Birth injury
Asking for Preferences
Reading File
Finding Sources
Searching PubMed
"birth injury" neonatal
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Loading Image
Here is a thorough overview of birth injury - its types, mechanisms, and key clinical points - drawn from authoritative textbook sources.
Birth Injury - Overview & Types
Birth injury (birth trauma) refers to physical damage to the neonate sustained during labor and delivery. The incidence is approximately 2 per 1,000 live births for significant injuries, though minor soft-tissue trauma is far more common. Risk factors include macrosomia, shoulder dystocia, instrumental delivery (forceps/vacuum), breech presentation, prolonged labor, and maternal diabetes.
1. Scalp & Cranial Injuries
These are the most common birth injuries and are distinguished by the anatomical layer involved:
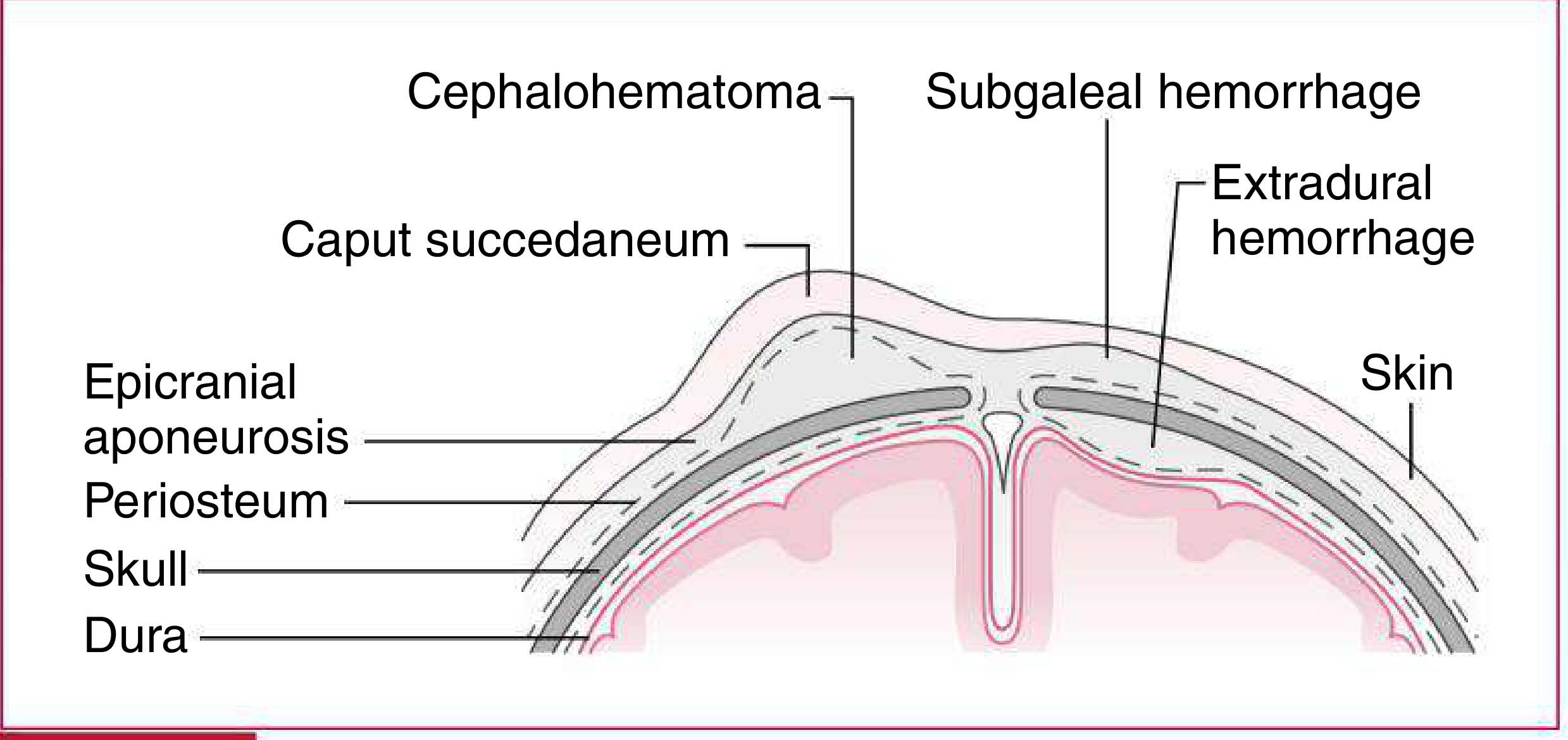
| Feature | Caput Succedaneum | Cephalohematoma | Subgaleal Hemorrhage |
|---|---|---|---|
| Location | Connective tissue above epicranial aponeurosis | Subperiosteal (beneath periosteum) | Beneath epicranial aponeurosis |
| Suture lines | Crosses freely | Does NOT cross sutures | May extend to orbits or nape of neck |
| Onset | Maximal at birth | Increases over 12-24 hrs | Progressive after birth |
| Resolution | 48-72 hours | Weeks | Weeks |
| Severity | Minimal | Rarely severe | Can be severe (especially with coagulopathy) |
- Caput succedaneum: Diffuse pitting edema at the presenting scalp; shifts with gravity; self-resolving.
- Cephalohematoma: Firm, distinct swelling limited by periosteal attachments; does not cross suture lines; associated with underlying skull fracture in ~5% of cases; watch for hyperbilirubinemia as blood resorbs.
