i am very nervous and confused about large,medium and small vessel and its vasculitis
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
Reading File
Loading Image
Reading File
I now have everything I need for a thorough, well-organized answer. Let me compile this clearly.
Vasculitis: Large, Medium & Small Vessel - A Complete Guide
Don't be nervous - once you see the logic of the classification, it all clicks into place. The entire framework is based on which vessel size is predominantly affected.
The Master Diagram - Chapel Hill Consensus Classification
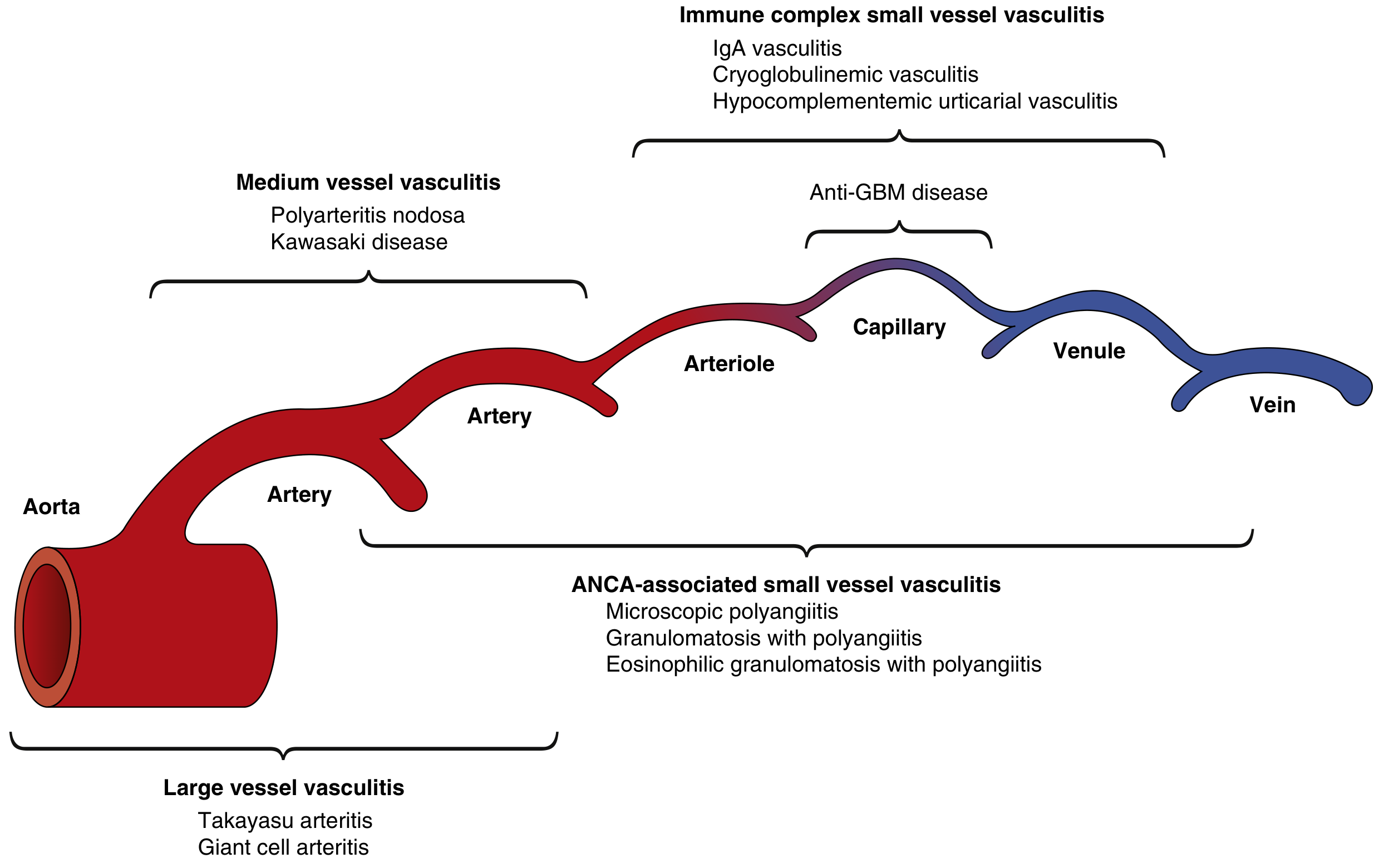
The predominant distribution of vessel involvement by vasculitis type. ANCA-associated vasculitis affects the broadest spectrum; immune complex vasculitis is mostly restricted to capillaries/venules. - Henry's Clinical Diagnosis and Management, p. 1217
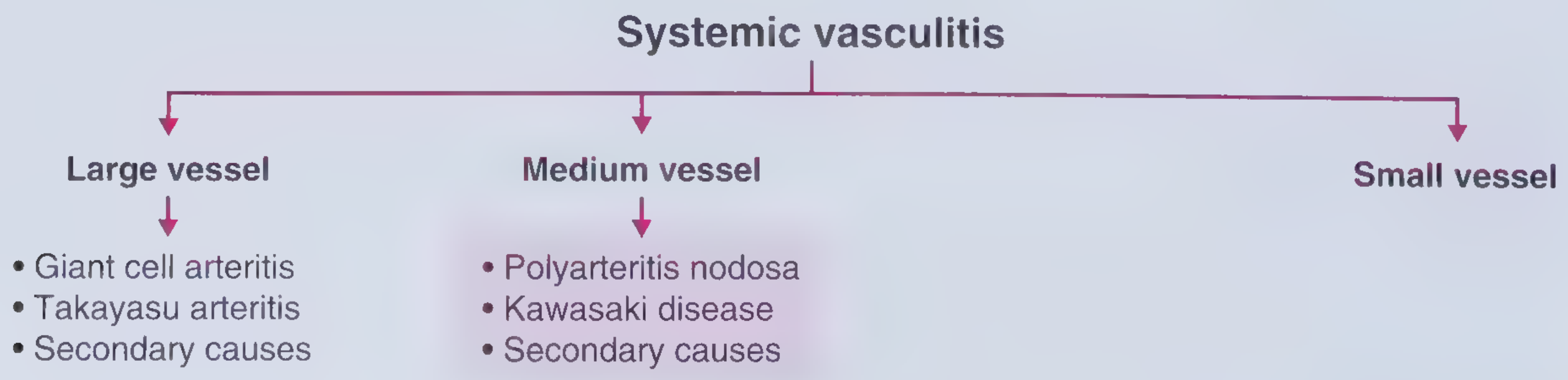
The Core Framework
| Category | Vessels Affected | Diseases |
|---|---|---|
| Large vessel | Aorta + major branches | Giant Cell Arteritis, Takayasu Arteritis |
| Medium vessel | Main visceral arteries + branches | Polyarteritis Nodosa, Kawasaki Disease |
| Small vessel | Arterioles, capillaries, venules | GPA, MPA, EGPA, IgA vasculitis, Cryoglobulinemic, Anti-GBM |
Important rule: overlap exists. Medium vessel vasculitis can also hit small arteries, and large vessel vasculitis can involve medium-sized vessels. But the predominant target is what defines the category. - Goldman-Cecil Medicine, p. 2848
LARGE VESSEL VASCULITIS (LVV)
Affects the aorta and its major branches. Key distinction is by age:
1. Giant Cell Arteritis (GCA) - "Temporal Arteritis"
- Age: >50 years (almost exclusively). More common in women
- Target vessels: Extracranial branches of the aorta, especially temporal artery and other branches of the carotid/vertebral arteries. Spares intracranial vessels
- Pathology: Granulomatous arteritis
- Classic symptoms:
- New-onset headache (temporal region)
- Jaw claudication (prandial jaw pain - highly specific)
- Scalp tenderness
- Visual loss (ischemic optic neuropathy - an emergency!)
