# COMPREHENSIVE HISTOLOGY OF THE DIGESTIVE TRACT
## TABLE OF CONTENTS
1. General Organization (The Four-Layer Plan)
2. Esophagus
3. Stomach
4. Small Intestine
5. Large Intestine
6. Anal Canal
7. Clinical Correlations Integrated Throughout
---
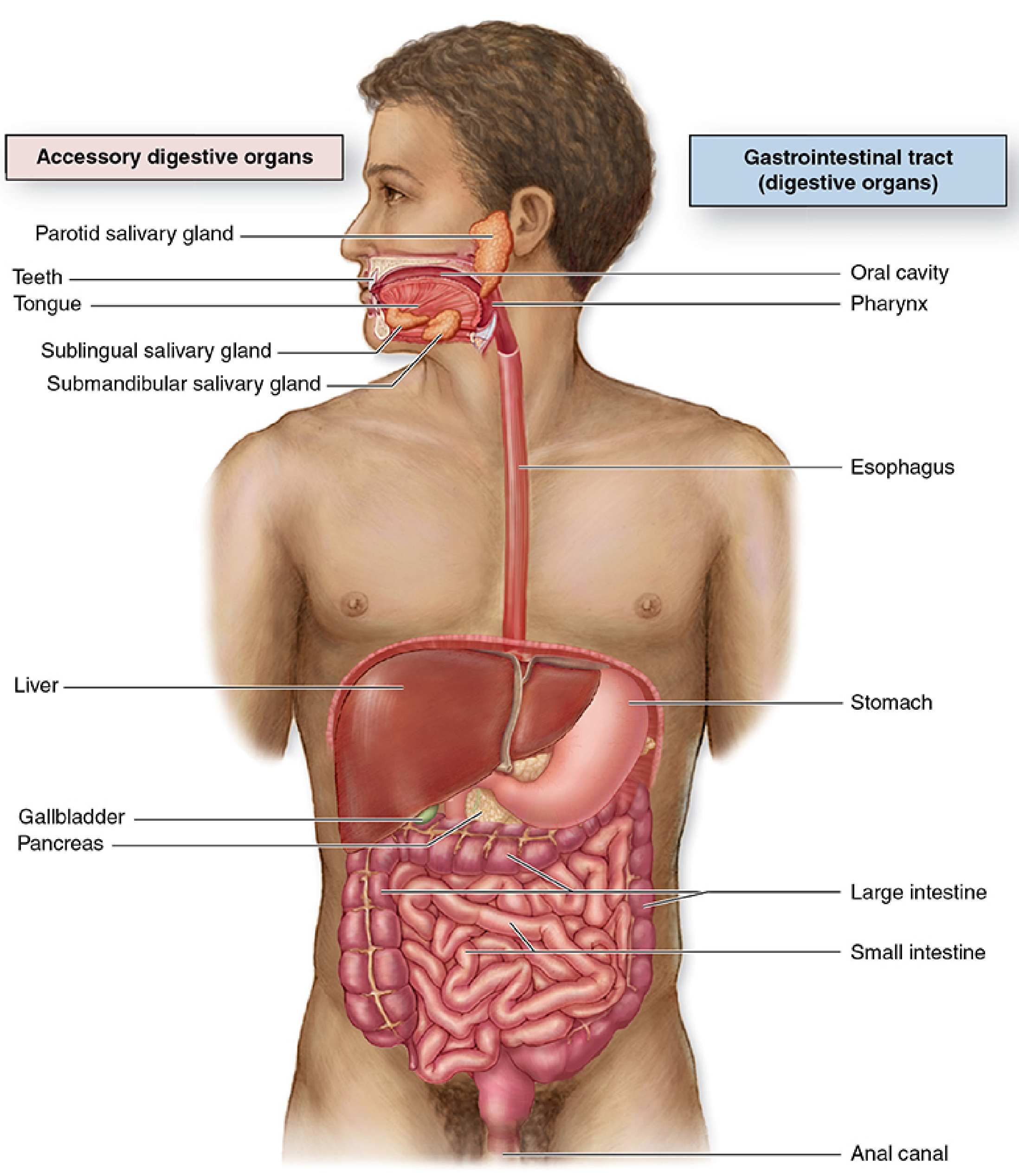
# 1. THE GENERAL PLAN OF THE DIGESTIVE TRACT (GI TUBE)
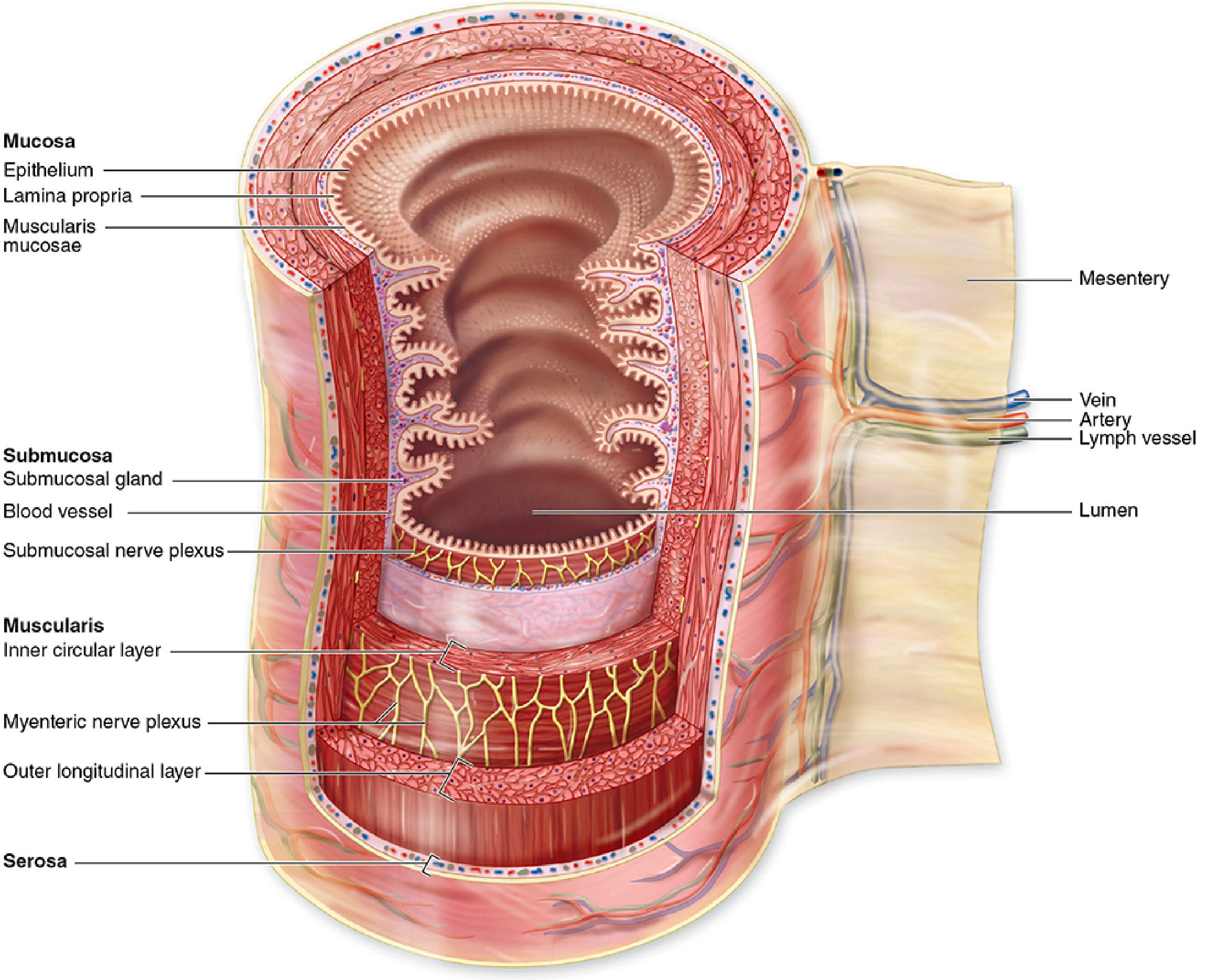
The entire digestive tract, from the esophagus to the anal canal, follows a **common four-layered structural plan** (from lumen outward):
1. **Mucosa**
2. **Submucosa**
3. **Muscularis Externa (Muscularis Propria)**
4. **Serosa or Adventitia**
---
## 1A. MUCOSA (Tunica Mucosa)
The mucosa is the innermost layer and is itself composed of **three sub-layers**:
### i. Epithelium (Lining Epithelium)
- The type of epithelium varies depending on the region of the GI tract.
- It is the surface that faces the lumen.
- Functions include **protection, absorption, secretion**, and **barrier function**.
- The epithelium rests on a **basement membrane** (basal lamina + reticular lamina).
- The epithelium is renewed constantly; GI epithelium is one of the most rapidly renewing tissues in the body, with a turnover time of **3–5 days** in the small intestine.
- **Stem cells** reside in specific niches (e.g., base of crypts in the intestine, isthmus/neck region in the stomach).
> **CLINICAL: Barrett's Esophagus** – The normal stratified squamous epithelium of the lower esophagus is replaced by intestinal-type columnar epithelium with goblet cells (intestinal metaplasia). This is a premalignant condition with a risk of progressing to **esophageal adenocarcinoma**. This is an example of **metaplasia** – a reversible change in which one differentiated cell type is replaced by another.
### ii. Lamina Propria
- This is a layer of **loose (areolar) connective tissue** that lies immediately beneath the epithelium.
- It is rich in:
- **Blood capillaries** and **lymphatic capillaries (lacteals in the small intestine)** – important for absorption of nutrients.
- **Immune cells**: lymphocytes, plasma cells, macrophages, eosinophils, mast cells.
- **GALT (Gut-Associated Lymphoid Tissue)**: scattered lymphocytes, lymphoid nodules (follicles), and in some regions, organized lymphoid structures (e.g., Peyer's patches).
- **Smooth muscle fibers** – isolated strands from the muscularis mucosae extend into the lamina propria (e.g., into villi in the small intestine, facilitating the "villous pump" for lymph drainage).
- **Nerve fibers** and small **ganglion cells**.
- **Fibroblasts** and **extracellular matrix** (collagen type I, III, reticular fibers, ground substance).
- **Glands** in some regions (e.g., gastric glands in the stomach, intestinal glands/crypts of Lieberkühn in the intestine).
> **CLINICAL: Celiac Disease (Celiac Sprue)** – In this autoimmune condition triggered by gluten (gliadin), there is marked **lymphocytic infiltration of the lamina propria** and the epithelium (intraepithelial lymphocytes >25 per 100 enterocytes), leading to villous atrophy, crypt hyperplasia, and malabsorption. The lamina propria becomes densely infiltrated with plasma cells and lymphocytes.
> **CLINICAL: Helicobacter pylori Gastritis** – Chronic infection with H. pylori leads to dense **lymphoplasmacytic infiltration** of the lamina propria of the stomach, with formation of lymphoid follicles (follicular gastritis), which can progress to MALT lymphoma (MALToma).
### iii. Muscularis Mucosae
- The outermost sub-layer of the mucosa.
- Composed of **two thin layers of smooth muscle**:
- **Inner circular layer**
- **Outer longitudinal layer**
- In some regions, a third layer may be present.
- **Functions**:
- Allows independent movement of the mucosa (folding and unfolding).
- Facilitates contact between the epithelium and luminal contents.
- In the small intestine, extensions of smooth muscle from muscularis mucosae into the villi help in the "villous pump" mechanism – rhythmic contraction of the villi aids in propelling lymph (containing absorbed lipids as chylomicrons) from the lacteals toward larger lymphatic vessels.
- **Thickness**: very thin, typically 3–10 smooth muscle cells thick.
> **CLINICAL: Staging of GI cancers (TNM Staging)** – The muscularis mucosae is a **critical landmark** in cancer staging. A carcinoma that has **not penetrated** the muscularis mucosae is classified as **carcinoma in situ (Tis)** or **intramucosal carcinoma** (in some organs, like the colon, intramucosal carcinoma has essentially no metastatic potential because there are no significant lymphatics superficial to the muscularis mucosae). Once the cancer penetrates **through** the muscularis mucosae into the submucosa (**T1**), the risk of lymph node metastasis increases significantly because the submucosa is rich in lymphatic and blood vessels.
---
## 1B. SUBMUCOSA (Tela Submucosa)
- A layer of **moderately dense irregular connective tissue**.
- Much thicker and more robust than the lamina propria.
- Contains:
- **Larger blood vessels** (arteries and veins) – these form the **submucosal vascular plexus (Heller's plexus)**.
- **Lymphatic vessels** – the submucosa is the first layer with significant lymphatic drainage; hence, submucosal invasion by cancer (T1) is clinically significant.
- **Submucosal nerve plexus (Meissner's plexus / plexus of Meissner)**: part of the **enteric nervous system (ENS)**. This plexus contains:
- Ganglion cells (multipolar neurons)
- Schwann cells
- Nerve fibers (both intrinsic and extrinsic)
- It primarily regulates **mucosal secretion** and **submucosal blood flow**, as well as **absorption** and **local muscular movements of the muscularis mucosae**.
- **Glands** – only in **two regions**:
- **Esophagus**: Esophageal glands proper (mucous glands)
- **Duodenum**: Brunner's glands (mucous glands)
- **Adipose tissue** may be present.
- **Immune cells**: lymphocytes, macrophages.
- **Peyer's patches** extend from the lamina propria through the muscularis mucosae into the submucosa in the ileum.
> **CLINICAL: Hirschsprung's Disease (Congenital Aganglionic Megacolon)** – In this condition, there is a **congenital absence of ganglion cells** in the myenteric (Auerbach's) and submucosal (Meissner's) plexuses, usually in the rectosigmoid region. The affected segment cannot relax, leading to a functional obstruction and massive dilation of the proximal normal colon. Diagnosis is confirmed by **suction rectal biopsy** showing **absence of ganglion cells** and **hypertrophied nerve fibers (nerve trunk hypertrophy)** in the submucosa. This is due to failure of neural crest cell migration during embryonic development.
> **CLINICAL: Submucosal (Meissner's) Plexus Damage** – Chagas disease (caused by *Trypanosoma cruzi*) can destroy the ganglion cells in the submucosal and myenteric plexuses, leading to **megaesophagus** and **megacolon**.
The submucosa also forms the structural core of the **plicae circulares (valves of Kerckring)** in the small intestine. These are permanent circular/spiral folds that increase surface area.
---
## 1C. MUSCULARIS EXTERNA (Muscularis Propria)
- Responsible for **peristalsis** and **segmentation** (mixing movements).
- Composed of **two layers of smooth muscle** (in most regions):
- **Inner circular layer**: when contracted, narrows the lumen.
- **Outer longitudinal layer**: when contracted, shortens the tube.
- Between these two muscle layers lies the **Myenteric nerve plexus (Auerbach's plexus)**:
- Part of the enteric nervous system.
- Contains ganglion cells, supporting (glial-like) cells, and nerve fibers.
- Primarily controls **motility** (peristaltic and segmental contractions) of the muscularis externa.
- Receives input from both parasympathetic (vagus nerve – stimulatory; pelvic splanchnic nerves for distal colon/rectum) and sympathetic (inhibitory) divisions.
- In the **stomach**, there are **three layers** of smooth muscle (an additional inner oblique layer).
- In the **large intestine**, the outer longitudinal layer is modified into **three bands called teniae coli** (except in the appendix and rectum, where it is again a complete layer).
- The **upper esophagus** has **skeletal muscle** instead of smooth muscle (explained further below).
