis should be made in any at-risk patient with even a single feature.
Differential Diagnoses to Consider
- Hepatic encephalopathy
- Delirium tremens (overlapping with acute alcohol withdrawal)
- Meningitis/encephalitis
- Posterior reversible encephalopathy syndrome (PRES)
- Central pontine myelinolysis
- Drug intoxication / overdose
- Stroke (thalamic, brainstem)
10. Treatment
Principle: Treat First, Confirm Later
"In acute settings, especially in ICUs, all patients should receive replenishment with high-dose IV or IM thiamine prior to any glucose administration." — Goldman-Cecil Medicine
Thiamine Replacement Doses
If WE is suspected / confirmed (acute treatment):
- IV or IM thiamine 500–1000 mg/day × 3–5 days — Goldman-Cecil Medicine
- UK NICE / Maudsley Guidelines: IV thiamine (Pabrinex) 2–3 pairs (each pair = 250 mg) three times daily for 3–5 days
Prophylaxis in high-risk patients (e.g., alcohol detoxification):
- Community: IM thiamine 200–300 mg once daily for at least 3 days
- Hospital: IM or IV thiamine 200–300 mg once daily for 3–5 days with daily monitoring
Low-risk drinkers with adequate diet:
- Oral thiamine 300 mg daily during withdrawal
Additional Measures
- Never give IV glucose before thiamine in a thiamine-deficient or at-risk patient
- Replace magnesium (required cofactor for thiamine-dependent enzymes)
- Replace sodium if deficient
- Monitor electrolytes, fluid balance
- Treat nausea/vomiting (metoclopramide 10 mg or prochlorperazine 5 mg)
Response to Treatment
- Nystagmus and ophthalmoplegia resolve first — often within hours of thiamine administration
- Ataxia resolves more slowly (days to weeks)
- Mental status changes — variable; may partially or fully resolve
- Korsakoff syndrome does not respond to thiamine replacement — prevention by early recognition of WE is essential
11. Prevention
- Thiamine supplementation of anyone at risk due to vomiting, starvation, bariatric surgery, dialysis, or malnutrition (>100 mg/day)
- Routine thiamine fortification of foods (e.g., flour, rice) has reduced the population burden
- Universal thiamine before IV dextrose in the emergency department for at-risk patients
- Post-bariatric surgery: lifelong thiamine supplementation is standard of care
12. Prognosis
| Outcome | Data |
|---|---|
| WE untreated mortality | ~90% |
| WE treated mortality | Up to 20% |
| KS following WE | ~80% of WE survivors |
| KS long-term mortality | ~50% of treated patients die within 8 years |
| Cognitive function in KS | Stable (neither progressive nor recovering) |
| Residual deficits | Ataxia and cognitive/memory impairment (partly from alcohol neurotoxicity) |
"Because Korsakoff syndrome does not respond to thiamine replacement, prevention by timely recognition of Wernicke encephalopathy is essential." — Goldman-Cecil Medicine
Recovery from KS
A small proportion (< 20%) achieve partial recovery with prolonged abstinence from alcohol, but full recovery is rare. Prognosis is better in non-alcoholic WKS (e.g., hyperemesis gravidarum).
13. Special Populations
Pregnancy (Hyperemesis Gravidarum)
WE complicating hyperemesis gravidarum is a well-described, systematically reviewed entity. High index of suspicion required; thiamine must be given before IV dextrose. Fetal brain injury is possible if untreated.
Bariatric Surgery
A leading non-alcoholic cause. ASMBS published dedicated clinical guidelines (2025) on prevention, diagnosis and treatment of WE/WKS in bariatric patients.
Renal Failure / Dialysis
Thiamine is water-soluble and dialyzable; patients on renal replacement therapy have high rates of deficiency. A 2024 systematic review (PMID 37838073) documented this in both acute and chronic kidney disease. Routine supplementation is indicated.
HIV/AIDS & Cancer
Cachexia, malabsorption, and poor oral intake create risk. WE can occur without any alcohol history.
14. Comparison: WE vs. KS
| Feature | Wernicke's Encephalopathy | Korsakoff's Syndrome |
|---|---|---|
| Phase | Acute | Chronic |
| Mechanism | Active thiamine deficiency | Structural limbic/thalamic damage |
| Core features | Confusion, ophthalmoplegia, ataxia | Anterograde + retrograde amnesia, confabulation |
| Consciousness | Impaired (delirium → coma) | Preserved (patient is alert) |
| Reversibility | Yes — if treated promptly | Largely irreversible |
| Response to thiamine | Dramatic (oculomotor signs first) | No significant response |
| MRI | Active edema/hemorrhage in mammillary bodies, thalami, periaqueductal | Atrophy of mammillary bodies, mesencephalon |
| Confabulation | Not typical | Present (especially early phase) |
15. Key Takeaways for Clinical Practice
- Diagnose clinically — do not wait for lab confirmation or MRI to start thiamine.
- The full classic triad is present in <30% of cases — treat on suspicion.
- Never administer IV glucose before thiamine in any malnourished or alcohol-dependent patient.
- High-dose IV thiamine (500–1000 mg/day for 3–5 days) is the standard for suspected WE.
- Magnesium replacement is mandatory alongside thiamine.
- Korsakoff syndrome is preventable but not treatable — early WE recognition is the only strategy.
- Non-alcoholic WE is common — think bariatric surgery, hyperemesis, cancer, dialysis.
- Only 25% of WE cases are detected before death — the syndrome is massively under-recognized.
Sources
- Goldman-Cecil Medicine, International Edition
- Adams and Victor's Principles of Neurology, 12th Edition
- Maudsley Prescribing Guidelines in Psychiatry, 15th Edition
- Grainger & Allison's Diagnostic Radiology
- Robbins & Kumar Basic Pathology
- Bradley and Daroff's Neurology in Clinical Practice
- Recent systematic reviews: PMID 37322816 (WE in hyperemesis gravidarum, 2023), PMID 37838073 (WE in kidney disease, 2024), PMID 38306946 (diagnosis and treatment systematic review, 2024)
This is a shared conversation. Sign in to Orris to start your own chat.