I don't know how to read ECG teach me and also list out and explain common ECG abnormalities with image and disease name
Reading File
Finding Sources
Finding Sources
Searching the Web
ECG reading guide common abnormalities with images
Finding Sources
Finding Sources
Reading Web Page
https://geekymedics.com/how-to-read-an-ecg
Reading File
Reading File
Loading Image
Finding Sources
Loading Image
Loading Image
Reading File
Searching the Web
ECG waveform diagram labeled P wave QRS T wave normal sinus rhythm image
Loading Image
Searching the Web
ECG 12 lead placement chest leads anatomy diagram image
Finding Sources
Loading Image
Loading Image
Reading File
Loading Image
Reading File
Loading Image
Loading Image
I now have comprehensive material to write a complete, well-illustrated ECG guide. Let me compile it.
How to Read an ECG - Complete Guide
An ECG (electrocardiogram) records the heart's electrical activity through electrodes placed on the skin. It is one of the most useful and widely used tests in medicine. Here is a full, structured guide from basics to common abnormalities.
Part 1 - Understanding the ECG Paper
ECG paper has a standardized grid:
- Small box = 1 mm wide = 0.04 seconds horizontally, 0.1 mV vertically
- Large box = 5 mm wide = 0.2 seconds horizontally, 0.5 mV vertically
- Standard paper speed = 25 mm/second
- Standard calibration = 10 mm = 1 mV (the calibration box appears at the start of a strip)
Part 2 - The ECG Leads
A standard 12-lead ECG uses 10 electrodes to generate 12 "views" of the heart.
Lead Placement

Chest (Precordial) Leads:
| Lead | Position |
|---|---|
| V1 | 4th intercostal space, RIGHT of sternum |
| V2 | 4th intercostal space, LEFT of sternum |
| V3 | Between V2 and V4 |
| V4 | 5th intercostal space, midclavicular line |
| V5 | Between V4 and V6 |
| V6 | Horizontal to V4, midaxillary line |
Limb Leads:
- RA = right arm/wrist, LA = left arm/wrist, LL = left leg/ankle, RL = right leg (ground)
- Generate leads I, II, III (bipolar) and aVR, aVL, aVF (augmented unipolar)
What Each Lead "Sees"
| Territory | Leads |
|---|---|
| Inferior wall | II, III, aVF |
| Lateral wall | I, aVL, V5, V6 |
| Anterior wall | V1-V4 |
| Right ventricle | V1, aVR (+ right-sided leads) |
| Posterior wall | Reciprocal changes in V1-V2 |
Part 3 - The Normal ECG Waveform
Every heartbeat produces a characteristic sequence of deflections:
R
|
P | T
/\ | /\
--/ \--|--S--/ \--U--
Q
The Waves, Intervals and Segments
| Component | What it represents | Normal values |
|---|---|---|
| P wave | Atrial depolarization (SA node fires, atria contract) | <120 ms wide, <2.5 mm tall, upright in I and II |
| PR interval | Time from atrial depolarization to ventricular activation (through AV node) | 120-200 ms (3-5 small boxes) |
| QRS complex | Ventricular depolarization | <120 ms (3 small boxes) |
| ST segment | Early ventricular repolarization (isoelectric = flat) | Isoelectric (no elevation or depression) |
| T wave | Ventricular repolarization | Upright in most leads except aVR and V1 |
| QT interval | Total ventricular depolarization + repolarization | QTc < 440 ms (men), <460 ms (women) |
| U wave | Slow repolarization of His-Purkinje (not always seen) | Small, same direction as T wave |
Part 4 - The Systematic 7-Step Approach
Always analyze every ECG in the same order. Missing one step is how diagnoses get missed.
Step 1 - Rate
Quick method: Count large boxes between two R waves.
- 1 box = 300 bpm
- 2 boxes = 150 bpm
- 3 boxes = 100 bpm
- 4 boxes = 75 bpm
- 5 boxes = 60 bpm
- 6 boxes = 50 bpm
For irregular rhythms: Count QRS complexes in a 10-second strip, then multiply by 6.