- Palpable, tender, cord-like thickened temporal artery
- Associated condition: Polymyalgia rheumatica (PMR) - pain and stiffness of neck, shoulders, hips, thighs. About 50% of GCA patients have PMR; ~15% of isolated PMR patients eventually develop GCA
- Diagnosis: Temporal artery biopsy (gold standard)
- Physical signs: Asymmetric pulses, BP discrepancy between arms, bruits
Temporal artery may be tender, red, enlarged, tortuous, or nodular with decreased pulsation - Frameworks for Internal Medicine, p. 692
2. Takayasu Arteritis
- Age: <50 years - adolescent girls and young women (2nd-3rd decade), especially from Japan, Southeast Asia, India
- Target vessels: Aorta and major branches (subclavian, carotid, renal arteries)
- Pathology: Granulomatous; cannot be distinguished from GCA by pathology alone - age is the key differentiator
- Classic symptoms:
- Pulseless disease - absent or weak pulses in upper extremities
- Discrepant blood pressure between arms
- Bruits over affected vessels
- Hypertension (from renal artery involvement)
- Arm or leg claudication
- Classic presentation: Young non-smoking woman with pulseless extremities and BP discrepancy
MEDIUM VESSEL VASCULITIS (MVV)
Affects the main visceral arteries and their branches (mesenteric, renal, hepatic, coronary arteries). Note: the renal artery itself is a "large vessel" but its intralobar branches - interlobar and arcuate arteries - are medium-sized. - Goldman-Cecil, p. 2847
1. Polyarteritis Nodosa (PAN)
- Age: Older adults; all genders and races
- Key association: Historically linked to Hepatitis B (now <5% in developed countries due to vaccination; used to be >35%)
- Target vessels: Main visceral arteries especially renal, mesenteric, hepatic, coronary. Also epineural arteries (causing mononeuritis multiplex) and subcutaneous arteries
- Does NOT affect: Lungs (pulmonary vessels spared - key distinguisher from ANCA vasculitis), glomerular capillaries
