What are effects of dead space on alveolar ventilation
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a thorough, textbook-grounded answer on the effects of dead space on alveolar ventilation.
Dead Space and Its Effects on Alveolar Ventilation
1. What Is Dead Space?
Dead space refers to the volume of air that is breathed in with each tidal breath but does not participate in gas exchange. It has two components:
| Type | Description | Normal Volume |
|---|---|---|
| Anatomic dead space | Air in conducting airways (nose, pharynx, trachea, bronchi, bronchioles) - no gas exchange walls | ~150 mL |
| Alveolar dead space | Alveoli that are ventilated but not perfused (V/Q = infinity) | ~0 in healthy lungs |
| Physiologic dead space | Anatomic + alveolar dead space combined | ~150 mL (normal) |
In healthy lungs, anatomic and physiologic dead space are nearly equal. In diseased lungs, physiologic dead space can reach 1-2 liters - as much as 10 times the anatomical dead space. (Guyton & Hall, p. 499)
2. The Core Equation: How Dead Space Reduces Alveolar Ventilation
The defining relationship is:
VA = (VT - VD) × Respiratory Rate
Where:
- VA = alveolar ventilation (mL/min)
- VT = tidal volume (mL)
- VD = physiologic dead space (mL)
Normal example (Guyton & Hall):
VA = 12 × (500 mL - 150 mL) = 4,200 mL/min
Only the portion of each breath that exceeds dead space volume reaches the gas exchange zones. Dead space air is expired first on exhalation - before any alveolar gas reaches the atmosphere - making it directly "wasted" ventilation. (Guyton & Hall, p. 499)
3. Effect on Gas Exchange: The Alveolar Ventilation Equation
Dead space, by reducing VA, directly drives changes in alveolar (and arterial) gas tensions via:
PACO₂ = (VCO₂ × K) / VA
- If VA falls (dead space rises) → PACO₂ rises → PaCO₂ rises → hypercapnia
- If VA rises (dead space falls or breathing deepened) → PACO₂ falls → hypocapnia
The relationship between PACO₂ and VA is hyperbolic: small reductions in alveolar ventilation at low VA values cause large CO₂ rises. (Costanzo Physiology, p. 201)
Similarly, PAO₂ falls when alveolar ventilation is reduced (less fresh O₂ delivered), leading to hypoxemia.
4. Dead Space vs. Alveolar Ventilation: Clinical Comparison
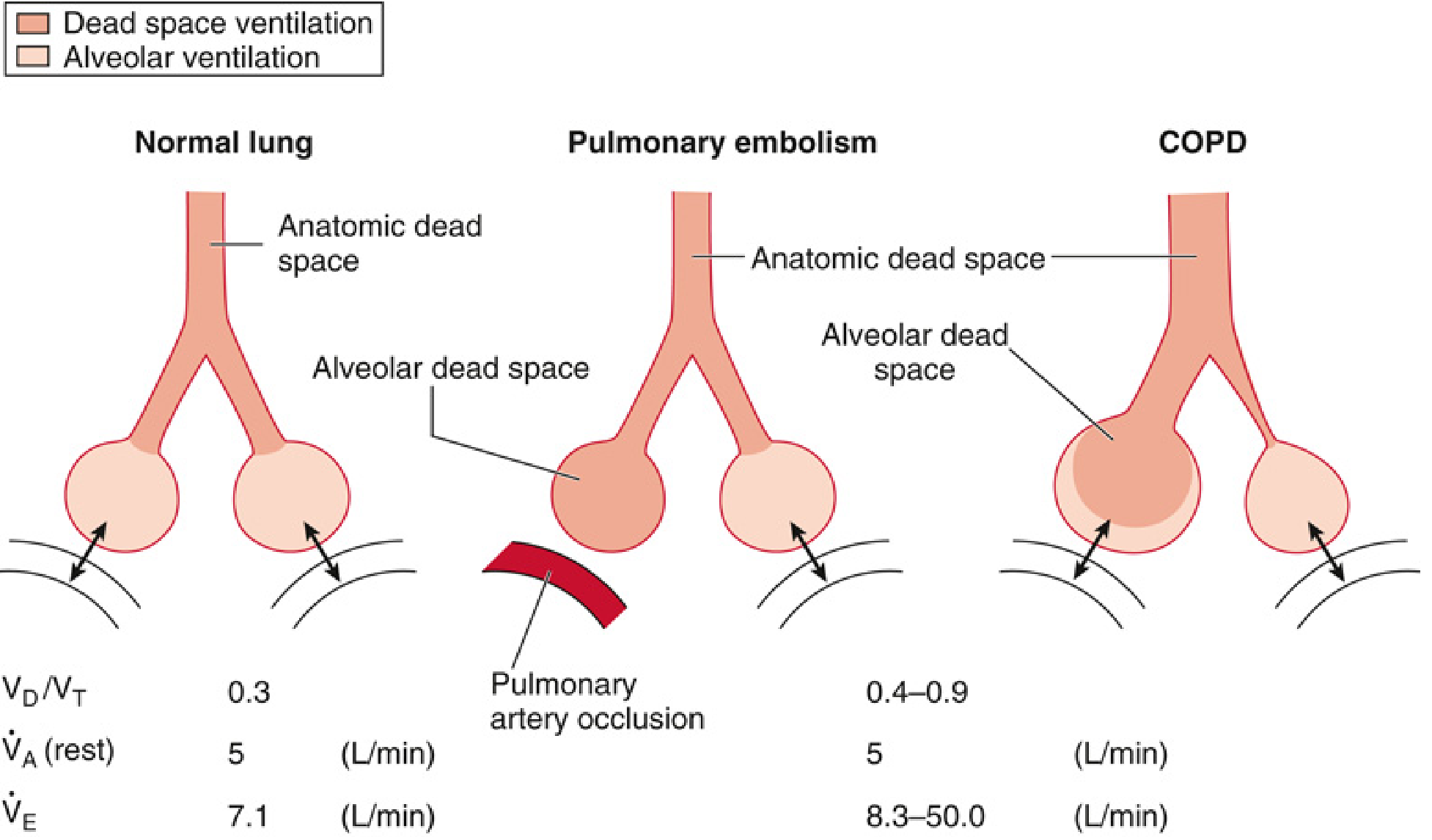
| Condition | VD/VT | VA (at rest) | Minute Ventilation (VE) needed |
|---|---|---|---|
| Normal | 0.3 | 5 L/min | 7.1 L/min |
| Pulmonary embolism | Increased | 5 L/min | 8.3-50.0 L/min |
| COPD | 0.4-0.9 | 5 L/min | Much higher |
Key insight: To maintain the same alveolar ventilation (5 L/min) in the face of increased dead space, minute ventilation must increase substantially. Patients who cannot compensate develop CO₂ retention. (Miller's Anesthesia, p. 1239)