> **CLINICAL: Achalasia** – This is a motility disorder of the esophagus characterized by **failure of relaxation of the lower esophageal sphincter (LES)** and **loss of peristalsis** in the distal esophagus. Histologically, there is **loss or degeneration of ganglion cells in the myenteric (Auerbach's) plexus** of the esophagus. In South America, the most common cause is Chagas disease. In North America/Europe, it is usually idiopathic (likely autoimmune). This leads to functional obstruction, dilation of the proximal esophagus, and "bird's beak" appearance on barium swallow.
> **CLINICAL: Myenteric Plexus and Gut Motility** – The interstitial cells of Cajal (ICC) are pacemaker cells located within and around the myenteric plexus. They generate slow-wave electrical rhythms that coordinate smooth muscle contractions. Loss of ICC has been implicated in gastroparesis and chronic intestinal pseudo-obstruction.
> **CLINICAL: Gastrointestinal Stromal Tumors (GISTs)** – These are the most common mesenchymal tumors of the GI tract. They arise from the **interstitial cells of Cajal** or their precursors. They are most commonly found in the stomach (60–70%) and small intestine (20–30%). They characteristically express **CD117 (c-KIT)** and **DOG1**. The discovery of c-KIT mutations led to the targeted therapy with **imatinib (Gleevec)**.
---
## 1D. SEROSA / ADVENTITIA (Outermost Layer)
### Serosa (Tunica Serosa)
- Present where the GI tract is **intraperitoneal** (i.e., suspended by a mesentery and covered by peritoneum).
- Composed of:
- A thin layer of **loose connective tissue** (subserosal connective tissue).
- Covered by a single layer of **simple squamous epithelium** called **mesothelium** (derived from mesoderm).
- The mesothelium secretes a small amount of **serous fluid** that lubricates the surface and reduces friction between abdominal organs.
- Regions covered by serosa: most of the stomach, jejunum, ileum, transverse colon, sigmoid colon, cecum (variable), and upper rectum (partial).
### Adventitia (Tunica Adventitia)
- Present where the GI tract is **retroperitoneal** or where it lacks a mesentery.
- Composed of **ordinary connective tissue** that blends with the connective tissue of surrounding structures.
- **No mesothelial covering**.
- Regions with adventitia: esophagus (most of its length), duodenum (retroperitoneal part), ascending colon, descending colon, middle and lower rectum.
> **CLINICAL: Peritoneal Metastasis** – Once a GI carcinoma invades through the muscularis externa and penetrates the serosa (**T4a** in TNM staging), tumor cells can **exfoliate** into the peritoneal cavity, leading to **peritoneal carcinomatosis** (transcoelomic spread). This is why serosal involvement significantly worsens prognosis.
> **CLINICAL: Peritonitis** – Perforation of the GI tract (e.g., from peptic ulcer, appendicitis, diverticulitis, or trauma) allows luminal contents (bacteria, acid, digestive enzymes) to enter the peritoneal cavity, causing inflammation of the mesothelium (peritonitis), which is a surgical emergency.
---
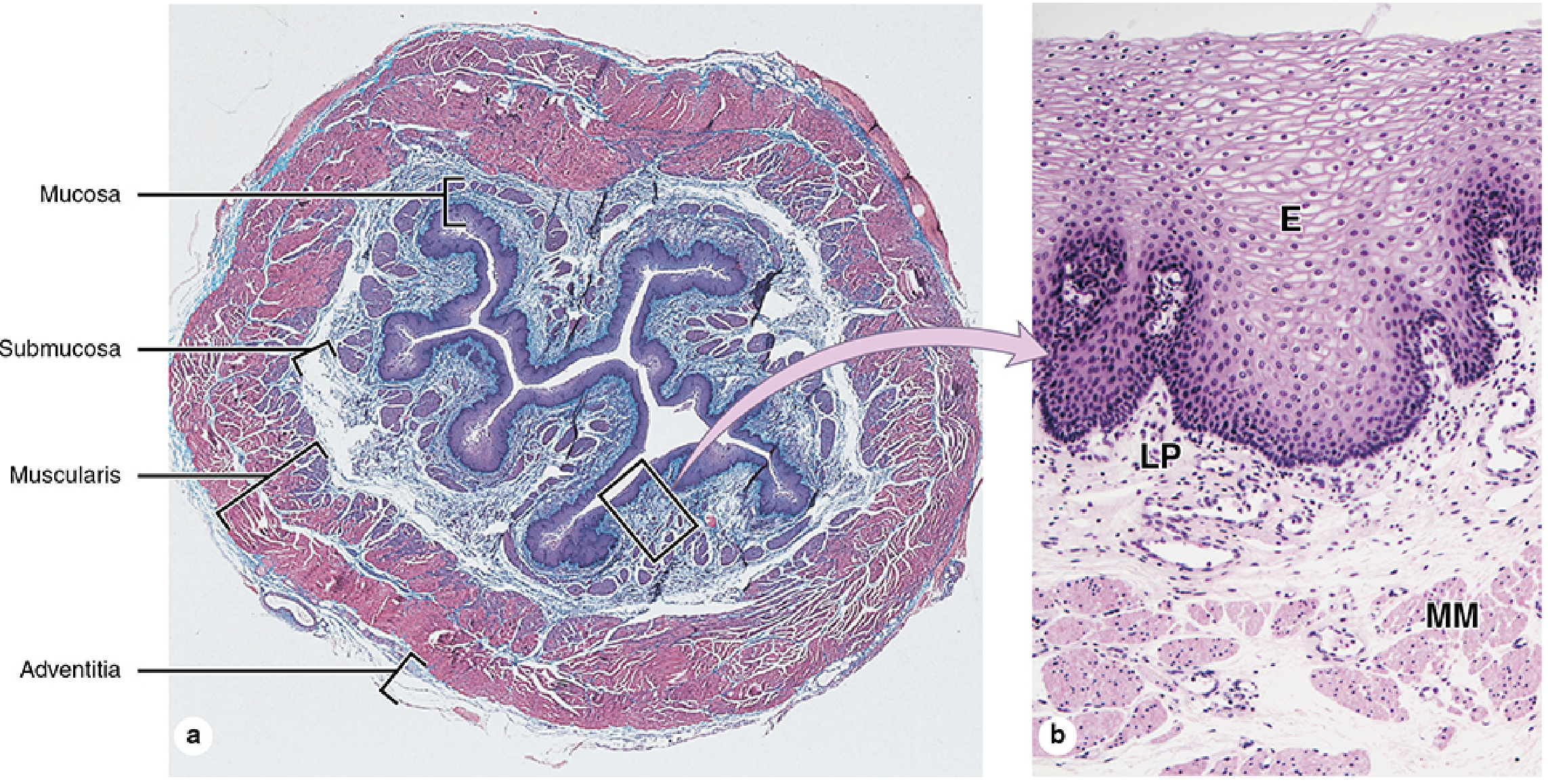
# 2. ESOPHAGUS
## Overview
- A muscular tube (~25 cm long) that connects the pharynx to the stomach.
- Divided into: cervical, thoracic, and abdominal parts.
- Primarily **retroperitoneal**; covered by **adventitia** (except a very short abdominal segment which has serosa).
## Mucosa
### Epithelium
- **Non-keratinized (or slightly parakeratinized) stratified squamous epithelium**.
- This is a **protective epithelium** designed to withstand the abrasion of food bolus passage.
- **Layers of the epithelium (from deep to superficial)**:
- **Stratum basale (basal layer/germinativum)**: A single layer of cuboidal to low columnar cells resting on the basement membrane. These are the **stem cells/progenitor cells** that undergo mitosis and renew the epithelium. They are connected to the basement membrane by hemidesmosomes. The cells contain **keratin intermediate filaments** (mainly keratins K5 and K14).
- **Stratum spinosum (prickle cell layer)**: Multiple layers of polyhedral cells connected by numerous **desmosomes** (which appear as "spines" or "prickles" in histological preparations due to shrinkage artifact). Cells begin to flatten as they move superficially. They express keratins K4 and K13.
- **Stratum superficiale (surface layer)**: Flattened cells that are shed into the lumen. In the esophagus, these cells typically **retain their nuclei** (non-keratinized), although in some individuals or conditions, slight keratinization may be present (parakeratinized).
- **No stratum granulosum or stratum corneum** (as seen in keratinized epithelium of the skin).
- The epithelium is **50–100 μm thick**.
- The basal surface of the epithelium is **undulating**, with connective tissue papillae of the lamina propria projecting into the epithelium (similar to dermal papillae in skin). Normally, these papillae extend to **no more than 50–66% of the total epithelial thickness**. Elongation of papillae is a sign of chronic reflux.
- The epithelium contains scattered **Langerhans cells** (antigen-presenting dendritic cells), **melanocytes** (rarely), and occasional **intraepithelial lymphocytes** (mainly T cells).
> **CLINICAL: Esophageal Squamous Cell Carcinoma** – This is the most common type of esophageal cancer worldwide (especially in the "esophageal cancer belt" – Iran, China, East Africa). Risk factors include alcohol, smoking, hot beverages, achalasia, lye stricture, Plummer-Vinson syndrome, and HPV infection. The tumor arises from the squamous epithelium and commonly occurs in the **middle third** of the esophagus. Histologically, it shows nests and sheets of malignant squamous cells with keratin pearls and intercellular bridges.
> **CLINICAL: Barrett's Esophagus (Detailed)** – Chronic GERD → acid injury → the squamous epithelium of the lower esophagus undergoes **intestinal metaplasia**, replaced by **columnar epithelium with goblet cells**. The goblet cells are the **hallmark**; without goblet cells, the diagnosis of Barrett's is not made (in the American definition; British guidelines may differ). Barrett's can progress through **low-grade dysplasia → high-grade dysplasia → esophageal adenocarcinoma**. Surveillance endoscopy with biopsy is recommended.
> **CLINICAL: Reflux Esophagitis** – Chronic gastroesophageal reflux causes histological changes including: **basal cell hyperplasia** (>15% of epithelial thickness), **elongation of lamina propria papillae** (>66% of epithelial thickness), **infiltration of eosinophils** and **neutrophils** into the epithelium, and **dilated intercellular spaces** (spongiosis) visible on electron microscopy.
> **CLINICAL: Eosinophilic Esophagitis (EoE)** – An allergic/immune-mediated condition characterized by **≥15 eosinophils per high-power field (HPF)** in the esophageal epithelium (peak count). The eosinophils may form **microabscesses**. Clinically presents with dysphagia and food impaction, often in young atopic males. The mucosa shows **rings (trachealization)** and **furrows** on endoscopy.
> **CLINICAL: Esophageal Candidiasis** – In immunocompromised patients (HIV/AIDS, on immunosuppressants), *Candida albicans* can invade the squamous epithelium. Histologically, **pseudohyphae and yeast forms** are seen within the superficial layers of the epithelium. PAS or GMS stains highlight the organisms.
### Lamina Propria
- Loose connective tissue with blood vessels, scattered lymphocytes, and occasional small mucous glands called **esophageal cardiac glands** (found in two regions):
- Near the **upper esophageal sphincter** (near the cricoid cartilage).
- Near the **lower esophageal sphincter** (near the gastroesophageal junction).
- These glands resemble the cardiac glands of the stomach and secrete **mucus** and **lysozyme**, providing protection and lubrication.
- They open onto the surface via short ducts.
### Muscularis Mucosae
- **Uniquely thick** in the esophagus compared to other regions of the GI tract.
- Consists of only a **longitudinal layer** of smooth muscle (no circular layer initially). In the upper esophagus, it begins as scattered fascicles and becomes a continuous layer distally.
- At the gastroesophageal junction, it becomes the typical two-layered muscularis mucosae (inner circular + outer longitudinal).
## Submucosa
- **Dense irregular connective tissue** with collagen and elastic fibers.
- Contains the **esophageal glands proper** (also called **submucosal glands**):
- These are **compound tubuloalveolar glands** that secrete **mucus**.
- The mucus is **acidic** (sulfated and carboxylated mucins) and lubricates the esophageal lumen, facilitating bolus passage.
- The ducts of these glands penetrate through the muscularis mucosae and lamina propria to open onto the epithelial surface.
- The glands are scattered throughout the submucosa but are most numerous in the **upper half** of the esophagus.
- **Cell types in the glands**:
- Mucous cells (predominant)
- Serous cells (less common)
- Occasional myoepithelial cells surrounding the secretory units
- The submucosa also contains the **submucosal venous plexus**.
> **CLINICAL: Esophageal Varices** – In **portal hypertension** (most commonly due to liver cirrhosis), blood is shunted from the portal system to the systemic venous system via portosystemic anastomoses. One such anastomosis is between the **left gastric vein** (portal) and the **esophageal veins** draining into the **azygos system** (systemic), located in the **submucosal venous plexus** of the lower esophagus. This leads to **dilated, tortuous submucosal veins (varices)**. Rupture of varices causes **massive, life-threatening upper GI hemorrhage**. Histologically, the submucosa shows markedly dilated thin-walled venous channels.
- **Meissner's plexus** is present in the submucosa.
## Muscularis Externa
- **Two layers**: inner circular and outer longitudinal (standard arrangement).
- **Unique feature**: The composition of muscle changes along the length:
- **Upper third (approximately)**: **Skeletal muscle** (striated) in both layers. This is a continuation of the pharyngeal musculature and is responsible for the voluntary initiation of swallowing.
- **Middle third**: **Mixed skeletal and smooth muscle**. The skeletal muscle fibers are gradually replaced by smooth muscle.
- **Lower third**: **Entirely smooth muscle**. Peristalsis here is involuntary.
- The **myenteric (Auerbach's) plexus** is located between the two muscle layers.
- The **lower esophageal sphincter (LES)** is a **physiological sphincter** (not a true anatomical sphincter, although there is some thickening of the circular muscle). It maintains a tonic contraction to prevent reflux.
> **CLINICAL: Achalasia (Additional Detail)** – In achalasia, the myenteric plexus in the lower esophagus shows **loss of ganglion cells** and **inflammation** (particularly in early stages). The inhibitory neurons (those that release VIP and nitric oxide, responsible for LES relaxation) are preferentially lost. The remaining excitatory neurons (cholinergic) are relatively preserved, leading to an unopposed contraction of the LES. Treatment includes pneumatic dilation, Heller myotomy, or peroral endoscopic myotomy (POEM).
> **CLINICAL: Zenker's Diverticulum** – This is a **false diverticulum** (pulsion diverticulum) that occurs through **Killian's triangle** (a weak area between the thyropharyngeal and cricopharyngeal parts of the inferior pharyngeal constrictor). The mucosa and submucosa herniate through the muscular wall. It occurs at the **pharyngoesophageal junction** (technically a pharyngeal diverticulum but clinically grouped with esophageal diverticula). The wall of the diverticulum contains only mucosa and submucosa (no muscularis externa).
> **CLINICAL: Mallory-Weiss Tear** – Severe retching/vomiting (often in alcoholics or patients with bulimia) causes a **longitudinal mucosal tear** at the **gastroesophageal junction**. This tear extends through the mucosa (epithelium, lamina propria, muscularis mucosae) and may extend into the submucosa. It causes upper GI bleeding. A **Boerhaave syndrome** is a full-thickness perforation (transmural tear) of the esophagus, which is a surgical emergency.
## Adventitia
- The esophagus is surrounded by **adventitia** (loose connective tissue blending with surrounding mediastinal structures) for most of its length.
- The very short **abdominal portion** of the esophagus (below the diaphragm) is covered by **serosa** (visceral peritoneum).
---
## GASTROESOPHAGEAL (GE) JUNCTION (Z-LINE / ORA SERRATA)
- This is the junction between the esophageal epithelium and the gastric (cardiac) epithelium.
- **Abrupt transition** from **stratified squamous (non-keratinized)** epithelium to **simple columnar** epithelium.