- Pathology: Necrotizing arteritis - fibrinoid necrosis with neutrophil-rich inflammation, evolves to fibrosis. Segmental involvement at branch points
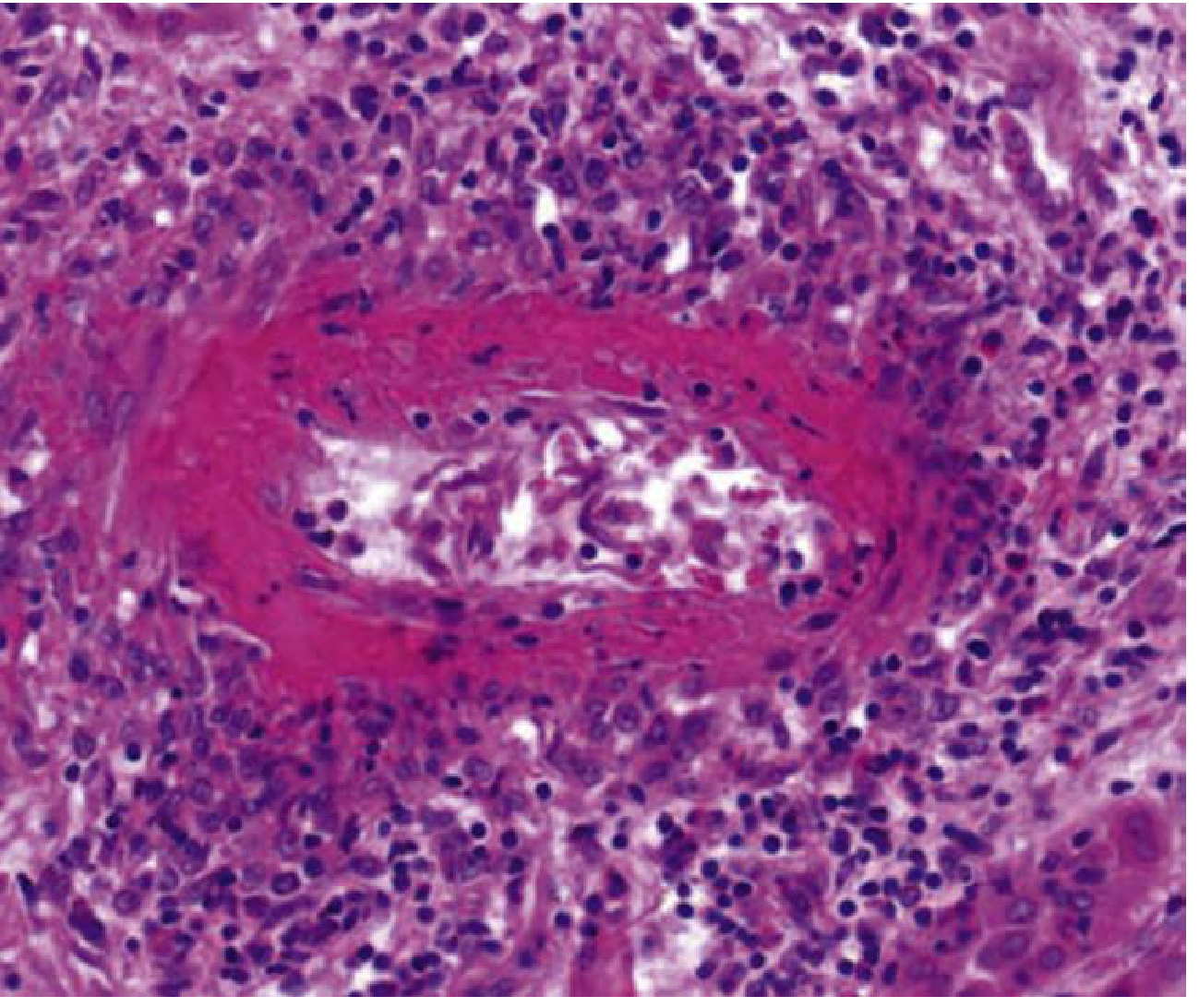
Necrotizing arteritis of PAN: fibrinoid necrosis replacing the media with perivascular inflammation - Henry's Clinical Diagnosis, p. 1220
- Classic symptoms:
- Fever, weight loss, fatigue
- Testicular pain (highly specific - testicular artery involvement)
- Mononeuritis multiplex (foot drop, wrist drop)
- Hypertension (renovascular)
- Livedo reticularis, skin nodules
- Abdominal pain (mesenteric ischemia)
- Classic arteriographic finding: Multiple microaneurysms (1-5 mm) in renal, mesenteric, hepatic arteries
- ANCA negative (important distinguisher from MPA/GPA)
2. Kawasaki Disease
- Age: Children (typically <5 years); Japan and East Asia highest rates
- Pathology: Necrotizing arteritis (similar histology to PAN)
- Classic "CRASH" criteria:
- Conjunctival injection (bilateral, non-purulent)
- Rash (polymorphous)
- Adenopathy (cervical lymphadenopathy >1.5 cm)
- Strawberry tongue / lip cracking / oral mucositis
- Hand/foot swelling (edema with desquamation later)
-
- Fever >5 days
- Feared complication: Coronary artery aneurysms (can cause MI even in young children; overall mortality up to 3%)
- Treatment: IVIG + Aspirin (early treatment prevents coronary aneurysms)
- Generally self-limited
SMALL VESSEL VASCULITIS (SVV)
Affects arterioles, capillaries, and venules. Divided into two major groups:
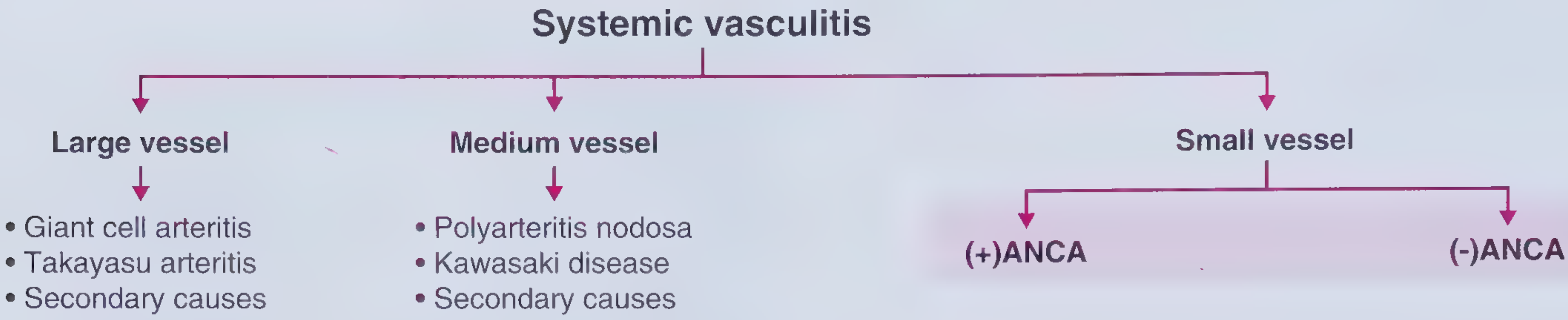
GROUP A: ANCA-Associated Vasculitis (AAV)
ANCA = Antineutrophil cytoplasmic antibodies - directed against proteins in neutrophil cytoplasm (PR3 and MPO).
- c-ANCA (cytoplasmic pattern) = anti-PR3 antibodies → associated with GPA
- p-ANCA (perinuclear pattern) = anti-MPO antibodies → associated with MPA and EGPA
1. Granulomatosis with Polyangiitis (GPA) - formerly Wegener's
- ANCA: c-ANCA (anti-PR3) - ~90% positive