- Subgaleal (subaponeurotic) hemorrhage: Most dangerous - blood accumulates in a large potential space and can hold the entire neonatal blood volume. Presents as a fluctuant, ill-defined swelling that crosses sutures and may have a fluid wave. High risk of hemorrhagic shock, especially with coagulopathy.
(Source: Harriet Lane Handbook, 23rd ed., Table 18.3 & Fig. 18.3)
2. Hypoxic-Ischemic Encephalopathy (HIE)
HIE results from perinatal asphyxia - inadequate oxygen and blood flow to the neonatal brain. It is one of the most clinically significant birth injuries.
Criteria for diagnosis/treatment include:
- Cord gas or blood gas within the first hour: pH <7.0 or base deficit >16
- 10-minute APGAR ≤5
- Need for assisted ventilation at birth for ≥10 minutes
Management: Therapeutic hypothermia (33.5°C body cooling) is the standard of care and must be initiated within 6 hours of delivery in infants ≥35 weeks gestation with moderate-to-severe HIE. Head cooling and whole-body cooling are equally efficacious.
(Source: Harriet Lane Handbook, 23rd ed.; Creasy & Resnik's Maternal-Fetal Medicine)
3. Brachial Plexus Palsy (Obstetric Brachial Plexus Injury)
Occurs in approximately 2 per 1,000 births due to stretching or contusion of the brachial plexus - most often during shoulder dystocia, difficult vaginal delivery, or breech extraction.
Three classic types:
| Type | Nerve Roots | Clinical Presentation | Prognosis |
|---|---|---|---|
| Erb-Duchenne palsy | C5, C6 | "Waiter's tip" deformity - arm adducted, internally rotated; elbow extended, forearm pronated, wrist flexed | Best - most common; >90% resolve |
| Klumpke palsy | C8, T1 | Intrinsic hand weakness; claw hand; associated with Horner syndrome (ptosis, miosis, anhidrosis) | Poor |
| Total plexus palsy | C5-T1 | Flail arm | Worst |
Prognosis indicators:
- Lack of biceps function at 6 months = poor prognosis
- Presence of Horner syndrome = poor prognosis
- Progressive glenoid hypoplasia occurs in 70% with persistent internal rotation contracture
Management:
- Passive range of motion exercises (shoulder elevation, abduction, external rotation) by parents
- Await spontaneous recovery for up to 18 months
- Surgical options: microsurgical nerve grafting (early), tendon/muscle transfers (late), rotational osteotomy (>5 years)
(Source: Miller's Review of Orthopaedics, 9th ed.; Campbell's Operative Orthopaedics, 15th ed.)
4. Facial Nerve Palsy
- Incidence: ~1.8 per 1,000 deliveries
- ~80% are related to birth trauma (forceps delivery, cephalopelvic disproportion, sacral prominence pressure on the fetal face)
- Presents as asymmetric facial movement, inability to close the eye on the affected side
- Most cases are peripheral nerve injuries that resolve spontaneously within weeks; eye protection is important to prevent corneal damage
(Source: Shambaugh Surgery of the Ear; Scott-Brown's Otorhinolaryngology)
5. Skeletal (Birth) Fractures
The most common birth fractures are of the clavicle, humerus, and femur.
Risk factors: Macrosomia, breech presentation, instrumented delivery, small uterine incision (cesarean), prematurity, osteogenesis imperfecta.
Clinical features:
- Warmth, swelling, irritability with movement, pseudoparalysis of a limb
- 60-80% of patients have no positive findings on the initial newborn exam - diagnosis is often delayed 1-2 days
- Can mimic osteomyelitis, septic arthritis, or brachial plexus palsy
Management:
- Most heal without surgery and remodel fully
- Clavicular/humeral shaft fractures: pin the sleeve to the front of the shirt for 1-2 weeks
- Femoral fractures: Pavlik harness or splinting; spica cast rarely needed
- Physeal (Salter-Harris) separations at distal femur or humerus are rare but can occur with difficult delivery
(Source: Campbell's Operative Orthopaedics, 15th ed.)
6. Summary: Risk Factor Matrix
| Injury | Key Risk Factors |
|---|---|
| All birth injuries | Macrosomia, shoulder dystocia, forceps/vacuum, maternal diabetes |
| Brachial plexus palsy | Shoulder dystocia, LGA infant, forceps delivery, breech |
| Facial palsy | Forceps delivery, cephalopelvic disproportion |
| Fractures | Macrosomia, breech, instrumented delivery, prematurity, OI |
| HIE | Perinatal asphyxia, placental abruption, cord prolapse, prolonged labor |
| Subgaleal hemorrhage | Vacuum delivery (highest risk) |
In infants of diabetic mothers, birth injury risk is 2-5x higher at any given birth weight class, and the risk is further magnified by instrumental delivery. Tight glycemic control reduces shoulder dystocia by ~60% (Farrar et al. meta-analysis). (Creasy & Resnik's Maternal-Fetal Medicine)
Recent literature note: A 2024 review (PMID 38366382) and a 2026 narrative review (PMID 42080466) in J Hand Surgery (Eur) highlight ongoing advances and controversies in brachial plexus birth injury management, including anatomical predisposition and timing of surgical intervention.
This is a shared conversation. Sign in to Orris to start your own chat.