Normal resting rate = 60-100 bpm. >100 = tachycardia. <60 = bradycardia.
Step 2 - Rhythm
Ask:
- Is the rhythm regular (R-R intervals equal) or irregular?
- Is there a P wave before every QRS?
- Is there a QRS after every P wave?
- Are the P waves upright in lead II (normal sinus origin)?
Normal sinus rhythm = regular, P before every QRS, P upright in II, rate 60-100.
Step 3 - Axis
The mean QRS axis tells you the dominant direction of ventricular depolarization.
Look at leads I and aVF:
| Lead I | aVF | Axis |
|---|---|---|
| Positive (up) | Positive (up) | Normal (-30° to +90°) |
| Positive (up) | Negative (down) | Left axis deviation |
| Negative (down) | Positive (up) | Right axis deviation |
| Negative (down) | Negative (down) | Extreme (northwest) axis |
Step 4 - P Waves
- Present? Upright in I and II? Rounded? One P per QRS?
- Wide (>120 ms) or notched = left atrial enlargement
- Tall peaked (>2.5 mm in lead II) = right atrial enlargement
- Absent + irregular rhythm = think atrial fibrillation
Step 5 - PR Interval
- Short (<120 ms) = pre-excitation (WPW) or junctional rhythm
- Long (>200 ms) = 1st degree AV block (or worse)
- Progressively getting longer until a QRS drops = Mobitz I (Wenckebach)
- Constant PR with random dropped QRS = Mobitz II
- P and QRS completely independent = 3rd degree (complete) heart block
Step 6 - QRS Complex
- Wide QRS (>120 ms): bundle branch block, ventricular rhythm, WPW, hyperkalemia