5. Effect of Breathing Pattern on Dead-Space Impact
Because dead space is a fixed volume per breath, breathing pattern profoundly affects its relative impact:
| Breathing Pattern | Effect on Alveolar Ventilation |
|---|---|
| Rapid, shallow breathing (low VT, high rate) | VT approaches VD → alveolar ventilation collapses. If VT = VD, no fresh air reaches alveoli at all |
| Slow, deep breathing (high VT, low rate) | Dead space is a smaller fraction of each breath; alveolar ventilation is preserved or increased |
Example from Guyton & Hall: At 12 breaths/min and VT = 150 mL (equal to dead space), alveolar ventilation = 0, even though minute ventilation = 1,800 mL/min. Deep slow breaths are far more efficient.
6. Alveolar Dead Space: V/Q Mismatch at the Extreme
When alveoli are ventilated but receive no blood flow (V/Q = infinity), as in pulmonary embolism:
- Those alveoli add to physiologic dead space
- They dilute CO₂ from normal alveoli, making expired gas hypocapnic relative to arterial blood
- This is the basis of the Bohr equation for measuring dead space:
VD/VT = (PaCO₂ - PeCO₂) / PaCO₂
where PeCO₂ is the partial pressure of CO₂ in mixed expired air. (Costanzo Physiology, p. 200)
Compensatory bronchospasm: When alveoli are unperfused (alveolar dead space), local CO₂ in those alveoli falls (no blood to add CO₂). This alkaline environment triggers bronchiolar constriction, redirecting airflow to better-perfused areas - a lung efficiency mechanism. (Medical Physiology - Boron & Boulpaep, p. 1021)
7. Clinical Consequences of Increased Dead Space
- Hypercapnia (CO₂ retention) - when the patient cannot increase minute ventilation enough to compensate
- Hypoxemia - reduced alveolar PO₂ due to decreased fresh air delivery
- Increased work of breathing - patients must breathe harder/faster to maintain adequate VA
- Ventilatory failure - in severe disease (e.g., COPD, massive PE), VA falls and PaCO₂ rises despite maximum respiratory effort
Summary
Dead space "wastes" a fixed volume of each breath on non-exchanging airways and unperfused alveoli. The formula VA = (VT - VD) × Rate captures the key relationship: any increase in VD directly reduces alveolar ventilation unless tidal volume or rate increases to compensate. Since PACO₂ is inversely proportional to VA, rising dead space leads to CO₂ retention and hypoxemia. Slow, deep breaths minimize dead space's proportional impact; rapid, shallow breaths maximize it.
Sources:
- Guyton and Hall Textbook of Medical Physiology, pp. 497-499
- Costanzo Physiology, 7th Ed., pp. 200-201
- Miller's Anesthesia, 10th Ed., pp. 1238-1240
- Medical Physiology (Boron & Boulpaep), pp. 1020-1021
This is a shared conversation. Sign in to Orris to start your own chat.