- Endoscopically visible as an irregular line called the **Z-line** (squamocolumnar junction, SCJ).
- This junction normally lies at or near the level of the diaphragmatic hiatus.
> **CLINICAL: In Barrett's esophagus**, the Z-line migrates proximally (upward). Biopsy of the area above the normal Z-line showing intestinal metaplasia with goblet cells confirms the diagnosis.
> **CLINICAL: Junctional (Siewert) Tumors** – Adenocarcinomas arising at the GE junction are classified by the Siewert classification (Type I, II, III) based on the location of the tumor center relative to the Z-line. These tumors are increasing in incidence in Western countries, associated with obesity and GERD.
---
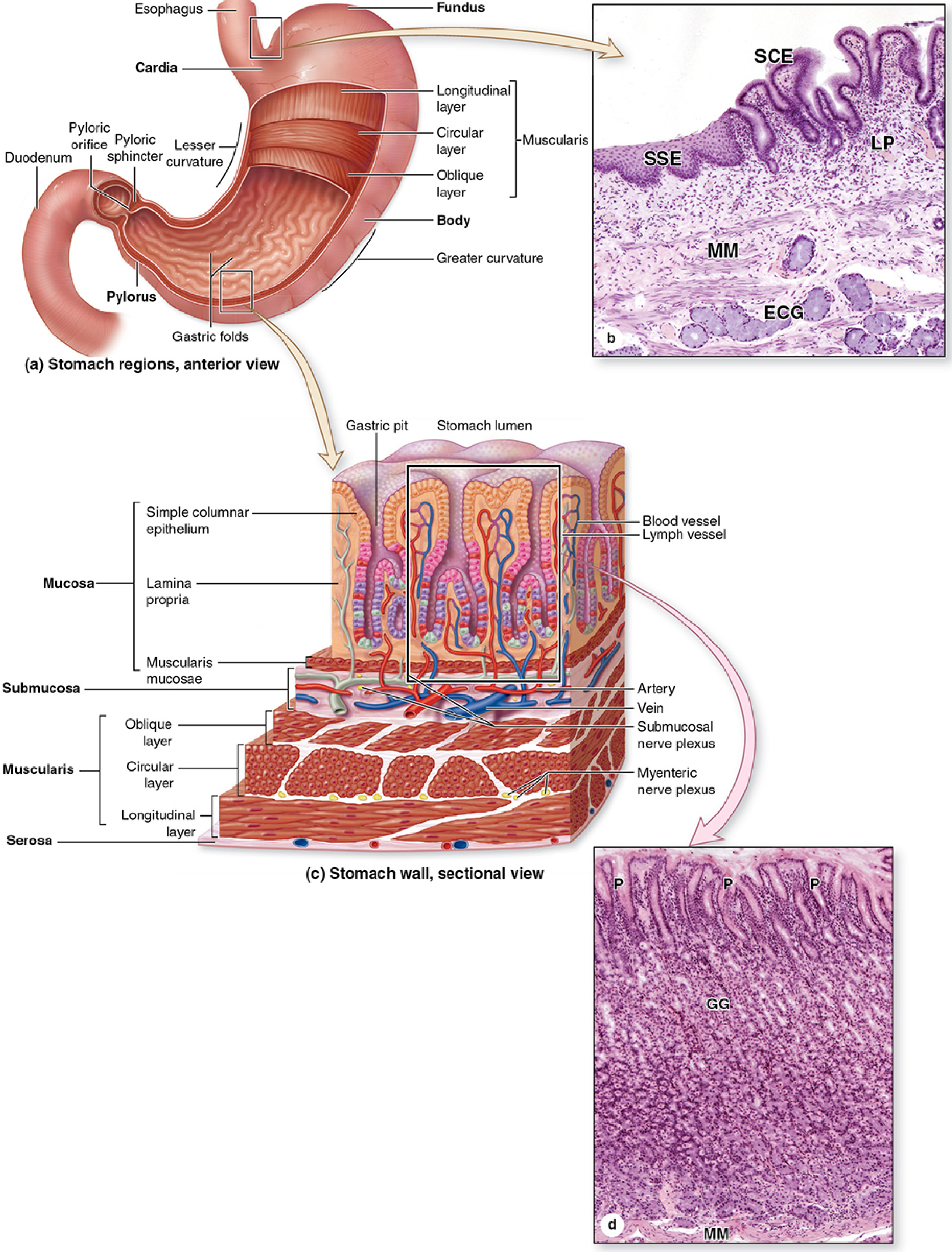
# 3. STOMACH
## Overview
- The stomach is divided (histologically relevant) into:
- **Cardia**: narrow zone near the GE junction
- **Fundus and Body**: largest part, with characteristic gastric glands
- **Pylorus (Pyloric antrum and pyloric canal)**: distal part with pyloric glands
- The surface of the stomach has visible **rugae** (large folds involving mucosa AND submucosa, which flatten when the stomach distends), **areae gastricae** (small 1–6 mm irregular patches on the mucosal surface), and **gastric pits (foveolae gastricae)** (invaginations of the surface epithelium into which the gastric glands open).
## Mucosa
### Epithelium
- **Simple columnar epithelium** – uniform throughout the entire stomach.
- The cells are called **surface mucous cells (foveolar cells)**.
- They are tall columnar cells with:
- **Basally placed, flattened nuclei**.
- **Apical cytoplasm filled with mucous granules** (pale-staining in H&E; strongly PAS-positive because they contain neutral glycoproteins).
- The mucus is **visible (not dissolved)** in H&E sections, appearing as a clear/pale zone above the nucleus.
- They secrete a **thick, viscous, alkaline mucus** that forms a **mucus-bicarbonate barrier** protecting the gastric epithelium from the highly acidic (pH 1–2) and proteolytic luminal environment.
- The mucus layer is approximately **1 mm thick** and maintains a pH gradient from ~1–2 at the luminal surface to ~7 at the epithelial cell surface.
- **Turnover**: Surface mucous cells are replaced every **3–5 days** – one of the fastest turnover rates in the body.
> **CLINICAL: NSAIDs and Gastric Mucosal Injury** – NSAIDs (aspirin, ibuprofen) inhibit **cyclooxygenase (COX)**, particularly **COX-1**, which is responsible for producing **prostaglandins E2 and I2**. These prostaglandins stimulate mucus and bicarbonate secretion, promote mucosal blood flow, and inhibit acid secretion. NSAID use reduces the mucus-bicarbonate barrier, making the mucosa vulnerable to acid-peptic damage → **gastric erosions and ulcers**.
> **CLINICAL: Peptic Ulcer Disease** – Ulcers are defects that penetrate through the **muscularis mucosae** (as opposed to erosions, which are superficial and do not penetrate the muscularis mucosae). The base of a peptic ulcer shows four zones histologically (from lumen to base): (1) **necrotic/fibrinous debris**, (2) **non-specific inflammatory infiltrate** (neutrophils), (3) **granulation tissue** (neovascularization, fibroblasts), (4) **fibrosis/scar tissue**. Ulcer complications include hemorrhage (erosion into vessels, especially the gastroduodenal artery for posterior duodenal ulcers), perforation, penetration, and gastric outlet obstruction.
### Gastric Pits (Foveolae)
- These are **invaginations** of the surface epithelium into the lamina propria.
- They are lined by the same **surface mucous cells**.
- **Depth varies by region**:
- **Cardia**: pits occupy about **50%** of the mucosal thickness
- **Fundus/Body**: pits occupy about **25%** of the mucosal thickness (shallow pits, long glands)
- **Pylorus**: pits occupy about **50%** (or more) of the mucosal thickness (deep pits, shorter glands)
- At the base of the pits, the gastric glands open.
### Gastric Glands
Three types based on region:
---
#### A. CARDIAC GLANDS (Cardia Region)
- Found in a narrow zone (0.5–3 cm) around the GE junction.
- **Simple or branched tubular glands**.
- Composed predominantly of **mucus-secreting cells** (similar to pyloric mucous cells).
- May contain occasional **enteroendocrine cells**.
- The glands are coiled and often have a wide lumen.
- **Clinical note**: The cardiac glands may contain parietal cells; some authors consider the cardia to be a transitional zone.
> **CLINICAL: Carditis** – Inflammation of the cardia mucosa is common in GERD and H. pylori infection. The presence of intestinal metaplasia in the cardia may be a risk factor for cardia adenocarcinoma.
---
#### B. FUNDIC (OXYNTIC) GLANDS (Fundus and Body – the majority of the stomach)
- **Straight, tubular, slightly branched glands** that extend from the base of the gastric pits to the muscularis mucosae.
- Each gland has three parts:
- **Isthmus** (opening into the pit)
- **Neck**
- **Base (fundus of the gland)**
- The glands are densely packed, separated by minimal lamina propria.
- **Cell types (from surface to base)**:
##### 1. Surface Mucous Cells
- Line the surface and pits (described above).
##### 2. Mucous Neck Cells
- Located in the **neck** region of the gland (between isthmus and base).
- **Irregular, shorter** cells compared to surface mucous cells.
- Contain **acidic mucins** (in contrast to the neutral mucins of surface mucous cells). Hence, they stain differently:
- Surface mucous cells: PAS-positive (neutral mucins)
- Mucous neck cells: **mucicarmine and Alcian blue-positive** (acidic mucins)
- Their mucus granules are **smaller** and more basophilic.
- They are interspersed among parietal cells.
- They are thought to be **precursors/stem cells** for other cell types in the gland (the **stem cell zone** is at the **isthmus/neck** junction).
- They also differentiate into **surface mucous cells** (which migrate upward) and into **parietal cells, chief cells, and enteroendocrine cells** (which migrate downward).
##### 3. Parietal Cells (Oxyntic Cells)
- Found predominantly in the **upper half** of the gland (isthmus and neck), but can be found throughout.
- **Large, pyramidal or triangular** cells that bulge from the gland wall.
- **Eosinophilic (intensely pink)** cytoplasm in H&E due to abundant **mitochondria** (which occupy ~40% of the cell volume – one of the highest mitochondrial concentrations of any cell type).
- **Centrally placed, round nucleus**.
- **Key ultrastructural feature**: **Intracellular canaliculus** – an extensive invagination of the apical plasma membrane that penetrates deep into the cell. When the cell is **resting (unstimulated)**, the cytoplasm contains numerous **tubulovesicles** (membrane-bound vesicles). When **stimulated** (by histamine, ACh, or gastrin), the tubulovesicles **fuse with the intracellular canaliculus**, dramatically increasing the surface area available for acid secretion. The canalicular membrane is densely studded with **H⁺/K⁺-ATPase (proton pump)**.
- **Functions**:
1. **HCl secretion**: The proton pump (H⁺/K⁺-ATPase) secretes H⁺ ions into the lumen in exchange for K⁺. Cl⁻ ions are transported through Cl⁻ channels. This generates **hydrochloric acid** with a pH as low as ~0.8 within the canaliculus.
2. **Intrinsic factor (IF) secretion**: Essential for vitamin B12 (cobalamin) absorption in the **terminal ileum**. IF binds vitamin B12, and the IF-B12 complex is absorbed by specific receptors (cubilin) on the ileal enterocytes.
- **Stimulation of acid secretion** involves three pathways:
- **Histamine** (from ECL cells) → H2 receptors → cAMP pathway
- **Acetylcholine** (from vagus nerve/enteric neurons) → M3 muscarinic receptors → Ca²⁺ pathway
- **Gastrin** (from G cells in pyloric antrum) → CCK-B receptors → Ca²⁺ pathway (mainly acts indirectly via ECL cells)
- **Inhibition**: Somatostatin (from D cells), prostaglandins, secretin, GIP
> **CLINICAL: Pernicious Anemia** – An autoimmune condition in which **antibodies against parietal cells** and/or **intrinsic factor** are produced. Destruction of parietal cells leads to:
> - **Achlorhydria** (loss of HCl production)
> - **Loss of intrinsic factor** → inability to absorb vitamin B12 in the terminal ileum → **megaloblastic (macrocytic) anemia**, **subacute combined degeneration of the spinal cord** (posterior columns and lateral corticospinal tracts), and **glossitis**
> - **Atrophic gastritis** (Type A autoimmune gastritis) – affecting the **body/fundus** (where parietal cells are located)
> - **Compensatory hypergastrinemia** (loss of acid removes negative feedback on G cells) → ECL cell hyperplasia → risk of **gastric carcinoid tumors (Type 1 gastric neuroendocrine tumors)**
> **CLINICAL: Proton Pump Inhibitors (PPIs)** – Omeprazole, esomeprazole, lansoprazole etc. irreversibly block the **H⁺/K⁺-ATPase** on the parietal cell. They are the most potent inhibitors of acid secretion. Long-term use can cause hypergastrinemia (due to loss of acid feedback) and ECL cell hyperplasia. There are theoretical concerns about carcinoid risk, though this is not firmly established in humans.
> **CLINICAL: H2 Receptor Blockers** – Ranitidine, famotidine block histamine H2 receptors on parietal cells, reducing acid secretion.
> **CLINICAL: Zollinger-Ellison Syndrome** – A gastrin-secreting tumor (gastrinoma), usually located in the pancreas or duodenum (gastrinoma triangle), causes massive hypergastrinemia → extreme hypersecretion of gastric acid → severe/multiple peptic ulcers (often in unusual locations like jejunum), diarrhea, and parietal cell hyperplasia.
##### 4. Chief Cells (Peptic Cells / Zymogenic Cells)
- Located predominantly in the **lower half/base** of the fundic glands.
- **Columnar cells** with:
- **Basally placed, round nucleus**
- **Basophilic basal cytoplasm** (due to extensive **rough endoplasmic reticulum (RER)** – characteristic of protein-secreting cells)
- **Apical cytoplasm filled with zymogen granules** (secretory granules containing **pepsinogen**) – these appear as pale/eosinophilic granules but may be washed out during fixation, leaving a foamy/vacuolated appearance.
- Well-developed **Golgi apparatus** (supranuclear).
- **Functions**:
- Secrete **pepsinogen** (inactive zymogen) → converted to **pepsin** (active protease) by HCl in the gastric lumen (autocatalytic at pH < 5).
- Also secrete **gastric lipase** (functions at acidic pH, important in neonates).
- Chief cells are stimulated by **vagal stimulation (ACh)**, **secretin**, and **CCK**.
> **CLINICAL: Chief Cell Tumors** – Rare. Chief cell hyperplasia is not typically a significant clinical entity.
##### 5. Enteroendocrine Cells
- Scattered throughout the gland, especially at the base.
- Part of the **diffuse neuroendocrine system (DNES)**.
- Previously called **APUD cells** (Amine Precursor Uptake and Decarboxylation).
- They are typically **small, triangular** cells with basally located **secretory granules** (hence also called **basal-granulated cells**).
- They are difficult to identify on routine H&E; they require **immunohistochemistry** or **silver staining** (argentaffin and argyrophilic reactions) for identification.
- Types include:
- **ECL cells (Enterochromaffin-like cells)**: The most abundant enteroendocrine cell in the fundic mucosa. They secrete **histamine** in response to **gastrin**. Histamine then acts on **H2 receptors** on parietal cells to stimulate acid secretion. They are crucial intermediaries in acid secretion.
- **D cells**: Secrete **somatostatin**, which inhibits acid secretion by acting on parietal cells, G cells, and ECL cells. Somatostatin is a paracrine inhibitor.
- **EC cells (Enterochromaffin cells)**: Secrete **serotonin (5-HT)**, which affects gut motility.
- **A cells (X/A-like cells)**: Secrete **ghrelin** (the "hunger hormone"), predominantly in the fundus.