- RBBB pattern: RSR' (bunny ears) in V1, wide S in I and V6 - "WiLLiaM MaRRoW" (LBBB: W in V1, M in V6)
- LBBB pattern: Broad notched R in I, V5, V6; QS in V1
- Pathological Q waves (>25% of R height or >40 ms wide): old MI in that territory
- Low voltage (<5 mm in limb leads, <10 mm in precordial): pericardial effusion, emphysema, hypothyroidism
Step 7 - ST Segment and T Waves
- ST elevation (>1 mm in 2 contiguous limb leads, >2 mm in 2 chest leads): STEMI until proven otherwise
- ST depression (≥0.5 mm in ≥2 contiguous leads): ischemia, NSTEMI, digoxin
- T wave inversion: ischemia, LVH strain, RBBB, PE, intracranial hemorrhage
- Tall peaked T waves: hyperkalemia (early sign)
- Prolonged QT: risk of torsades de pointes - drugs, hypokalemia, hypocalcemia
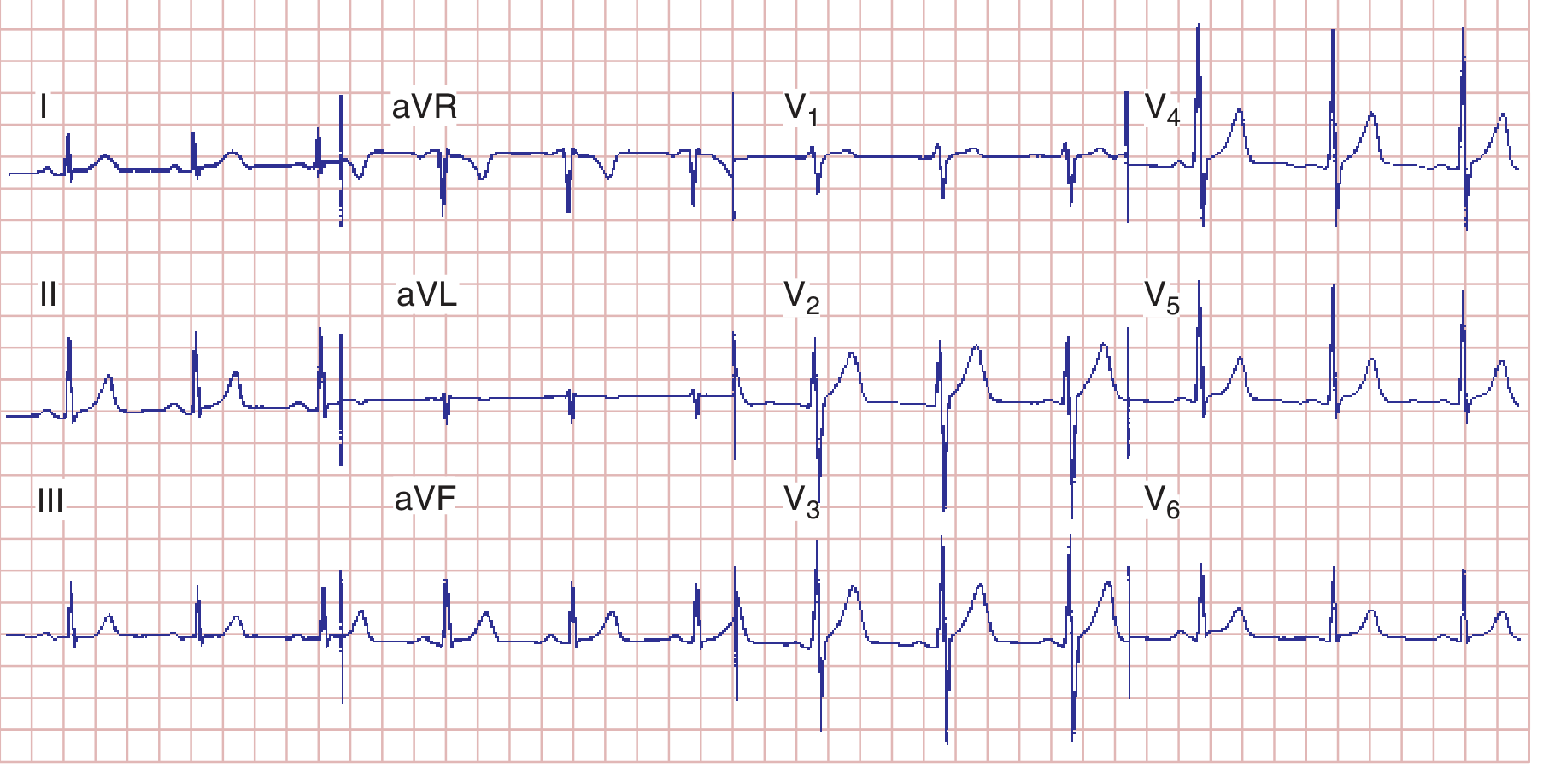
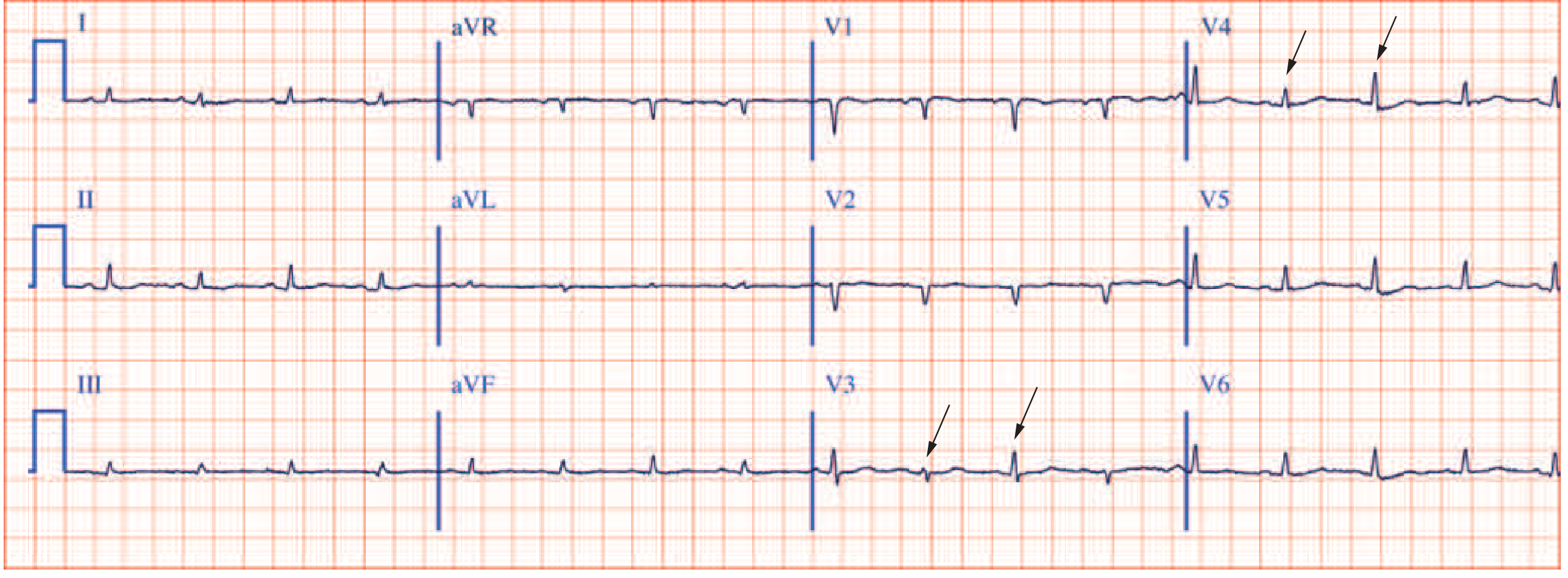
Part 5 - Normal 12-Lead ECG (Reference)
This is a normal ECG from a healthy male: regular sinus rhythm at 75 bpm, PR 160 ms, QRS 80 ms, normal axis.
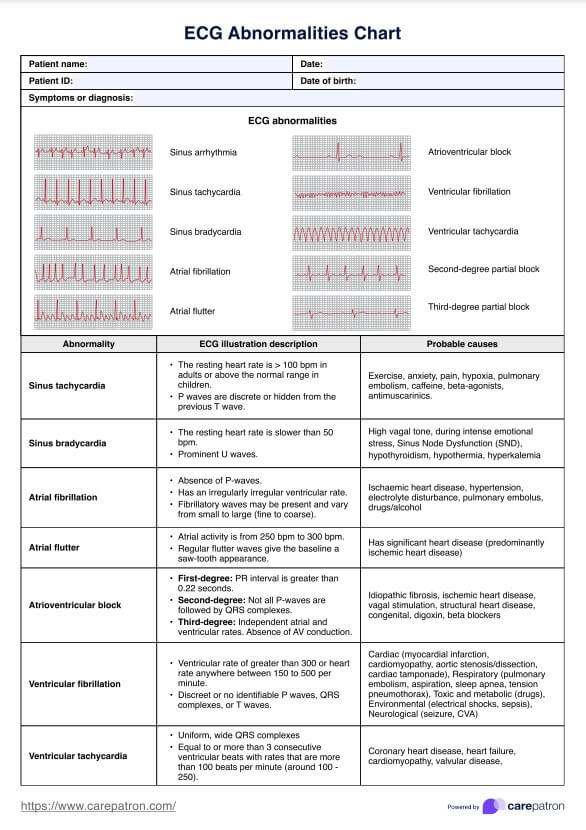
Part 6 - Common ECG Abnormalities
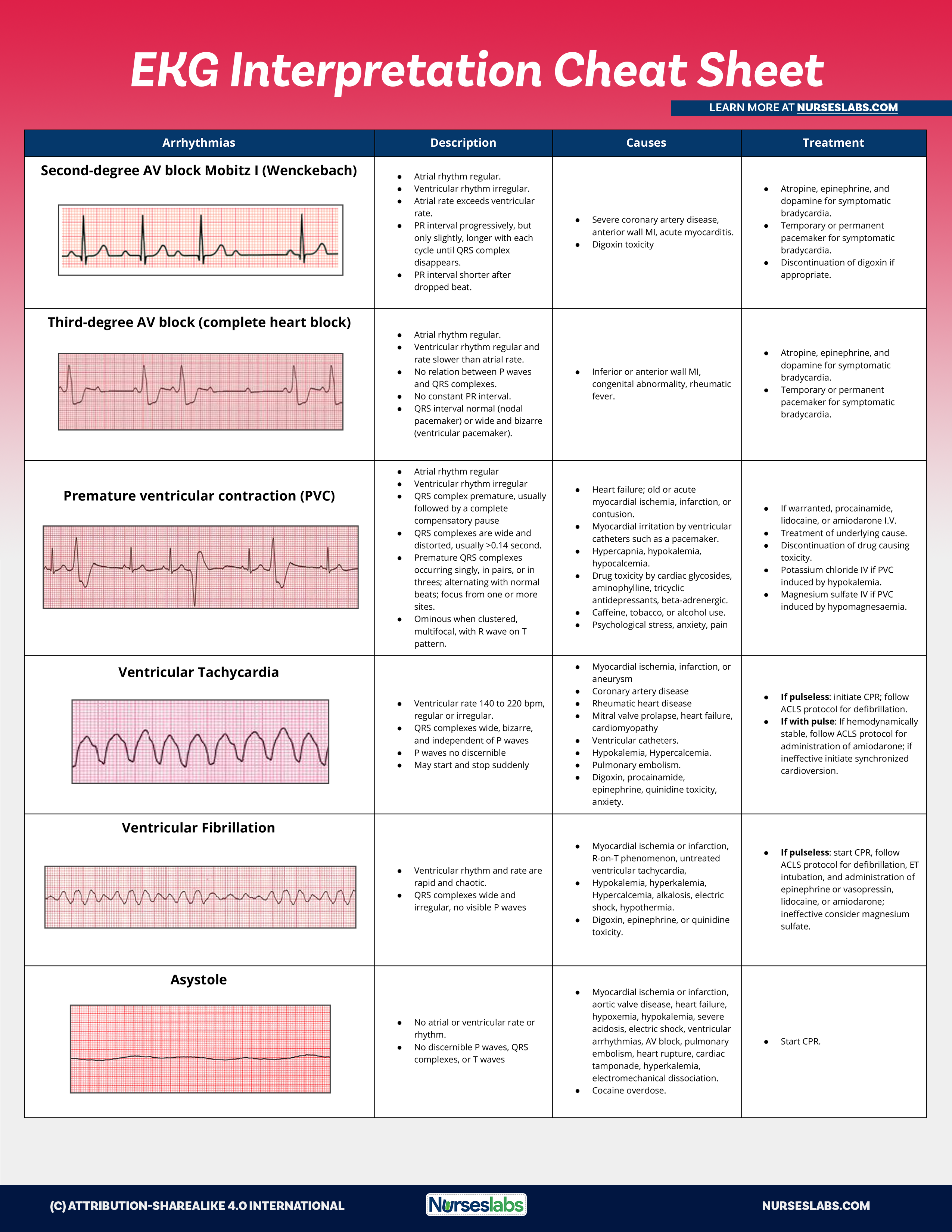
Arrhythmia/Rhythm Overview Chart
Killer Rhythms and Special Patterns
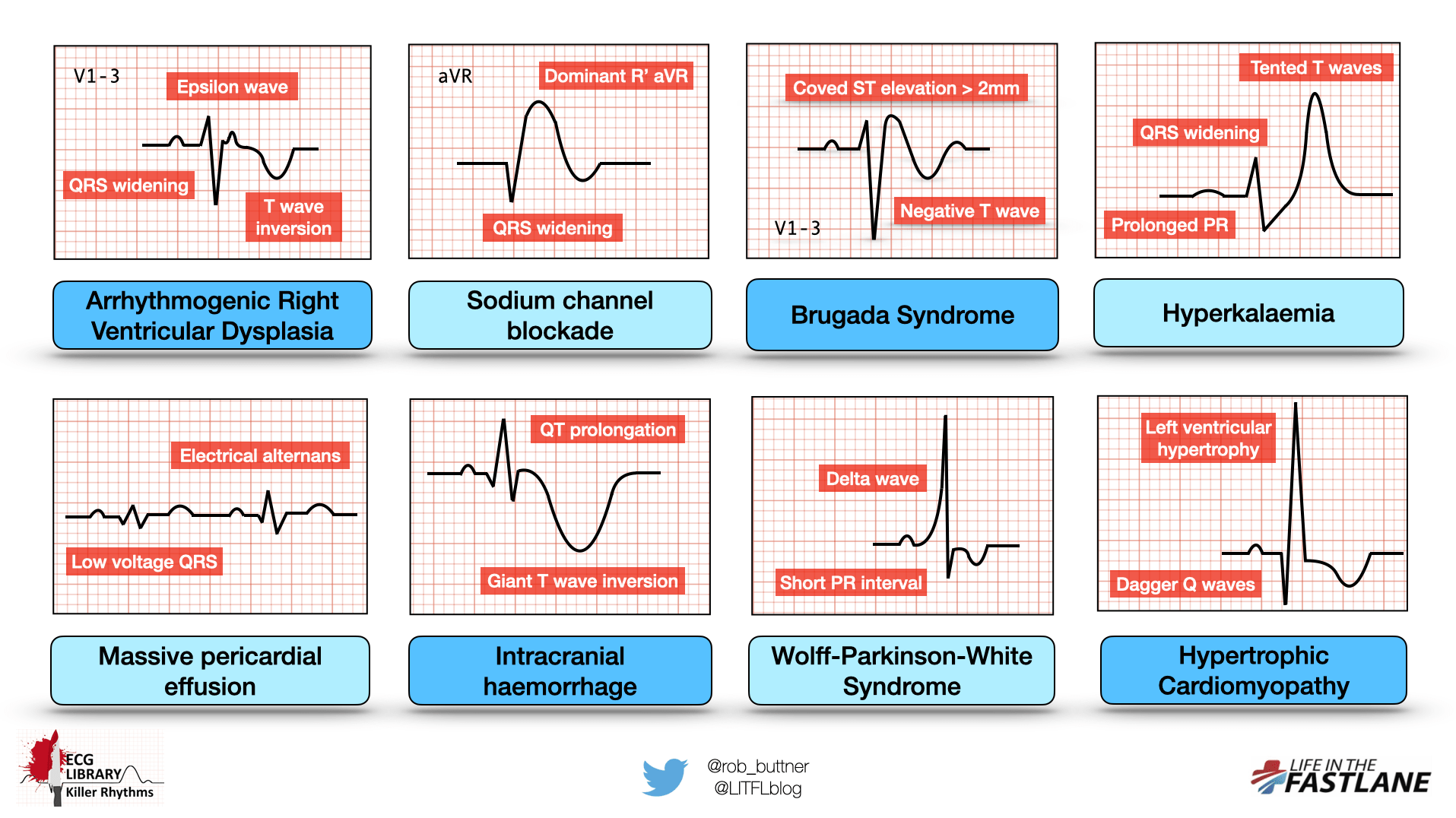
Here are the most clinically important ECG abnormalities explained individually:
1. Sinus Tachycardia
Disease: Fever, pain, anxiety, hypovolemia, pulmonary embolism, hyperthyroidism