- Classic triad: Upper airway + Lower airway + Kidneys
- Upper airway (95%): Chronic sinusitis, nasal septal perforation, saddle nose deformity, epistaxis, otitis media
- Lower airway: Pulmonary nodules, cavities, hemoptysis (pulmonary capillaritis)
- Kidney: Crescentic glomerulonephritis (pauci-immune - little/no immune deposits on IF)
- Pathology: Necrotizing granulomatous inflammation + vasculitis (granulomas = key distinguisher from MPA)
- Classic case: Middle-aged person with sinusitis + hemoptysis + hematuria + c-ANCA positive
2. Microscopic Polyangiitis (MPA)
- ANCA: p-ANCA (anti-MPO) - most common
- Key distinguisher from GPA: NO granulomatous inflammation, NO upper airway disease
- Key distinguisher from PAN: Affects glomerular capillaries (renal involvement very common, >80%), affects pulmonary capillaries
- Renal involvement: Most common manifestation - rapidly progressive glomerulonephritis (pauci-immune crescentic GN)
- Can also involve: Skin (palpable purpura), lungs, GI, peripheral nerves
- Classic case: Patient with hemoptysis + hematuria + p-ANCA (pulmonary-renal syndrome)
3. Eosinophilic Granulomatosis with Polyangiitis (EGPA) - formerly Churg-Strauss
- ANCA: p-ANCA (anti-MPO) - but only ~40-60% positive
- The asthma vasculitis - the only vasculitis that begins with asthma
- Classic triad (three phases):
- Allergic phase: Asthma + allergic rhinitis (can precede vasculitis by years)
- Eosinophilic phase: Peripheral eosinophilia (>1500 cells/μL or >10%), eosinophilic organ infiltration
- Vasculitic phase: Frank small vessel vasculitis
- Key findings: Asthma + palpable purpura + mononeuritis multiplex (wrist/foot drop) + eosinophilia
- Pathology: Necrotizing granulomatous inflammation with abundant eosinophils in granulomas and vasculitis (eosinophils = key distinguisher from GPA)
GROUP B: Non-ANCA Small Vessel Vasculitis (Immune Complex-mediated)
These involve immune complex deposition in vessel walls.