> **CLINICAL: Gastric Neuroendocrine Tumors (Carcinoids)** – These tumors arise from enteroendocrine cells, particularly **ECL cells** in the fundus/body. Three types:
> - **Type 1** (most common, ~75%): Associated with autoimmune (Type A) atrophic gastritis and hypergastrinemia. Multiple small tumors. Low malignant potential.
> - **Type 2**: Associated with MEN-1/Zollinger-Ellison syndrome and hypergastrinemia. Low-intermediate malignant potential.
> - **Type 3**: Sporadic, gastrin-independent. Single, large. High malignant potential.
##### 6. Stem Cells
- Located in the **isthmus** of the fundic gland.
- They are undifferentiated cells that continuously divide and give rise to all cell types of the gastric gland and surface epithelium.
- **Upward differentiation**: into surface mucous cells (migrate upward and are shed from the surface after ~3–5 days).
- **Downward differentiation**: into mucous neck cells, parietal cells, chief cells, and enteroendocrine cells (these cells have a longer lifespan; parietal cells live ~150–200 days).
---
#### C. PYLORIC GLANDS (Pyloric Antrum and Canal)
- **Branched, coiled tubular glands**.
- The gastric pits are **deep** (occupy ~50% or more of the mucosal thickness), and the glands are **shorter** than fundic glands.
- The glands are predominantly composed of **mucus-secreting cells** (resembling mucous neck cells). The secretion is **viscous and alkaline**.
- **No parietal cells or chief cells** (or very few).
- **Important enteroendocrine cells**:
- **G cells**: The most important cell in the pyloric mucosa from a physiological standpoint. They secrete **gastrin** into the bloodstream (endocrine secretion). Gastrin stimulates parietal cells (directly and via ECL cells) and has a trophic effect on the gastric mucosa. G cells are **open-type** enteroendocrine cells – their apical surface reaches the lumen to sense the chemical composition (especially amino acids and peptides) of the luminal contents.
- **D cells**: Secrete somatostatin. The D cells in the antrum are also **open-type** and sense luminal pH. When pH drops below ~3, D cells release somatostatin, which inhibits adjacent G cells (paracrine inhibition). This is a key negative feedback mechanism.
> **CLINICAL: H. pylori and Gastrin** – H. pylori colonizes the antral mucosa (primarily), causing chronic inflammation. The organism produces **urease** (which generates ammonia, raising local pH), **VacA** and **CagA** toxins. The infection suppresses D cells (reducing somatostatin) and stimulates G cells (increasing gastrin), leading to **hypergastrinemia → increased acid secretion → peptic ulcer disease** (especially duodenal ulcers). In contrast, when H. pylori involves the body/fundus (pangastritis), it destroys parietal cells, reducing acid output and increasing the risk of **gastric adenocarcinoma** and **gastric MALT lymphoma**.
> **CLINICAL: Gastric Adenocarcinoma** – The most common malignant tumor of the stomach.
> - **Intestinal type (Lauren classification)**: Well-differentiated, forms glands, associated with intestinal metaplasia, chronic H. pylori gastritis, and environmental factors (diet, smoking). More common in high-incidence areas (East Asia). Follows the metaplasia-dysplasia-carcinoma sequence: chronic gastritis → atrophic gastritis → intestinal metaplasia → dysplasia → carcinoma.
> - **Diffuse type**: Poorly differentiated, composed of **signet ring cells** (cells with a large intracellular mucin vacuole that pushes the nucleus to the periphery). Often associated with loss of **E-cadherin** (CDH1 gene mutation). Causes diffuse wall thickening → **linitis plastica (leather bottle stomach)**. Not associated with intestinal metaplasia; may be hereditary (hereditary diffuse gastric cancer – HDGC).
### Lamina Propria of the Stomach
- Very scanty between the densely packed gastric glands.
- Contains:
- Reticular fibers (provide support)
- Blood capillaries
- Lymphocytes, plasma cells (physiological low-grade inflammation; any significant increase is pathological)
- Occasional lymphoid follicles (increased with H. pylori infection)
- Smooth muscle strands from the muscularis mucosae
### Muscularis Mucosae of the Stomach
- Typical two layers (inner circular, outer longitudinal).
- May have a third layer in some areas.
- Sends fine smooth muscle strands upward between the glands.
## Submucosa of the Stomach
- Dense irregular connective tissue.
- Contains larger blood vessels, lymphatics, Meissner's plexus.
- **No glands** (unlike esophagus and duodenum).
- The submucosa forms the **core of the rugae** (along with the mucosa).
## Muscularis Externa of the Stomach
- **Three layers** (unique to the stomach):
1. **Inner oblique layer** (the additional layer; incomplete, most prominent in the body)
2. **Middle circular layer** (thickens at the pylorus to form the **pyloric sphincter** – a true anatomical sphincter)
3. **Outer longitudinal layer**
- **Myenteric (Auerbach's) plexus** lies between the circular and longitudinal layers.
- The three muscle layers provide for the powerful churning and mixing movements of the stomach.
> **CLINICAL: Pyloric Stenosis (Infantile Hypertrophic Pyloric Stenosis)** – This condition (typically occurring in male infants, 2–8 weeks old) is characterized by **marked hypertrophy and hyperplasia of the circular smooth muscle** of the pylorus. The thickened pylorus feels like an "olive" on physical examination. Histologically, the smooth muscle fibers are hypertrophied. Treatment is Ramstedt pyloromyotomy (surgical splitting of the thickened muscle down to the submucosa).
> **CLINICAL: Gastric Motility** – The interstitial cells of Cajal (ICC) in the muscularis externa generate pacemaker potentials (slow waves) at ~3 cycles/minute in the stomach. The stomach's motility includes receptive relaxation (fundus), peristaltic contractions (body and antrum for mixing), and gastric emptying (regulated by pyloric sphincter).
## Serosa of the Stomach
- The stomach is an intraperitoneal organ (completely covered by visceral peritoneum).
- The serosa is continuous with the **greater omentum** and **lesser omentum**.
---
# 4. SMALL INTESTINE
## Overview
The small intestine is the **primary site of digestion and absorption**. It is ~6 meters long and is divided into:
- **Duodenum** (~25 cm) – mostly retroperitoneal
- **Jejunum** (~2.5 m) – intraperitoneal
- **Ileum** (~3.5 m) – intraperitoneal
## Surface Area Amplification
The small intestine has an enormous absorptive surface area (~200 m², roughly the size of a tennis court), achieved by three levels of structural modification:
1. **Plicae circulares (valves of Kerckring / circular folds)**:
- **Permanent** transverse/spiral folds of the mucosa AND submucosa.
- Most prominent in the **distal duodenum and jejunum**; diminish in the ileum; absent in the proximal duodenum and distal ileum.
- Increase surface area by ~3×.
- They slow the passage of chyme, allowing more time for absorption.
2. **Villi**:
- **Finger-like or leaf-like projections** of the mucosa (epithelium + lamina propria core; **no submucosa** in villi).
- Height: 0.5–1.5 mm.
- Shape varies by region:
- **Duodenum**: broad, leaf-shaped (spatulate)
- **Jejunum**: tall, finger-like (the tallest villi)
- **Ileum**: shorter, finger-like
- Each villus has:
- **Epithelial covering** (absorptive cells + goblet cells)
- **Core of lamina propria** containing:
- A **central lacteal** (blind-ended lymphatic capillary) – for absorption of lipids (as chylomicrons)
- A **capillary network** (fenestrated capillaries – for absorption of amino acids, sugars, etc.)
- **Smooth muscle strands** from the muscularis mucosae (contract rhythmically to shorten the villus, pumping lymph from the lacteal – the "villous pump")
- **Fibroblasts**, **immune cells** (lymphocytes, macrophages, eosinophils, mast cells, plasma cells)
- Increase surface area by ~10×.
3. **Microvilli (brush border / striated border)**:
- Microscopic projections (~1 μm long) on the apical surface of each absorptive cell (enterocyte).
- Each enterocyte has ~3,000 microvilli.
- Core of **actin filaments** (bundled by villin, fimbrin; attached to terminal web by myosin).
- Covered by a **glycocalyx** (carbohydrate-rich surface coat composed of glycoproteins and glycolipids).
- The glycocalyx contains:
- **Digestive enzymes**: disaccharidases (lactase, maltase, sucrase-isomaltase), peptidases (aminopeptidases, dipeptidases), and alkaline phosphatase.
- These enzymes perform the **final steps of digestion** (terminal/membrane digestion) at the brush border surface.
- Increase surface area by ~20×.
> **CLINICAL: Lactase Deficiency (Lactose Intolerance)** – Lactase is a brush border enzyme (on microvilli of enterocytes) that cleaves lactose (milk sugar) into glucose and galactose. Deficiency of lactase (most commonly primary adult-type hypolactasia – a normal developmental decline in lactase after weaning, especially in non-Northern European populations) leads to undigested lactose reaching the colon, where bacteria ferment it, producing gas (H₂, CO₂, CH₄) and osmotically active products → **bloating, flatulence, osmotic diarrhea, abdominal cramping**. Diagnosis: hydrogen breath test. The lactase enzyme is located on the tips of the villi; hence villous damage (e.g., celiac disease, viral gastroenteritis) can cause **secondary lactase deficiency**.
## Mucosa
### Epithelium
- **Simple columnar epithelium** with several cell types:
#### 1. Absorptive Cells (Enterocytes)
- The **most abundant cell type**.
- Tall columnar cells with:
- **Oval, basally placed nucleus**
- **Prominent brush border (microvilli)** on the apical surface – visible with light microscopy as a **striated border**
- **Well-developed terminal web** (meshwork of actin and intermediate filaments beneath the microvilli)
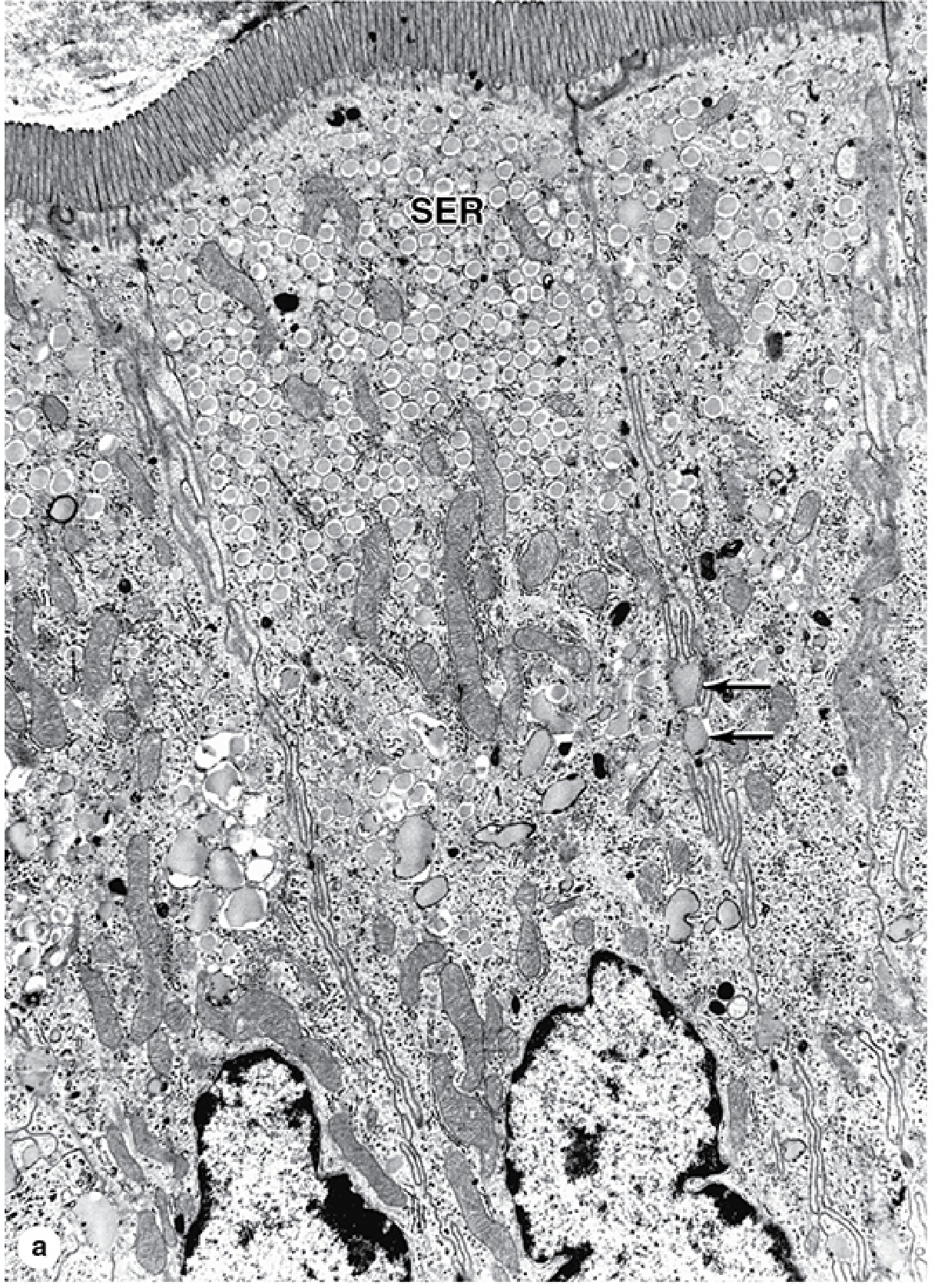
- Abundant **smooth ER** (for lipid absorption and processing)
- **Rough ER** and **Golgi apparatus** (for synthesis of enzymes and glycocalyx components)
- **Mitochondria** (for energy-dependent transport)
- Tight junctions (zonulae occludentes) connect adjacent cells at their apical surfaces, creating a barrier that regulates paracellular transport
- Junctional complex (zonula occludens, zonula adherens, macula adherens/desmosome) at the apical lateral border
- **Function**: Absorption of nutrients – sugars, amino acids, fatty acids, monoglycerides, vitamins, electrolytes, water.