- Rate >100 bpm
- Normal P waves before every QRS
- Regular rhythm
2. Sinus Bradycardia
Disease: High vagal tone, hypothyroidism, hypothermia, sick sinus syndrome, beta-blockers
- Rate <60 bpm
- Normal P waves, regular
- Prominent U waves possible
3. Atrial Fibrillation (AF)
Disease: Ischemic heart disease, hypertension, valve disease, thyrotoxicosis, alcohol
- Absent P waves - replaced by irregular fibrillatory baseline
- Irregularly irregular ventricular rhythm
- Normal or narrow QRS (unless aberrant conduction)
4. Atrial Flutter
Disease: Significant structural heart disease, ischemia
- Sawtooth flutter waves at 250-300 bpm
- Regular atrial activity
- Usually 2:1, 3:1 or 4:1 block giving regular ventricular rates of 150, 100 or 75 bpm
5. 1st Degree AV Block
Disease: Vagal tone, digoxin, inferior MI, myocarditis
- PR interval >200 ms (>5 small boxes)
- Every P followed by a QRS (no dropped beats)
6. 2nd Degree AV Block - Mobitz I (Wenckebach)
Disease: Inferior MI, digoxin toxicity, myocarditis
- PR interval progressively lengthens until a QRS is dropped
- Cycle repeats
- PR shortest after the dropped beat
7. 2nd Degree AV Block - Mobitz II
Disease: Anterior MI, idiopathic fibrosis, structural heart disease
- Constant PR interval with suddenly dropped QRS (no warning)
- More serious than Mobitz I - can progress to complete block
- Often needs pacemaker