4. IgA Vasculitis (Henoch-Schönlein Purpura - HSP)
- Mechanism: IgA immune complex deposition
- Classic in: Children (after upper respiratory infection); can occur in adults
- Classic tetrad:
- Palpable purpura (lower limbs - dependent areas; non-thrombocytopenic)
- Arthritis/arthralgias (knees, ankles)
- Abdominal pain (GI vasculitis - can cause intussusception)
- Renal involvement (IgA nephropathy-like: hematuria, proteinuria)
- If: presents with palpable purpura on legs after a sore throat in a child - think HSP
5. Cryoglobulinemic Vasculitis
- Association: Strongly linked to Hepatitis C (unlike PAN which is HBV)
- Cold-precipitable immunoglobulins (cryoglobulins) deposit in vessel walls
- Triad: Purpura + arthralgia + weakness (Meltzer's triad)
- Also: peripheral neuropathy, renal involvement (membranoproliferative GN)
6. Anti-GBM Disease (Goodpasture Syndrome)
- Autoantibodies against the glomerular basement membrane (type IV collagen)
- Pulmonary-renal syndrome: Pulmonary hemorrhage + rapidly progressive GN
- Young men (pulmonary component more prominent), older individuals (renal predominant)
Quick Memory Table
| Disease | Age | Sex | Key Association | ANCA | Pathology | Buzzword |
|---|---|---|---|---|---|---|
| GCA | >50 | F>M | HLA-DR4 | Neg | Granulomatous | Jaw claudication + blindness |
| Takayasu | <50 | F>>M | Asian | Neg | Granulomatous | Pulseless disease |
| PAN | Any | M>F | Hep B | Neg | Necrotizing (no granuloma) | Microaneurysms, testicular pain |
| Kawasaki | <5 yrs | M>F | Japan | Neg | Necrotizing | Strawberry tongue, coronary aneurysm |
| GPA | 40-60 | M=F | - | c-ANCA (PR3) | Necrotizing granuloma | Saddle nose, sinus+lung+kidney |
| MPA | Any | M=F | - | p-ANCA (MPO) | Necrotizing (no granuloma) | Pulmonary-renal, no upper airway |
| EGPA | 30-50 | M=F | Atopy | p-ANCA (MPO) | Granuloma + eosinophils | Asthma + eosinophilia |
| IgA vasculitis | Children | M>F | URI | Neg | Immune complex | Purpura + abdo pain + joints |
| Cryo vasculitis | Adults | F>M | Hep C | Neg | Immune complex | Purpura + neuropathy |
Key Concepts to Cement
- Large vessel = aorta and its big branches. But the renal artery (even though it goes to a visceral organ) is still "large" - its branches inside the kidney are "medium."
- PAN vs MPA - both can look similar but: PAN is ANCA-negative, spares the lungs and glomeruli; MPA is ANCA-positive, attacks both
- GPA vs MPA - both ANCA-associated but: GPA has granulomas and upper airway disease; MPA has neither
- EGPA is the only vasculitis that starts with asthma - always think of it when a patient with "difficult asthma" develops purpura or neuropathy
- Kawasaki = IVIG + Aspirin - urgent to prevent coronary aneurysms
- GCA + blindness risk = start steroids immediately without waiting for biopsy
Sources: Robbins & Kumar Basic Pathology; Henry's Clinical Diagnosis and Management by Laboratory Methods; Goldman-Cecil Medicine; Frameworks for Internal Medicine - all consulted via medical textbook library
This is a shared conversation. Sign in to Orris to start your own chat.