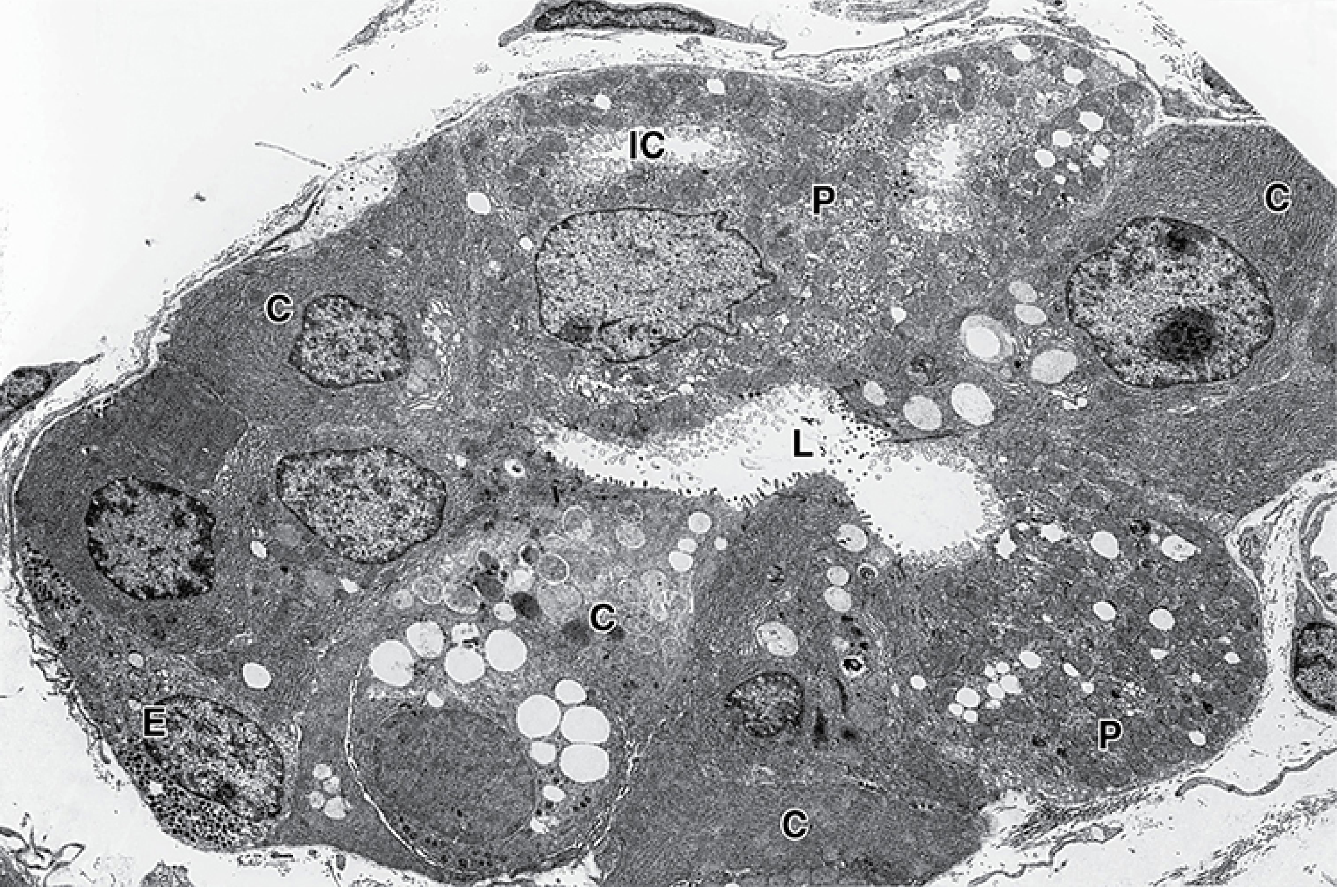
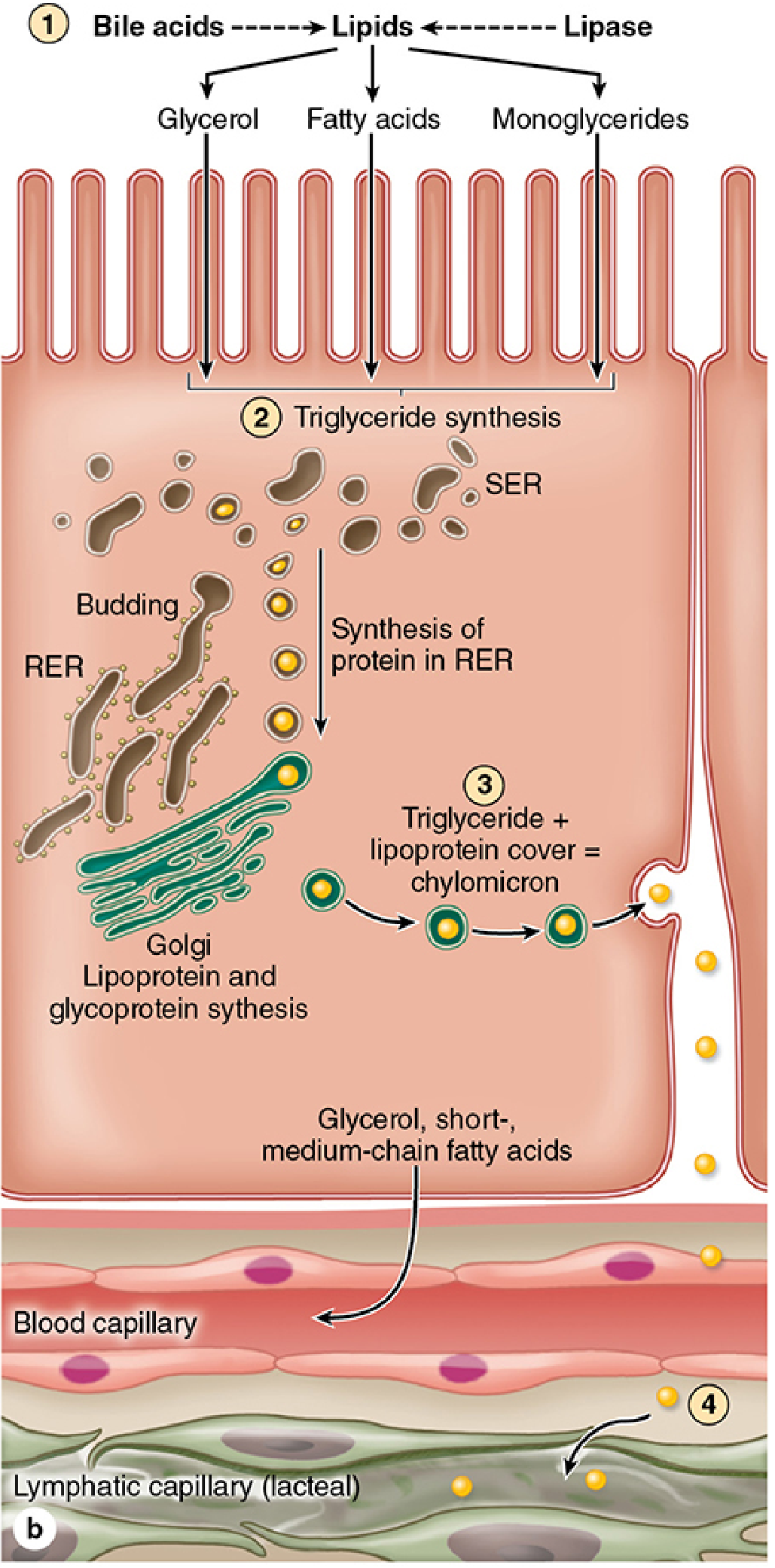
- **Lipid absorption** is unique:
- Fatty acids and monoglycerides enter the cell, are re-esterified to **triglycerides** in the smooth ER.
- Triglycerides are packaged with cholesterol, phospholipids, and apolipoproteins into **chylomicrons** (in the Golgi).
- Chylomicrons are exocytosed from the basolateral surface and enter the **lacteals** (not capillaries – too large).
- Short-chain and medium-chain fatty acids can enter capillaries directly.
> **CLINICAL: Abetalipoproteinemia** – A rare autosomal recessive condition with mutations in the **microsomal triglyceride transfer protein (MTP)**. Enterocytes cannot form chylomicrons. Histologically, the enterocytes appear **vacuolated** (lipid-laden) because absorbed fat accumulates but cannot be exported. Results in fat malabsorption, steatorrhea, failure to thrive, and deficiency of fat-soluble vitamins (A, D, E, K).
> **CLINICAL: Celiac Disease (Gluten-Sensitive Enteropathy) – Detailed Histology** – An immune-mediated reaction to gluten (specifically gliadin peptides) in genetically susceptible individuals (HLA-DQ2 or HLA-DQ8). The histological hallmark (Marsh classification) includes:
> - **Marsh 0**: Normal (pre-infiltrative)
> - **Marsh 1**: Increased **intraepithelial lymphocytes (IELs)** (>25 IELs per 100 enterocytes; normal <25). These are mainly CD8+ T cells.
> - **Marsh 2**: IEL increase + **crypt hyperplasia** (elongated, hyperplastic crypts with increased mitoses)
> - **Marsh 3a-c**: IEL increase + crypt hyperplasia + **villous atrophy** (partial to total)
> - **Marsh 3c**: Total villous atrophy – the mucosa becomes flat; the villi are completely absent.
> - The lamina propria shows increased **plasma cells, lymphocytes, eosinophils, and mast cells**.
> - Loss of brush border (reduced disaccharidases, including lactase – secondary lactase deficiency).
> - **Serology**: Anti-tissue transglutaminase (anti-tTG) IgA antibodies (most sensitive), anti-endomysial (anti-EMA) IgA antibodies (most specific), anti-deamidated gliadin peptide (anti-DGP) antibodies.
> - Primarily affects the **proximal small intestine** (duodenum and jejunum), because gluten exposure is greatest there.
> - Long-term complications: increased risk of **enteropathy-associated T-cell lymphoma (EATL)** and **small intestinal adenocarcinoma**.
#### 2. Goblet Cells
- Second most abundant cell type in the intestinal epithelium.
- **Unicellular mucous glands** that secrete **mucus** (acidic glycoproteins/mucins, mainly MUC2).
- Shape: resembles a goblet or wine glass:
- **Expanded apical portion (theca)** filled with pale-staining (or clear) mucous granules (the mucus is often washed out during H&E processing, leaving a clear space).
- **Narrow basal portion (stem)** containing the compressed, dark-staining nucleus and RER.
- The mucus forms a **protective lubricating layer** over the epithelium.
- **Distribution**: Goblet cells increase in number from the **duodenum to the ileum** (fewest in duodenum, most in ileum) and further increase in the **large intestine** (where they are the predominant cell type).
- The granules are **strongly PAS-positive** (mucins contain abundant carbohydrate).
- Goblet cells release mucus by **compound exocytosis** (simultaneously releasing the contents of multiple granules).
> **CLINICAL: Goblet Cell Metaplasia** – Presence of goblet cells where they normally should not be (e.g., esophagus in Barrett's, stomach in intestinal metaplasia) is a sign of metaplasia and potentially a precancerous change.
#### 3. Paneth Cells
- Located at the **base of the crypts of Lieberkühn** (intestinal glands).
- **Large, pyramidal cells** with:
- **Basally placed nucleus**
- **Basophilic basal cytoplasm** (abundant RER)
- **Large, brightly eosinophilic (refractile) apical secretory granules** – these are very characteristic and make Paneth cells easy to identify.
- **Contents of Paneth cell granules**:
- **Lysozyme**: an antimicrobial enzyme that cleaves bacterial cell wall peptidoglycan.
- **α-Defensins (cryptdins)**: antimicrobial peptides that form pores in bacterial membranes.
- **Secretory phospholipase A2**: antibacterial.
- **TNF-α** and other cytokines.
- **Matrix metalloproteinases**.
- **Zinc**: concentrated in the granules.
- **Function**: Innate immunity – they regulate the intestinal microbiome and protect the stem cells at the base of the crypts. They are the "guardians" of the crypt stem cell niche.
- **Long-lived cells**: unlike other intestinal epithelial cells that turn over every 3–5 days, Paneth cells live for **~20 days** and are eventually phagocytosed and replaced.
- **Distribution**: Present throughout the **small intestine**. Normally **absent** from the large intestine (their presence in the colon is a sign of **Paneth cell metaplasia**, seen in chronic inflammatory conditions like ulcerative colitis).
- Paneth cells are also present in the **appendix** (normally).
> **CLINICAL: Paneth Cell Dysfunction and Crohn's Disease** – There is emerging evidence that Paneth cell defects (e.g., mutations in **NOD2/CARD15**, **ATG16L1** – an autophagy gene) contribute to the pathogenesis of **Crohn's disease**, particularly ileal Crohn's. NOD2 is a pattern recognition receptor expressed in Paneth cells that senses muramyl dipeptide (from bacterial peptidoglycan). Mutations lead to defective innate immunity and altered microbiome, contributing to chronic inflammation.
#### 4. Enteroendocrine Cells
- Scattered throughout the epithelium of the crypts and villi.
- Belong to the **diffuse neuroendocrine system (DNES)**.
- They are the most common endocrine cells in the body (collectively).
- Usually **triangular** with **basally located secretory granules** (released into the lamina propria/capillaries – endocrine or paracrine secretion).
- Types in the small intestine include:
- **S cells** (duodenum/jejunum): secrete **secretin** → stimulates pancreatic bicarbonate secretion
- **I cells** (duodenum/jejunum): secrete **cholecystokinin (CCK)** → stimulates pancreatic enzyme secretion, gallbladder contraction, and satiety
- **K cells** (duodenum/jejunum): secrete **glucose-dependent insulinotropic peptide (GIP)** → stimulates insulin release (incretin effect)
- **L cells** (ileum/colon): secrete **glucagon-like peptide-1 (GLP-1)** and **peptide YY (PYY)** → GLP-1 is an incretin; PYY induces satiety and slows gastric emptying
- **EC cells** (throughout): secrete **serotonin (5-HT)** → stimulates gut motility
- **D cells** (throughout): secrete **somatostatin** → inhibits various GI functions
- **Mo cells** (duodenum): secrete **motilin** → stimulates migrating motor complex (MMC – "housekeeper" waves during fasting)
- **N cells** (ileum): secrete **neurotensin**
> **CLINICAL: Carcinoid Tumors (Neuroendocrine Tumors/NETs) of the Small Intestine** – Most commonly arise in the **ileum**. They are derived from enteroendocrine cells, especially EC cells. Small intestinal NETs are the most common small bowel malignancy. They can secrete **serotonin** and other vasoactive substances. If hepatic metastases are present (serotonin bypasses hepatic first-pass metabolism), patients develop **carcinoid syndrome**: episodic flushing, diarrhea, wheezing (bronchoconstriction), and right-sided heart disease (endocardial fibrosis of tricuspid and pulmonic valves). Diagnosis: elevated **urinary 5-HIAA** (5-hydroxyindoleacetic acid, a serotonin metabolite). Histologically, the tumors show nests, trabeculae, or insular patterns of uniform cells with salt-and-pepper chromatin. IHC: positive for **chromogranin A** and **synaptophysin**.
> **CLINICAL: Incretin-based Therapies** – GLP-1 receptor agonists (e.g., semaglutide, liraglutide) and DPP-4 inhibitors (e.g., sitagliptin) are used in type 2 diabetes. They enhance the incretin effect of GLP-1 secreted by L cells. GLP-1 receptor agonists also promote weight loss and are now used in obesity management.
#### 5. M Cells (Microfold Cells)
- Specialized epithelial cells overlying **Peyer's patches** and other organized lymphoid follicles in the lamina propria.
- Located in the **follicle-associated epithelium (FAE)**.
- Characteristics:
- **Flattened apical surface** with **microfolds** (rather than microvilli) – this is the origin of the name.
- **No glycocalyx or brush border enzymes**.
- **Deeply invaginated basolateral surface** that forms a pocket containing **lymphocytes** and **antigen-presenting cells (macrophages, dendritic cells)**.
- **Function**: M cells **sample luminal antigens** by **transcytosis** (endocytosis from the luminal surface, transport across the cell, and exocytosis to the basolateral pocket where immune cells are waiting). This is the primary mechanism by which the intestinal immune system "surveys" luminal antigens and microorganisms.
- They do NOT process antigens; they merely transport them.
> **CLINICAL: M Cells as Portals of Entry for Pathogens** – Certain pathogens exploit M cells for invasion:
> - *Salmonella typhi* (typhoid fever) – invades through M cells overlying Peyer's patches, especially in the **ileum**. The Peyer's patches become swollen, necrotic, and may ulcerate, with ulcers oriented along the **long axis** of the bowel. Complications include hemorrhage and perforation.
> - *Shigella* spp.
> - **Poliovirus**
> - *Yersinia enterocolitica*
> - **Prions** (bovine spongiform encephalopathy)
#### 6. Stem Cells
- Located at the **base of the crypts of Lieberkühn**, interspersed among Paneth cells.
- Two populations:
- **CBC cells (Crypt Base Columnar cells / Lgr5+ cells)**: Slender cells wedged between Paneth cells at the very base of the crypt. They express **Lgr5** (leucine-rich repeat-containing G-protein coupled receptor 5), a Wnt target gene and stem cell marker. They are actively cycling stem cells.