8. 3rd Degree (Complete) AV Block
Disease: Inferior/anterior MI, congenital, Lyme disease, medication toxicity
- P waves and QRS complexes completely independent (no relationship)
- Atrial rate > ventricular rate (escape rhythm)
- Wide, slow QRS if ventricular escape; narrow if junctional escape
- Requires emergency pacing if symptomatic
9. STEMI (ST-Elevation Myocardial Infarction)
Disease: Acute full-thickness myocardial infarction (coronary occlusion)
- ST elevation >1 mm in ≥2 contiguous limb leads, or >2 mm in ≥2 chest leads
- Later: pathological Q waves develop (infarction)
- Territory localization (inferior = II/III/aVF; anterior = V1-V4; lateral = I/aVL/V5-V6)
10. NSTEMI / Ischemia
Disease: Partial coronary occlusion, demand ischemia
- ST depression ≥0.5 mm in ≥2 contiguous leads
- T-wave inversion in ischemic territory
- No ST elevation
11. Left Bundle Branch Block (LBBB)
Disease: LVH, ischemic heart disease, cardiomyopathy, hypertension
- QRS >120 ms (broad)
- M-shaped (notched) R wave in I, V5, V6
- QS pattern in V1
- New LBBB in chest pain = treat as STEMI equivalent
12. Right Bundle Branch Block (RBBB)
Disease: Pulmonary embolism, RV disease, congenital (may be normal)
- QRS >120 ms
- RSR' (rabbit ears / M pattern) in V1
- Wide slurred S wave in I and V6
- Remember: WiLLiaM (LBBB) and MaRRoW (RBBB) mnemonic
13. Wolff-Parkinson-White (WPW) Syndrome
Disease: Accessory conduction pathway (Bundle of Kent) bypassing AV node
