EXPLAIN BISHOP'S SCORE
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive information to provide a thorough explanation. Here is a complete breakdown:
Bishop's Score
What Is It?
The Bishop Pelvic Scoring System (described by Dr. E.H. Bishop) is a standardized pre-labor cervical assessment tool used to predict the likelihood of successful induction of labor and to guide the need for cervical ripening before induction. It quantifies cervical "ripeness" (readiness for labor) through a digital examination of five parameters.
The Five Parameters (Original Score)
| Score | Dilation | Effacement (%) | Station | Position | Consistency |
|---|---|---|---|---|---|
| 0 | Closed | 0–30% | –3 | Posterior | Firm |
| 1 | 1–2 cm | 40–50% | –2 | Midposition | Moderately firm |
| 2 | 3–4 cm | 60–70% | –1, 0 | Anterior | Soft |
| 3 | 5+ cm | 80%+ | +1, +2 | — | — |
Maximum possible score: 13 (Effacement and position can score up to 3; all others up to 3 as well)
Score Interpretation
| Score | Interpretation |
|---|---|
| ≥ 9 | Favorable cervix — induction success rate approaches that of spontaneous labor; no failed inductions in Bishop's original multipara series |
| ≥ 8 | Successful vaginal delivery with oxytocin is highly likely |
| 6–8 | Intermediate; induction may be attempted |
| < 6 | Unfavorable cervix — associated with prolonged labor or failed induction; cervical ripening is recommended first |
| ≤ 5 (nullipara) | ~50% risk of failed induction |
— Textbook of Family Medicine 9e; Pfenninger and Fowler's Procedures for Primary Care
Modifiers (Score Adjustments)
Add 1 point for each of:
- Preeclampsia
- Each prior vaginal delivery
Subtract 1 point for each of:
- Post-dates pregnancy
- Nulliparity
- Premature or prolonged rupture of membranes
— Textbook of Family Medicine 9e
Clinical Significance
- Dilation is the single most important component. Lange et al. (808 patients) found dilation was dominant among all five components and recommended scoring it at twice the value given by Bishop.
- Induction procedure depends on Bishop score:
- Favorable cervix (score ≥ 6–8): Proceed with oxytocin infusion or amniotomy
- Unfavorable cervix (score < 6): First perform cervical ripening — mechanical (Foley catheter, laminaria) or pharmacologic (dinoprostone/PGE₂, misoprostol)
- Transvaginal ultrasound of cervical length does not improve upon the Bishop score in predicting induction success.
— Creasy & Resnik's Maternal-Fetal Medicine
Simplified Bishop Score
A simplified 3-parameter version uses only dilation, effacement, and station (range 0–9). Research from the Consortium on Safe Labor (Laughton et al., 5,610 nulliparous women) showed this simplified 9-point system had better positive and negative predictive values than the traditional 5-component method across all populations tested (term induction, preterm induction, spontaneous labor).
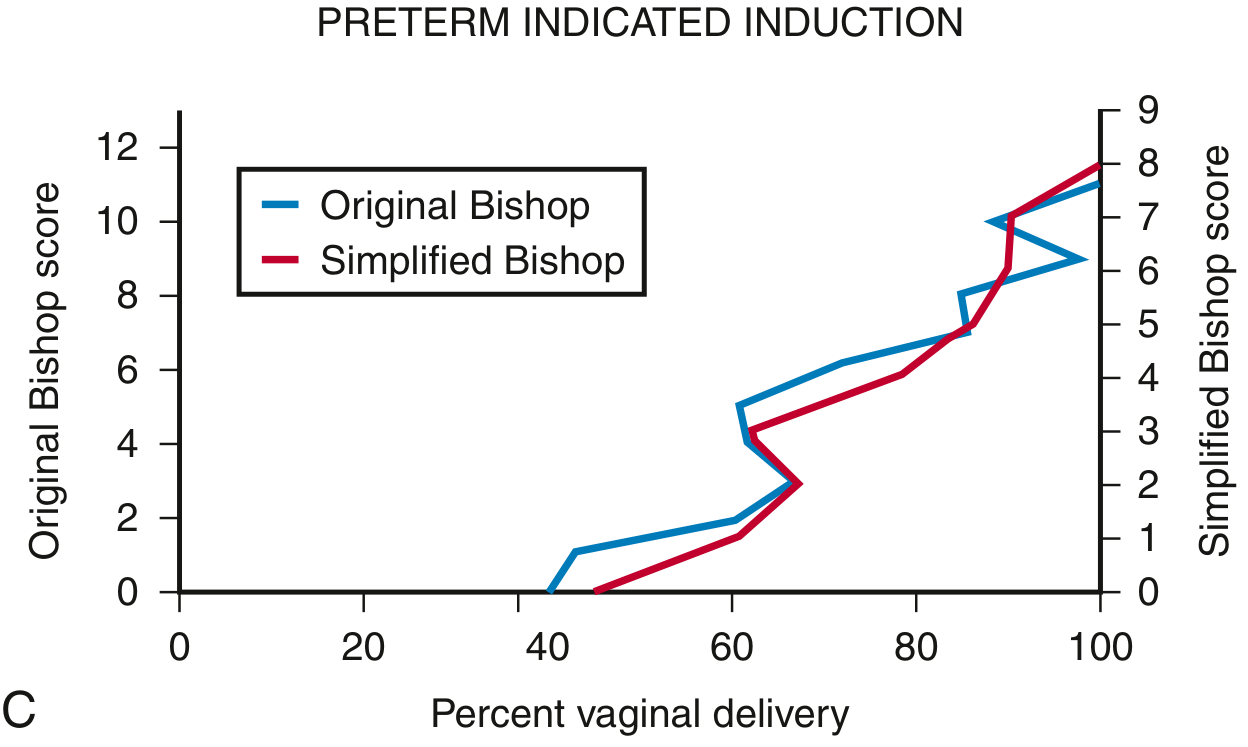
Figure: Comparison of Original vs. Simplified Bishop score vs. rate of vaginal delivery (preterm indicated induction). Both systems track closely, confirming the simplified score's utility. — Creasy & Resnik's Maternal-Fetal Medicine
When to Calculate Bishop Score
Before any method of labor induction, a cervical assessment and Bishop score must be calculated. This should be combined with a nonstress test (NST) and assessment for regular uterine contractions. If the NST is non-reactive or a normal contraction pattern is already present, induction medications should not be initiated at that time.
Memory Aid — "DECPS" (5 Parameters)
| Letter | Parameter |
|---|---|
| D | Dilation |
| E | Effacement |
| C | Consistency |
| P | Position |
| S | Station |
Key thresholds to remember:
- Score < 6 → ripen first
- Score ≥ 8–9 → go ahead with induction (favorable)
This is a shared conversation. Sign in to Orris to start your own chat.