- **"+4 position" cells**: Located approximately 4 cell positions from the base of the crypt. May serve as reserve/quiescent stem cells (activated when CBC cells are damaged). Express markers like **Bmi1**.
- Stem cells give rise to **transit-amplifying cells** that rapidly divide and differentiate as they migrate upward along the crypt-villus axis.
- All epithelial cell types are derived from these stem cells.
- The stem cell niche is maintained by signals from surrounding Paneth cells and mesenchymal cells (Wnt, Notch, BMP, EGF pathways).
> **CLINICAL: Colorectal Carcinogenesis** – The stem cells in intestinal crypts are thought to be the **cells of origin** for colorectal adenomas and carcinomas. Mutations in the **APC gene** (adenomatous polyposis coli), a component of the Wnt signaling pathway, lead to constitutive Wnt activation and uncontrolled stem cell proliferation. APC mutation is the initiating event in the **adenoma-carcinoma sequence** (Vogelstein model): Normal epithelium → APC mutation → small adenoma → KRAS mutation → large adenoma → p53 loss/SMAD4 loss → carcinoma.
> **CLINICAL: Radiation Enteritis** – Radiation therapy targeting abdominal/pelvic tumors can damage the rapidly dividing stem cells and transit-amplifying cells in the crypts, leading to **crypt loss** (radiation-induced apoptosis), mucosal atrophy, villous blunting, and ulceration. Chronic radiation enteritis is characterized by **submucosal fibrosis**, **vascular sclerosis** (endarteritis obliterans), and mucosal atrophy.
### Intestinal Glands (Crypts of Lieberkühn)
- **Simple tubular glands** that extend from the base of the villi to the muscularis mucosae.
- They open between the bases of adjacent villi.
- The crypts are the sites of **cell proliferation** (stem cells and transit-amplifying cells) and **secretion** (Paneth cells, goblet cells, enteroendocrine cells).
- Crypt cells secrete **chloride ions** (via the **CFTR** chloride channel), and water follows osmotically → contributes to the liquid environment of the lumen.
> **CLINICAL: Cystic Fibrosis** – Mutations in the **CFTR gene** (cystic fibrosis transmembrane conductance regulator) affect the chloride channel on the apical membrane of crypt epithelial cells. In the intestine, this leads to thick, dehydrated mucus that can obstruct the intestinal lumen → **meconium ileus** (in neonates, ~15% of CF patients) – obstruction of the distal ileum by thick meconium.
> **CLINICAL: Cholera** – *Vibrio cholerae* produces **cholera toxin**, which permanently activates **adenylyl cyclase** in crypt epithelial cells (via ADP-ribosylation of the Gs protein). This leads to massive cAMP-mediated secretion of Cl⁻ (via CFTR) and water into the intestinal lumen → profuse, life-threatening **secretory diarrhea** ("rice-water stool"). The epithelium is histologically intact (no destruction), but the functional secretion is overwhelming. The volume of diarrhea can reach 15–20 liters/day, leading to death from dehydration and electrolyte imbalance.
> **CLINICAL: Crypt Abscess** – Accumulation of neutrophils within the lumen of intestinal crypts. This finding is characteristic of **inflammatory bowel disease (IBD)**, especially **ulcerative colitis**, but is not entirely specific (can be seen in infectious colitis). In UC, crypt abscesses are associated with mucosal and submucosal inflammation (the inflammation does NOT extend beyond the submucosa in UC, unlike Crohn's disease which is transmural).
### Lamina Propria of the Small Intestine
- Fills the core of each villus and surrounds the crypts.
- Contains:
- **Central lacteal** in each villus (see above)
- **Capillary network** (fenestrated capillaries)
- **Smooth muscle strands** (from muscularis mucosae)
- **Immune cells**: The small intestinal lamina propria is one of the largest immune compartments in the body.
- **IgA-producing plasma cells**: IgA is transported across the epithelium by the **polymeric immunoglobulin receptor (pIgR / secretory component)** on the basolateral surface of enterocytes. It is released into the lumen as **secretory IgA (sIgA)**, which neutralizes pathogens and toxins in the lumen without triggering inflammation. The sIgA is resistant to proteolysis because of the secretory component.
- Macrophages, dendritic cells, T cells, mast cells, eosinophils
- **GALT**:
- **Isolated lymphoid follicles** (scattered throughout)
- **Peyer's patches** (organized lymphoid aggregates, primarily in the **ileum** – on the **anti-mesenteric border**):
- These are aggregates of **lymphoid follicles** (20–40 per patch) in the lamina propria that extend into the submucosa.
- They have **germinal centers** (B cell zones) surrounded by **T cell zones** (parafollicular areas).
- The overlying epithelium is the **follicle-associated epithelium (FAE)** containing **M cells** (described above).
- Peyer's patches lack villi (the surface is dome-shaped).
- They are visible macroscopically as oval elevations on the ileal mucosa.
- They are most prominent in **young individuals** and tend to regress with age.
> **CLINICAL: Typhoid Fever and Peyer's Patches** – As mentioned, *Salmonella typhi* invades through M cells over Peyer's patches in the ileum. The patches undergo hyperplasia (week 1), necrosis (week 2), ulceration (week 3 – risk of hemorrhage and perforation), and healing (week 4). The ulcers are elongated along the longitudinal axis of the bowel (unlike TB ulcers, which are transverse/circumferential).
> **CLINICAL: Selective IgA Deficiency** – The most common primary immunodeficiency (~1:500 in Caucasians). Patients have decreased sIgA in mucosal secretions, leading to increased susceptibility to GI and respiratory infections, and an association with celiac disease, giardiasis, and autoimmune diseases. Most patients are asymptomatic due to compensatory IgM secretion.
### Muscularis Mucosae of the Small Intestine
- Two layers (inner circular, outer longitudinal).
- Sends smooth muscle extensions into the villi (villous pump).
---
## REGIONAL DIFFERENCES IN THE SMALL INTESTINE
### DUODENUM
#### Special Features:
1. **Brunner's Glands (Duodenal Submucosal Glands)**:
- The **hallmark** of the duodenum – the most distinctive histological feature.
- Located in the **submucosa** (unique – glands in the submucosa are found only in the esophagus and duodenum in the GI tract).
- **Branched, coiled, tubular mucous glands**.
- They secrete:
- **Alkaline mucus** (rich in bicarbonate, pH ~9) that neutralizes the acidic chyme entering from the stomach, protecting the duodenal mucosa from acid-peptic damage.
- **Urogastrone (epidermal growth factor, EGF)**: promotes epithelial cell proliferation and mucosal repair.
- **Pepsinogen** (weak pepsin precursor).
- The ducts penetrate through the muscularis mucosae to open into the **base of the crypts of Lieberkühn** or directly onto the surface.
- Most abundant in the **proximal duodenum** (first part) and diminish distally; they may extend slightly into the proximal jejunum.
- The glands contain **pale-staining mucous cells** with flattened basal nuclei. In H&E, they appear as pale-staining lobulated structures in the submucosa.
> **CLINICAL: Duodenal Ulcers** – Duodenal ulcers are most common in the **first part of the duodenum** (duodenal bulb), where acidic chyme first contacts the duodenal mucosa. They are strongly associated with **H. pylori** infection (present in ~95% of cases) and NSAID use. Posterior duodenal ulcers may erode into the **gastroduodenal artery**, causing massive hemorrhage. Anterior duodenal ulcers may perforate into the peritoneal cavity.
> **CLINICAL: Brunner Gland Hyperplasia/Hamartoma** – Hyperplasia of Brunner's glands can occur in the setting of peptic disease. Brunner gland hamartoma (or Brunner gland adenoma) is a rare benign polypoid lesion of the duodenum.
2. **Villi**: Broad, leaf-shaped (spatulate or tongue-shaped) – wider than jejunal/ileal villi.
3. **Goblet cells**: Fewer than in the jejunum and ileum.
4. **Enteroendocrine cells**: S cells (secretin), I cells (CCK), K cells (GIP) are concentrated here.
### JEJUNUM
#### Special Features:
1. **Plicae circulares**: Tallest and most numerous here – the jejunum is the site of maximal absorption.
2. **Villi**: Tall, finger-like (the tallest villi in the GI tract).
3. **No Brunner's glands** (submucosa contains only connective tissue, vessels, Meissner's plexus).
4. **Fewer goblet cells** than ileum.
5. **No Peyer's patches** (or very few).
### ILEUM
#### Special Features:
1. **Peyer's patches**: The **hallmark** of the ileum. Aggregated lymphoid follicles on the anti-mesenteric border.
2. **Villi**: Shorter and less numerous than in the jejunum.
3. **Plicae circulares**: Less prominent than in jejunum; absent in distal ileum.
4. **Goblet cells**: Most numerous in the small intestine (increasing gradient from duodenum to ileum).
5. **Specialized for B12 and bile salt absorption**: The terminal ileum has specific receptors for:
- **Intrinsic factor-B12 complex** (cubilin receptor)
- **Bile salt reabsorption** via the **apical sodium-dependent bile acid transporter (ASBT)** – enterohepatic circulation
> **CLINICAL: Resection of Terminal Ileum** – Surgical resection of the terminal ileum (e.g., for Crohn's disease) leads to:
> - **Vitamin B12 deficiency** → megaloblastic anemia
> - **Bile salt malabsorption** → bile salts reach the colon → stimulate colonic water secretion → **bile salt diarrhea** (cholerheic diarrhea). If the resection is extensive, bile salt pool is depleted → fat malabsorption → steatorrhea → deficiency of fat-soluble vitamins (A, D, E, K). Also increases risk of gallstones (cholesterol gallstones due to bile salt deficiency) and oxalate kidney stones (unabsorbed fatty acids bind calcium, leaving oxalate free to be absorbed).
> **CLINICAL: Meckel's Diverticulum** – A true diverticulum (all three layers of the bowel wall) resulting from incomplete obliteration of the **vitelline (omphalomesenteric) duct**. "Rule of 2s": ~2% of the population, ~2 feet from the ileocecal valve, ~2 inches long, presents by age 2, 2 types of ectopic mucosa (gastric and pancreatic). **Ectopic gastric mucosa** (containing parietal cells that secrete acid) in the diverticulum can cause **peptic ulceration** of the adjacent ileal mucosa, leading to painless GI bleeding (most common presentation in children) or perforation. Histologically, the diverticulum shows all layers of the intestinal wall (mucosa, submucosa, muscularis externa, serosa) and may contain heterotopic gastric or pancreatic tissue.
## Submucosa of the Small Intestine
- Standard features (dense irregular CT, vessels, Meissner's plexus, lymphatics).
- **Brunner's glands** in the duodenum (described above).
- Forms the core of **plicae circulares**.
## Muscularis Externa of the Small Intestine
- Standard two layers: inner circular, outer longitudinal.
- Myenteric plexus between the layers.
> **CLINICAL: Small Bowel Obstruction** – Histologically, the wall proximal to the obstruction shows dilated lumen, mucosal edema, congestion, and eventually ischemic changes if untreated (mucosal necrosis). The muscularis externa may show hypertrophy proximal to chronic partial obstruction.
## Serosa / Adventitia
- **Duodenum**: Retroperitoneal part → **adventitia**; the first part (superior) of the duodenum has serosa on its anterior surface.
- **Jejunum and Ileum**: Intraperitoneal → **serosa** (mesentery-suspended).
---
# 5. LARGE INTESTINE (COLON)
## Overview
- Includes the cecum, ascending colon, transverse colon, descending colon, sigmoid colon, and rectum.
- **Functions**: Absorption of **water and electrolytes** (especially Na⁺ and Cl⁻); synthesis and absorption of **vitamins** (vitamin K, some B vitamins by commensal bacteria); formation and storage of **feces**; secretion of **mucus** for lubrication of fecal matter.
## Key Histological Differences from Small Intestine
1. **No villi** – the mucosal surface is flat (smooth).
2. **No plicae circulares** (but there are **semilunar folds/plicae semilunares** between haustra – these involve mucosa, submucosa, and sometimes the inner circular muscle layer).
3. **No Paneth cells** (normally – their presence indicates metaplasia).
4. **No Brunner's glands**.
5. **Abundant goblet cells** – the predominant cell type in the colonic epithelium.
6. **Crypts of Lieberkühn are longer and straighter** than in the small intestine (more tubular, tightly packed, extend deeper to the muscularis mucosae).
7. **Teniae coli** – the outer longitudinal layer of the muscularis externa is concentrated into three bands.
8. **Appendices epiploicae** (peritoneal fat tags on the serosa).
## Mucosa
### Epithelium
- **Simple columnar epithelium** lining both the surface and the crypts.
- **Cell types**:
#### 1. Absorptive Cells (Colonocytes)
- Similar to enterocytes but with **shorter, less prominent microvilli** (fewer brush border enzymes needed since most digestion is complete before reaching the colon).
- Primary function: **absorption of water and electrolytes** (Na⁺ absorption via ENaC channels, stimulated by aldosterone; Cl⁻ absorption and HCO₃⁻ secretion).
- Also absorb **short-chain fatty acids (SCFAs)** – butyrate, propionate, acetate – produced by bacterial fermentation of dietary fiber. **Butyrate** is the primary energy source for colonocytes and has anti-inflammatory and anti-neoplastic properties.
> **CLINICAL: Diversion Colitis** – When a segment of colon is surgically diverted (e.g., by a proximal colostomy or ileostomy), the diverted segment no longer receives luminal contents and therefore lacks SCFAs. This leads to **mucosal inflammation** of the diverted segment (diversion colitis/proctitis). Treatment includes SCFA enemas (butyrate enemas) or restoration of bowel continuity.
> **CLINICAL: Pseudomembranous Colitis (C. difficile Colitis)** – *Clostridioides difficile* produces toxins A and B that damage colonocytes and trigger a severe inflammatory response. Histologically, the hallmark is the **"summit lesion"** or **"volcano lesion"**: an eruption of fibrin, mucus, neutrophils, and cellular debris from the surface epithelium/crypts, forming a **pseudomembrane** (yellowish-green plaques visible on colonoscopy). The pseudomembrane is an exudate that arises from focal areas of necrosis, with adjacent mucosa often relatively spared (skip lesions possible). Risk factors: antibiotic use (especially clindamycin, fluoroquinolones, cephalosporins), hospitalization, advanced age.
#### 2. Goblet Cells
- **Very abundant** – the most numerous cell type in the colonic crypt epithelium.
- Their number increases from the **cecum to the rectum**.
- They secrete abundant mucus that lubricates the feces and facilitates passage.
- The crypts of the colon appear "clear" or "pale" at low power due to the abundance of goblet cells (the mucus-filled theca appears clear in H&E).
> **CLINICAL: Mucin-Depleted Crypts** – In **ulcerative colitis**, active inflammation leads to depletion of mucin from goblet cells ("goblet cell depletion" or "mucin depletion"). This is a characteristic (but not specific) histological finding of active UC.
#### 3. Enteroendocrine Cells
- Present but less numerous than in the small intestine.
- **L cells** (secrete GLP-1 and PYY) are present in the colon.
- **EC cells** (secrete serotonin) are present.
#### 4. Stem Cells
- Located at the **base of the colonic crypts** (similar to the small intestine; Lgr5+ CBC cells).
- No Paneth cells to maintain the niche; instead, **deep crypt secretory cells (DCS cells)** and surrounding mesenchymal cells provide niche signals.
#### 5. M Cells
- Found overlying isolated lymphoid follicles in the colon.
### Crypts of Lieberkühn (Colonic Glands)
- **Long, straight, tubular glands** that extend from the surface to the muscularis mucosae.
- Very closely packed with minimal intervening lamina propria.
- Predominantly composed of goblet cells, with some absorptive cells and enteroendocrine cells.