- Short PR interval (<120 ms)
- Delta wave - slurred, slow upstroke of QRS
- Wide QRS
- Risk of SVT and, in AF, rapid conduction causing VF
14. Ventricular Tachycardia (VT)
Disease: MI, cardiomyopathy, electrolyte abnormalities, drug toxicity
- Rate 100-250 bpm, regular
- Wide, bizarre QRS complexes (>120 ms)
- P waves absent or dissociated from QRS
- Life-threatening - do not mistake for SVT with aberrancy
15. Ventricular Fibrillation (VF)
Disease: Cardiac arrest - MI, cardiomyopathy, electrocution, drowning
- Chaotic, rapid, irregular deflections
- No organized P waves, QRS, or T waves
- Pulseless cardiac arrest - immediate defibrillation required
16. Premature Ventricular Complexes (PVCs)
Disease: Anxiety, stimulants, electrolyte disturbances, ischemia, heart failure
- Wide, bizarre QRS appearing early (no preceding P wave)
- Full compensatory pause follows
- Concerning if: frequent (>10/hour), runs of 3+ (= non-sustained VT), R-on-T phenomenon
17. Hyperkalemia
Disease: Renal failure, ACE inhibitors, potassium-sparing diuretics, Addison's disease
Progressive ECG changes with rising K+:
- Tall, tented (peaked) T waves (early - K+ ~5.5-6.5 mmol/L)
- Widening QRS + flattened P waves (K+ ~6.5-7.0)
- Sine-wave pattern
- VF / asystole (severe)
18. Hypokalemia
Disease: Diarrhea, vomiting, diuretics, hyperaldosteronism
- Flattened or inverted T waves