- **No Paneth cells normally** (their presence is **Paneth cell metaplasia**, a sign of chronic mucosal injury, seen in IBD, especially chronic UC).
> **CLINICAL: Aberrant Crypt Foci (ACF)** – These are the earliest morphological lesions in the adenoma-carcinoma sequence. They are slightly enlarged, raised crypts that can be identified by magnification chromoendoscopy. Histologically, they may show hyperplasia or dysplasia. Some harbor APC or KRAS mutations.
### Lamina Propria
- Similar to the small intestine but without villi.
- Rich in immune cells, lymphoid follicles, capillaries, lymphatics.
- **Isolated lymphoid follicles** are common throughout the colon.
- **No lacteals** (no villi → no lacteals).
### Muscularis Mucosae
- Two layers (inner circular, outer longitudinal).
- Important landmark in cancer staging (see earlier discussion).
## Submucosa
- Standard features: dense irregular connective tissue, submucosal vascular plexus, Meissner's plexus, lymphatics.
- **No glands**.
- **Submucosal lipomatosis** – fat deposition in the submucosa, especially in the right colon, can occur normally or in obesity. Submucosal lipomas are the second most common benign tumors of the colon.
## Muscularis Externa
- **Inner circular layer**: Complete, continuous layer of smooth muscle.
- **Outer longitudinal layer**: NOT continuous; it is concentrated into **three longitudinal bands** called **teniae coli** (taenia libera, taenia mesocolica, taenia omentalis).
- Between the teniae, the outer longitudinal muscle layer is very thin or nearly absent.
- The teniae are shorter than the overall length of the colon, causing the colon wall to pucker → **haustra (haustrations)** – the characteristic sacculations of the colon.
- At the **rectosigmoid junction**, the teniae spread out and fuse to form a **complete** outer longitudinal layer around the **rectum**.
- In the **appendix**, the outer longitudinal layer is also **complete** (not in bands).
- **Myenteric (Auerbach's) plexus** lies between the inner circular and outer longitudinal layers (including the teniae).
> **CLINICAL: Diverticular Disease**
> - **Diverticulosis**: Outpouching of the mucosa and submucosa through weak points in the colonic wall – specifically at the sites where the **vasa recta (blood vessels)** penetrate the muscularis externa (between the mesenteric and anti-mesenteric teniae). These are **false (pulsion) diverticula** (they do NOT contain the muscularis externa in their wall – only mucosa, submucosa, and serosa). They are most common in the **sigmoid colon** (high intraluminal pressure due to small caliber – Laplace's law). Risk factors: low-fiber diet, advancing age, obesity.
> - **Diverticulitis**: Inflammation/perforation of a diverticulum, often due to inspissated fecal material (fecalith). Can cause pericolic abscess, fistula formation, perforation, obstruction.
> - **Diverticular bleeding**: Erosion of the vasa recta at the neck or dome of the diverticulum causes painless, massive hematochezia. Diverticular disease is the most common cause of significant lower GI bleeding in the elderly.
> - Histologically, the diverticulum shows the mucosa bulging through a gap in the muscularis externa, with the wall composed of only mucosa, submucosa (thinned), and serosa. The muscularis propria shows **thickening** in the affected segment (elastosis of the teniae and thickening of the circular muscle, though the overall total smooth muscle mass is normal – it is corrugated/compacted rather than hypertrophied).
> **CLINICAL: Hirschsprung's Disease (Revisited)** – In the colon, the diagnosis requires demonstration of absent ganglion cells in the myenteric AND submucosal plexuses. The transition zone (between aganglionic distal segment and normal proximal segment) shows **hypoganglionosis**. The aganglionic segment cannot relax → functional obstruction. The proximal normally innervated colon dilates (megacolon). Calretinin immunostaining of the rectal mucosa is used as an adjunct: normal tissue shows calretinin-positive nerve fibers in the lamina propria; in Hirschsprung's disease, these fibers are absent.
> **CLINICAL: Toxic Megacolon** – A life-threatening complication of ulcerative colitis (or C. difficile colitis, Crohn's colitis). The colon becomes massively dilated (>6 cm for the transverse colon on X-ray), with transmural inflammation causing necrosis of the muscularis externa and nerve plexuses. Risk of perforation and sepsis. Histologically, there is transmural necrosis/inflammation with loss of neural plexus elements.
## Serosa / Adventitia
- **Intraperitoneal segments** (cecum, transverse colon, sigmoid colon): **serosa** (with **appendices epiploicae** – fat-filled peritoneal tags hanging from the serosa).
- **Retroperitoneal segments** (ascending colon, descending colon): **adventitia** on the posterior surface; serosa on the anterior/lateral surfaces.
- **Rectum**: Upper third has serosa anteriorly and laterally; middle third has serosa only anteriorly; lower third has no serosa → adventitia.
---
## APPENDIX (VERMIFORM APPENDIX)
Although technically part of the cecum, the appendix has distinctive histological features:
- **Mucosa**: Similar to colon – crypts of Lieberkühn (with goblet cells, absorptive cells, enteroendocrine cells). **Paneth cells are normally present** in the appendix (unlike the rest of the colon).
- **Lamina propria and submucosa**: Rich in **lymphoid tissue** – often the entire cross-section shows large lymphoid follicles with prominent germinal centers. The appendix is sometimes called the "abdominal tonsil" due to its abundant GALT. The lymphoid tissue is most prominent in **childhood and adolescence** and regresses with age (fibrous obliteration of the lumen in older adults).
- The **lumen** is small, irregular, and often partially obliterated by lymphoid tissue.
- **Muscularis externa**: Two complete layers (the outer longitudinal layer is complete, not in teniae).
- **Serosa**: Complete (the appendix has its own mesentery – the mesoappendix).
> **CLINICAL: Appendicitis** – The most common surgical emergency of the abdomen. Usually caused by luminal obstruction (by fecalith, lymphoid hyperplasia, parasites, or rarely, tumors). Obstruction → increased intraluminal pressure → ischemia → bacterial invasion. Histologically:
> - **Early (acute focal appendicitis)**: Neutrophilic infiltration of the mucosa and submucosa, with mucosal ulceration.
> - **Acute suppurative appendicitis**: Neutrophilic infiltration extends through the full thickness of the wall (transmural). Fibrinopurulent serosal exudate.
> - **Gangrenous appendicitis**: Necrosis of the wall, hemorrhage, thrombosis of vessels.
> - **Perforated appendicitis**: Full-thickness necrosis with perforation → peritonitis, periappendiceal abscess.
> - The **single most important histological criterion** for the diagnosis of acute appendicitis is **neutrophilic infiltration of the muscularis externa** (muscularis propria).
> **CLINICAL: Tumors of the Appendix**:
> - **Appendiceal neuroendocrine tumor (carcinoid)**: The most common tumor of the appendix. Usually found incidentally at the tip. Most are <2 cm and benign. Histologically, nests of uniform neuroendocrine cells.
> - **Mucinous neoplasms**: Low-grade appendiceal mucinous neoplasm (LAMN) can rupture and cause **pseudomyxoma peritonei** (accumulation of mucinous/gelatinous material in the peritoneal cavity from ruptured mucinous tumors). Histologically, the appendiceal wall is replaced by mucinous epithelium (goblet cell-like cells) with abundant extracellular mucin.
> - **Goblet cell adenocarcinoma (goblet cell carcinoid)**: A unique tumor with features of both adenocarcinoma and neuroendocrine tumor.
---
# 6. RECTUM AND ANAL CANAL
## RECTUM
- Histologically similar to the **colon**, but with the following differences:
- **No teniae coli** – the outer longitudinal muscle layer is **complete** (continuous).
- **No haustra**.
- **No appendices epiploicae**.
- **Transverse rectal folds (valves of Houston)** are permanent folds involving mucosa, submucosa, and the inner circular muscle layer.
- The crypts are slightly longer than in the colon.
## ANAL CANAL
The anal canal (~3–4 cm long) is the terminal portion of the GI tract and shows a complex histological transition from the rectal mucosa to the perianal skin.
### Zones (from proximal to distal):
#### 1. Colorectal Zone (Upper Anal Canal)
- Above the **pectinate (dentate) line**.
- Lined by **simple columnar epithelium** (identical to rectum).
- Contains **anal columns of Morgagni** – longitudinal folds of mucosa containing branches of the **superior rectal artery and vein**.
- Between the columns are **anal sinuses (crypts of Morgagni)** – at the base of these sinuses are the **anal valves** (semilunar folds connecting adjacent columns).
- **Anal glands (glands of Hermann and Desfosses)**: Tubular glands that originate at the level of the pectinate line and extend into the submucosa, internal sphincter, or even into the intersphincteric space. They secrete mucus. Their ducts open into the **anal sinuses/crypts**.
> **CLINICAL: Perianal Abscess and Fistula-in-Ano** – Infection of the anal glands (cryptoglandular infection) is the most common cause of perianal abscess. The infection tracks along tissue planes. If the abscess drains spontaneously or is drained surgically, a **fistula** (abnormal tract connecting the anal canal to the perianal skin) may persist. In Crohn's disease, perianal fistulae are common due to transmural inflammation and may be complex.
#### 2. Anal Transitional Zone (ATZ)
- A narrow zone (6–12 mm) at and just above the pectinate line.
- Shows a **transitional epithelium** (not true urothelium, but a stratified epithelium that is intermediate between columnar and squamous) – often described as a **stratified columnar** or **stratified cuboidal** epithelium with features of both. It may also have patches of columnar or squamous epithelium.
- This is a zone of **epithelial transition** (similar to the transformation zone of the cervix).
#### 3. Squamous Zone (Pecten)
- Below the pectinate line.
- Lined by **stratified squamous non-keratinized epithelium** (initially, in the pecten/anoderm).
- **No hair follicles, sweat glands, or sebaceous glands** (modified skin – anoderm).
- The pecten is smooth and pale.
- Below the **intersphincteric groove (white line of Hilton)** (or approximately at the anal verge), the epithelium transitions to **keratinized stratified squamous epithelium** (true perianal skin) with **hair follicles, sebaceous glands, sweat glands (apocrine – circumanal glands), and melanocytes**.
> **CLINICAL: The Pectinate (Dentate) Line – Clinical Significance**
> This is an extremely important anatomical/histological landmark with profound clinical implications:
>
> | Feature | Above Pectinate Line | Below Pectinate Line |
> |---|---|---|
> | **Epithelium** | Simple columnar (or transitional) | Stratified squamous |
> | **Arterial supply** | Superior rectal artery (from IMA) | Inferior rectal artery (from internal pudendal) |
> | **Venous drainage** | Superior rectal vein → portal system | Inferior rectal vein → systemic (caval) system |
> | **Lymphatic drainage** | Internal iliac nodes | Superficial inguinal nodes |
> | **Nerve supply** | Autonomic (visceral) – insensitive to pain | Somatic (inferior rectal nerve) – very sensitive to pain |
> | **Hemorrhoids** | Internal hemorrhoids (not painful unless complicated) | External hemorrhoids (painful) |
> | **Cancer type** | Adenocarcinoma | Squamous cell carcinoma |
> **CLINICAL: Hemorrhoids**
> - **Internal hemorrhoids**: Dilated veins of the **internal rectal (hemorrhoidal) venous plexus** in the **submucosa** above the pectinate line, covered by columnar epithelium. They are painless (visceral innervation) but can cause **bright red painless rectal bleeding** and **prolapse**. They occur in three primary positions: left lateral (3 o'clock), right anterior (11 o'clock), and right posterior (7 o'clock) – corresponding to the branches of the superior rectal artery.
> - **External hemorrhoids**: Dilated veins of the **external rectal venous plexus** in the **subcutaneous tissue** below the pectinate line, covered by squamous epithelium. They are **painful** (somatic innervation). **Thrombosed external hemorrhoids** present as acutely painful, bluish-purple perianal lumps.
> **CLINICAL: Anal Squamous Cell Carcinoma** – Arises from the squamous epithelium of the anal canal (below the pectinate line or in the transitional zone). Strongly associated with **HPV infection** (types 16 and 18). Risk factors: receptive anal intercourse, HIV infection, immunosuppression, smoking. Histologically, shows malignant squamous cells. Treatment is primarily chemoradiation (Nigro protocol), NOT surgery (abdominoperineal resection is reserved for salvage).
> **CLINICAL: Anal Melanoma** – Rare but aggressive. Arises from melanocytes in the anal mucosa/skin. Often amelanotic (non-pigmented), leading to delayed diagnosis.
### Sphincters
#### Internal Anal Sphincter
- A thickening of the **inner circular smooth muscle** layer of the muscularis externa.
- **Involuntary** control (autonomic innervation).
- Maintains tonic contraction to prevent fecal incontinence.
#### External Anal Sphincter
- **Skeletal muscle** (striated, voluntary).
- **Not part of the GI wall** per se; it surrounds the anal canal externally.
- Innervated by the **inferior rectal branch of the pudendal nerve (S2-S4)** – somatic motor.
- Under voluntary control.
> **CLINICAL: Fecal Incontinence** – Can result from damage to either sphincter. Obstetric injury (vaginal delivery) is the most common cause in women. Injury to the pudendal nerve or surgical damage (from fistula surgery, hemorrhoidectomy) can also cause incontinence. Endoanal ultrasound can assess sphincter integrity.
---
# 7. ENTERIC NERVOUS SYSTEM (ENS) – COMPREHENSIVE REVIEW
The ENS is sometimes called the **"second brain"** or **"brain of the gut"**. It is the most complex division of the peripheral nervous system and can function **independently** of the CNS (although it normally communicates with the CNS via the vagus nerve and pelvic splanchnic nerves).
## Structure
- Contains approximately **100 million neurons** (roughly the same number as in the spinal cord).
- Organized into two major ganglionated plexuses:
### 1. Myenteric (Auerbach's) Plexus
- Located between the inner circular and outer longitudinal layers of the muscularis externa.
- **Continuous** from esophagus to internal anal sphincter.
- Primarily controls **GI motility** (peristalsis, segmentation, sphincter tone).
- Contains motor neurons, interneurons, and sensory neurons.
- Neurotransmitters include: **ACh** (excitatory, promotes contraction), **VIP** and **NO** (inhibitory, promote relaxation), **substance P**, **serotonin**.
### 2. Submucosal (Meissner's) Plexus
- Located in the submucosa.
- Primarily found in the **small and large intestine** (sparse in the esophagus and stomach).
- Primarily regulates **mucosal secretion**, **absorption**, and **local blood flow**.
## Interstitial Cells of Cajal (ICC)
- **Non-neuronal pacemaker cells** associated with the myenteric plexus and muscularis externa.
- They generate **slow wave potentials** (rhythmic electrical oscillations) that determine the **basic electrical rhythm (BER)** of the GI tract:
- **Stomach**: ~3 waves/min
- **Duodenum**: ~12 waves/min
- **Ileum**: ~8 waves/min
- **Colon**: ~2–6 waves/min (variable)
- ICC are identified by **c-KIT (CD117)** immunostaining.
- They form a network that coordinates smooth muscle contraction.
> **CLINICAL: GISTs** – (Reiterated) Arise from ICC or their precursors. Most common mesenchymal tumor of the GI tract. c-KIT mutations (exon 11 most common) or PDGFRA mutations. Targeted therapy with imatinib revolutionized treatment.
> **CLINICAL: Chronic Intestinal Pseudo-Obstruction (CIPO)** – A rare condition characterized by signs and symptoms of intestinal obstruction without any mechanical cause. Can be due to:
> - **Neuropathic**: damage to the enteric neurons (ENS disorders)
> - **Myopathic**: damage to the smooth muscle of the muscularis externa
> - **ICC-opathic**: loss of ICC
> Histologically, the muscularis externa and/or nerve plexuses may show degenerative changes, fibrosis, or inflammatory infiltration. Requires full-thickness biopsy for diagnosis (not mucosal biopsy).
---
# 8. GALT (GUT-ASSOCIATED LYMPHOID TISSUE) – COMPREHENSIVE REVIEW
The GI tract is the largest immunological organ in the body, constantly exposed to dietary antigens, commensal microbes, and pathogens.
## Components of GALT:
### 1. Intraepithelial Lymphocytes (IELs)
- Located between epithelial cells, above the basement membrane.
- Predominantly **CD8+ T cells** (cytotoxic T cells).
- Most express the **γδ T-cell receptor** (in the small intestine; αβ T cells also present).
- Function: first line of immune defense; recognize stressed or infected epithelial cells.
- **Normal count**: <25 IELs per 100 epithelial cells in the small intestine.
- **Increased IELs**: celiac disease (>25/100), tropical sprue, drug-associated enteropathy, autoimmune enteropathy, graft-versus-host disease.
### 2. Lamina Propria Lymphocytes
- A mixed population: CD4+ T cells (helper), CD8+ T cells, plasma cells (especially **IgA-secreting**), macrophages, dendritic cells, mast cells, eosinophils.
- **Plasma cells** produce mainly **IgA** (dimeric), which is transported across the epithelium by pIgR to become secretory IgA (sIgA).
### 3. Lymphoid Follicles/Nodules
- **Isolated (solitary) lymphoid follicles**: found throughout the GI tract, from esophagus to rectum. They are in the lamina propria and may extend into the submucosa.
- **Peyer's patches**: aggregated lymphoid follicles in the ileum (20–30 follicles per patch; ~30–40 patches in the ileum). Covered by M cell-containing FAE.
- **Cryptopatches**: clusters of lymphocyte precursors at crypt bases (in the small intestine and colon) – their role is being elucidated; they may give rise to IELs.
### 4. Mesenteric Lymph Nodes
- Not technically in the GI wall but drain lymph from the intestinal tract and are part of the mucosal immune system.
> **CLINICAL: MALT Lymphoma (Mucosa-Associated Lymphoid Tissue Lymphoma)** – An extranodal marginal zone B-cell lymphoma. Most commonly occurs in the **stomach** (gastric MALT lymphoma), associated with chronic **H. pylori** infection. The chronic antigenic stimulation by H. pylori leads to reactive lymphoid proliferation → monoclonal B cell expansion → lymphoma. Characterized by **lymphoepithelial lesions** (clusters of neoplastic lymphocytes infiltrating and destroying glandular epithelium). In early stages, eradication of H. pylori can lead to **complete regression** of the lymphoma (demonstrating its antigen dependence). T(11;18) translocation is associated with resistance to H. pylori eradication therapy.
> **CLINICAL: Whipple's Disease** – Caused by the bacterium *Tropheryma whipplei*. The lamina propria of the small intestine is packed with **foamy macrophages** filled with bacteria. The macrophages are **PAS-positive and diastase-resistant** (the bacterial cell wall glycoprotein stains with PAS). On electron microscopy, the bacteria are rod-shaped. Clinical features: diarrhea, weight loss, arthralgia, lymphadenopathy, cardiac and CNS involvement. This represents a failure of macrophage bactericidal function.
---
# 9. COMPARATIVE HISTOLOGY TABLE
| Feature | Esophagus | Stomach | Small Intestine | Large Intestine |
|---|---|---|---|---|
| **Epithelium** | Stratified squamous (non-keratinized) | Simple columnar (surface mucous cells) | Simple columnar (enterocytes, goblet cells) | Simple columnar (colonocytes, abundant goblet cells) |
| **Villi** | Absent | Absent | Present (finger/leaf-like) | Absent |
| **Glands in mucosa** | Cardiac glands (near GEJ) | Gastric glands (fundic, pyloric, cardiac) | Crypts of Lieberkühn | Crypts of Lieberkühn (longer, straighter) |
| **Paneth cells** | Absent | Absent | Present (base of crypts) | Absent (normally) |
| **Submucosal glands** | Esophageal glands proper | Absent | Brunner's glands (duodenum only) | Absent |
| **Muscularis externa** | Skeletal (upper) → smooth (lower); 2 layers | 3 layers (oblique, circular, longitudinal) | 2 layers (circular, longitudinal) | 2 layers (circular, longitudinal – outer in teniae coli) |
| **Outer covering** | Adventitia (mostly) | Serosa | Serosa (jejunum/ileum); Adventitia (retroperitoneal duodenum) | Serosa or Adventitia (varies) |
| **Special features** | Submucosal glands, skeletal muscle | Rugae, gastric pits, parietal/chief cells | Villi, plicae circulares, Brunner's glands, Peyer's patches | Teniae coli, haustra, appendices epiploicae |
---
# 10. ADDITIONAL CLINICAL CORRELATIONS
> **CLINICAL: Inflammatory Bowel Disease (IBD) – Histological Comparison**
>
> | Feature | Crohn's Disease | Ulcerative Colitis |
> |---|---|---|
> | **Distribution** | Any part of GI tract (mouth to anus); most common in terminal ileum and colon | Colon only (starts at rectum, extends proximally) |
> | **Pattern** | Skip lesions (discontinuous) | Continuous (no skip lesions) |
> | **Depth of inflammation** | **Transmural** (involves all layers) | **Mucosal and submucosal** (does not extend beyond submucosa, unless toxic megacolon) |
> | **Granulomas** | **Non-caseating granulomas** (present in ~50%; not always found but highly characteristic) | Absent (crypt abscesses and pseudopolyps, but no granulomas) |
> | **Crypt abscesses** | Uncommon | **Characteristic** |
> | **Goblet cell depletion** | Less prominent | **Characteristic** |
> | **Fissures/fistulae** | **Characteristic** (due to transmural inflammation; knife-like fissures, fistulae to skin, bladder, other bowel loops) | Rare (unless toxic megacolon) |
> | **Ulcers** | Deep, linear ("railroad track" ulcers), aphthous ulcers | Superficial, broad-based, undermining |
> | **Cobblestone mucosa** | Present (islands of edematous mucosa between linear ulcers) | Absent |
> | **Pseudopolyps** | Uncommon | **Characteristic** (inflammatory polyps – islands of regenerating mucosa surrounded by ulcerated areas) |
> | **Fibrosis/strictures** | Common (due to transmural fibrosis → bowel obstruction) | Uncommon |
> | **Fat wrapping (creeping fat)** | Characteristic (mesenteric fat wraps around the bowel wall) | Absent |
> | **Cancer risk** | Increased (but less than UC; risk in colonic Crohn's) | **Significantly increased** risk of colorectal carcinoma (risk increases with duration and extent of disease; requires surveillance colonoscopy) |
> | **Dysplasia** | Can occur | Flat dysplasia (DALM – dysplasia-associated lesion or mass) is a major concern for malignancy |
> **CLINICAL: Colorectal Carcinoma – Histopathological Staging (TNM)**
> - **Tis**: Carcinoma in situ / intramucosal carcinoma (does not penetrate muscularis mucosae)
> - **T1**: Invades submucosa
> - **T2**: Invades muscularis propria (muscularis externa)
> - **T3**: Invades through muscularis propria into subserosa/pericolorectal tissue
> - **T4a**: Penetrates visceral peritoneum (serosa)
> - **T4b**: Directly invades other organs/structures
> - **Dukes Classification (historical)**: A (confined to wall) → B (through wall) → C (lymph node involvement) → D (distant metastasis)
> **CLINICAL: Familial Adenomatous Polyposis (FAP)** – Autosomal dominant condition caused by mutations in the **APC gene** (chromosome 5q21). Patients develop hundreds to thousands of adenomatous polyps in the colon (and sometimes upper GI tract). Without prophylactic colectomy, nearly 100% progress to colorectal carcinoma by age 40–50. Histologically, the polyps are tubular, villous, or tubulovillous adenomas with varying degrees of dysplasia. Each polyp represents a clone with "second hit" loss of the remaining APC allele.
> **CLINICAL: Lynch Syndrome (Hereditary Nonpolyposis Colorectal Cancer – HNPCC)** – Autosomal dominant condition caused by mutations in **DNA mismatch repair (MMR) genes** (MLH1, MSH2, MSH6, PMS2). Leads to **microsatellite instability (MSI-high)** tumors. Colorectal carcinomas tend to occur in the **right (proximal) colon** and at a younger age. The tumors often show a **mucinous or signet ring cell** morphology and prominent **tumor-infiltrating lymphocytes**. Also increased risk of endometrial, ovarian, gastric, urinary tract, and other cancers.
> **CLINICAL: Peutz-Jeghers Syndrome** – Autosomal dominant; mutation in **STK11/LKB1** gene. **Hamartomatous polyps** throughout the GI tract (most common in the small intestine). The polyps have a characteristic histological appearance: arborizing smooth muscle bundles (from muscularis mucosae) extending into the polyp ("Christmas tree" pattern), covered by normal-appearing mucosa. Associated with mucocutaneous melanin pigmentation (lips, buccal mucosa, palms). Increased risk of GI and extra-GI malignancies (breast, ovary, pancreas, lung).
> **CLINICAL: Juvenile Polyps** – Hamartomatous polyps most common in children. Histologically, they show **dilated, mucus-filled cystic glands** (cystically dilated crypts) in an expanded, edematous, inflamed lamina propria with smooth muscle strands. The surface is often eroded. Juvenile polyposis syndrome (multiple polyps, autosomal dominant – SMAD4 or BMPR1A mutations) carries a risk of colorectal carcinoma.
> **CLINICAL: Ischemic Colitis** – Most commonly affects the **splenic flexure** (watershed area between SMA and IMA territories) and the **rectosigmoid** (watershed between IMA and internal iliac). Histologically: **mucosal necrosis** ("ghost" outlines of crypts with loss of nuclear staining), hemorrhage into the lamina propria, submucosal edema, **hemosiderin-laden macrophages** (in chronic/healing ischemia), and eventually fibrosis. The pattern of damage is "top-down" (mucosal surface affected first, then deeper layers).
> **CLINICAL: Microscopic Colitis** – Two subtypes with normal colonoscopic appearance (hence "microscopic" – diagnosis requires biopsy):
> 1. **Collagenous colitis**: Thickened subepithelial **collagen band** (>10 μm; normal ≤5 μm) beneath the surface epithelium, with chronic inflammatory infiltrate in the lamina propria and damage to surface epithelium.
> 2. **Lymphocytic colitis**: Increased **intraepithelial lymphocytes** (>20 IELs per 100 surface epithelial cells) with chronic inflammation in the lamina propria but NO thickened collagen band.
> Both present with chronic watery diarrhea, often in middle-aged to elderly women. Associated with autoimmune disorders and certain medications (NSAIDs, PPIs, SSRIs).
---
# 11. SPECIALIZED CELLS AND STRUCTURES – ADDITIONAL DETAILS
## Brush (Tuft / Caveolated) Cells
- Scattered among the epithelial cells throughout the GI tract (from stomach to colon, but most prominent in the small intestine).
- **Flask-shaped cells** with a **prominent tuft of long, thick microvilli** (longer than those of enterocytes) on their apical surface.
- Express taste receptors (T1R and T2R families) and **gustducin** (a G-protein also found in taste buds).
- They are **chemosensory cells** – they sense luminal contents (possibly parasites, bacterial products).
- When activated (e.g., by parasites), they secrete **IL-25** and **IL-33**, which initiate a **type 2 immune response** (involving ILC2 cells, Th2 cells) leading to goblet cell hyperplasia, mucus secretion, and smooth muscle contraction – helping to expel parasites.
- They play a role in initiating innate immune responses to helminthic infections.
## Cup Cells
- Found primarily in the small intestine (especially jejunum).
- Characterized by a **cup-shaped** or concave apical surface with shorter microvilli.
- Function is not fully understood; may have absorptive or chemosensory roles.
## Intestinal Glial Cells (Enteric Glial Cells)
- The "astrocytes" of the ENS.
- Express **GFAP (glial fibrillary acidic protein)** and **S100 protein**.
- They support enteric neurons, regulate intestinal barrier function, and participate in neuroimmune interactions.
- Damage to enteric glia may contribute to intestinal inflammation and barrier dysfunction.
---
# 12. RENEWAL AND REPAIR OF THE GI EPITHELIUM
The GI epithelium is one of the most rapidly renewing tissues in the body:
- **Stem cells** in the crypts (Lgr5+ cells) continuously divide.
- **Transit-amplifying cells** undergo rapid mitotic divisions as they migrate upward from the crypt.
- **Differentiation** occurs as cells migrate:
- **Upward migration**: absorptive cells, goblet cells → reach the villus tip (small intestine) or surface (colon) where they undergo **apoptosis and are shed** into the lumen (anoikis – detachment-induced apoptosis).
- **Downward migration**: Paneth cells (migrate to the base) and some enteroendocrine cells.
- **Turnover time**: ~3–5 days for enterocytes/colonocytes; ~20 days for Paneth cells; variable for enteroendocrine cells.
- **Wnt signaling** (from Paneth cells and mesenchymal cells) maintains stem cell self-renewal in the crypt.
- **Notch signaling** determines absorptive vs. secretory fate (Notch activation → absorptive cell; Notch inhibition → secretory cells: goblet, Paneth, enteroendocrine).
- **BMP signaling** (from mesenchymal cells in the villus) promotes differentiation and counteracts Wnt.
> **CLINICAL: Chemotherapy-Induced Mucositis** – Many chemotherapeutic agents (5-fluorouracil, methotrexate, irinotecan) target rapidly dividing cells. Since the GI epithelium turns over so rapidly, it is highly susceptible. Damage to crypt stem cells and transit-amplifying cells leads to **mucositis** – inflammation and ulceration of the GI mucosa (oral mucositis, esophagitis, enteritis, colitis). This causes pain, diarrhea, malabsorption, and risk of infection/sepsis (loss of mucosal barrier). Recovery depends on surviving stem cells repopulating the crypts.
> **CLINICAL: Graft-Versus-Host Disease (GVHD)** – After allogeneic bone marrow transplant, donor T cells can attack host tissues, including the GI tract. **Intestinal GVHD** characteristically shows **apoptosis of crypt epithelial cells** ("apoptotic bodies" or "exploding crypts"), with eventual crypt loss and mucosal denudation. The apoptotic bodies in crypts (individual cell necrosis) are a hallmark histological finding.
---
# SUMMARY OF KEY HISTOLOGICAL LANDMARKS FOR IDENTIFICATION
| Structure/Feature | Identifies... |
|---|---|
| **Stratified squamous epithelium + submucosal glands** | **Esophagus** |
| **Surface mucous cells + gastric pits + parietal cells (eosinophilic)** | **Stomach (fundus/body)** |
| **Deep gastric pits + mucous glands + G cells** | **Stomach (pylorus)** |
| **Villi + crypts + Brunner's glands in submucosa** | **Duodenum** |
| **Tall villi + prominent plicae circulares + no Brunner's glands + no Peyer's patches** | **Jejunum** |
| **Shorter villi + Peyer's patches + many goblet cells** | **Ileum** |
| **No villi + abundant goblet cells + teniae coli + long crypts** | **Colon** |
| **Dense lymphoid tissue + complete longitudinal muscle** | **Appendix** |
| **Transition from columnar → squamous epithelium + sphincters** | **Anal canal** |
---
This comprehensive review covers the histology of the entire digestive tract from esophagus to anal canal, including all four layers, all cell types with their ultrastructure and functions, regional variations, and the relevant clinical conditions. Every histological feature has been connected to its clinical significance where applicable.
Rewrite the whole content as it is plus add maximum number of high yield images along the content