- Prominent U waves (may appear as QT prolongation)
- Risk of torsades de pointes
19. Prolonged QT / Torsades de Pointes
Disease: Drugs (quinidine, amiodarone, antipsychotics, some antibiotics), hypokalemia, hypocalcemia, congenital long QT syndrome
- QTc >440 ms in men or >460 ms in women
- Risk of self-terminating runs of torsades de pointes ("twisting of the points" - QRS complexes twist around the baseline)
- Can degenerate to VF
ECG from Harrison's showing QT prolongation with hypocalcemia:
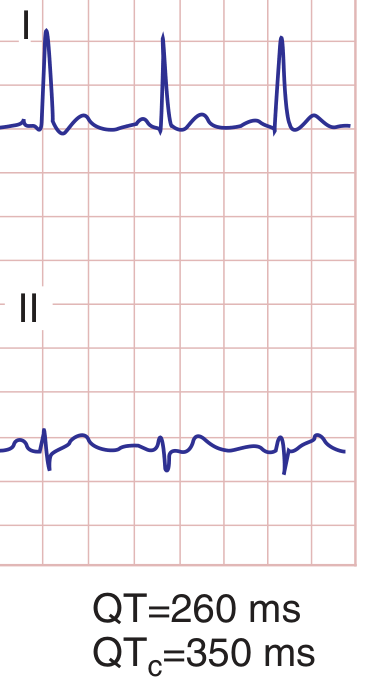 Harrison's Principles of Internal Medicine 22E - QT prolongation typical of hypocalcemia
Harrison's Principles of Internal Medicine 22E - QT prolongation typical of hypocalcemia
20. Pericardial Effusion / Cardiac Tamponade
Disease: Pericarditis, malignancy, trauma, uraemia, aortic dissection
Classic triad on ECG:
- Sinus tachycardia
- Low voltage QRS (<5 mm in limb leads)
- Electrical alternans - QRS height alternates beat-to-beat (from the heart swinging in fluid)
21. Brugada Syndrome
Disease: Genetic Na+ channel mutation - risk of sudden cardiac death
- Coved ST elevation >2 mm in V1-V3
- Followed by a negative T wave
- Right bundle branch block-like morphology
- Can occur in young, otherwise healthy people - especially at rest/sleep
22. Pulmonary Embolism (PE)
Disease: Acute massive pulmonary embolism causing right heart strain
- Sinus tachycardia (most common)
- Classic but uncommon: S1Q3T3 pattern (S wave in I, Q wave + T wave inversion in III)
- Right axis deviation
- RBBB (new)
- T wave inversions in V1-V4 (right heart strain)
Part 7 - Full ECG Abnormalities Summary Chart
Quick-Reference Cheat Sheet
| Finding | Think of |
|---|---|
| No P waves, irregularly irregular | Atrial fibrillation |
| Sawtooth P waves ~300/min | Atrial flutter |
| Long PR (>200 ms) | 1st degree AV block |
| PR lengthens then dropped QRS | Mobitz I (Wenckebach) |
| Constant PR, sudden dropped QRS | Mobitz II |
| P and QRS independent, slow rate | Complete (3rd degree) heart block |
| ST elevation, chest pain | STEMI - emergent |
| Wide QRS, RSR' in V1 | Right bundle branch block |
| Wide QRS, M-shaped in V5/V6 | Left bundle branch block |
| Short PR + delta wave | WPW |
| Tall peaked T waves | Hyperkalemia |
| Prominent U waves | Hypokalemia |
| Prolonged QTc | Long QT - torsades risk |
| Low voltage + alternans | Pericardial effusion/tamponade |
| ST elevation V1-V3 with coved pattern | Brugada syndrome |
| Wide QRS tachycardia | Ventricular tachycardia until proven otherwise |
Sources: Harrison's Principles of Internal Medicine 22E (2025); Braunwald's Heart Disease 12th Ed; Medical Physiology (Boron & Boulpaep); Geeky Medics ECG Guide; Life in the Fast Lane ECG Library; Nurseslabs EKG Cheat Sheet
This is a shared conversation. Sign in to Orris to start your own chat.