Traction retinal detachment
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Searching Images
traction retinal detachment fundus
Loading Image
Loading Image
Finding Sources
Reading File
Reading File
I now have comprehensive information to provide a thorough answer on traction retinal detachment.
Traction Retinal Detachment (TRD)
Definition & Pathophysiology
Traction retinal detachment occurs when fibrocellular (fibrovascular) membranes in the vitreous contract and pull the neurosensory retina away from the retinal pigment epithelium (RPE), without the presence of a retinal break (distinguishing it from rhegmatogenous RD). The forces involved are typically tangential (along the retinal surface) rather than anteroposterior.
Etiology
The common sources of fibrovascular/fibrocellular proliferation causing TRD include:
| Cause | Notes |
|---|---|
| Proliferative diabetic retinopathy (PDR) | Most common cause; neovascularization → fibrosis |
| Sickle cell retinopathy | Peripheral fibrovascular proliferation |
| Retinopathy of prematurity (ROP) | Fibrovascular ridge formation |
| Familial exudative vitreoretinopathy (FEVR) | Peripheral avascularization → traction |
| Proliferative vitreoretinopathy (PVR) | Post-rhegmatogenous or post-trauma |
| Toxocariasis | Inflammatory granuloma → fibrous bands |
| Trauma | Penetrating injury with vitreous organization |
| Coats' disease | Exudation-induced fibrosis |
— The Wills Eye Manual, p. 770
Clinical Features
Symptoms
- Visual loss or visual field defect
- May be asymptomatic, especially when extramacular
Signs (Key Features)
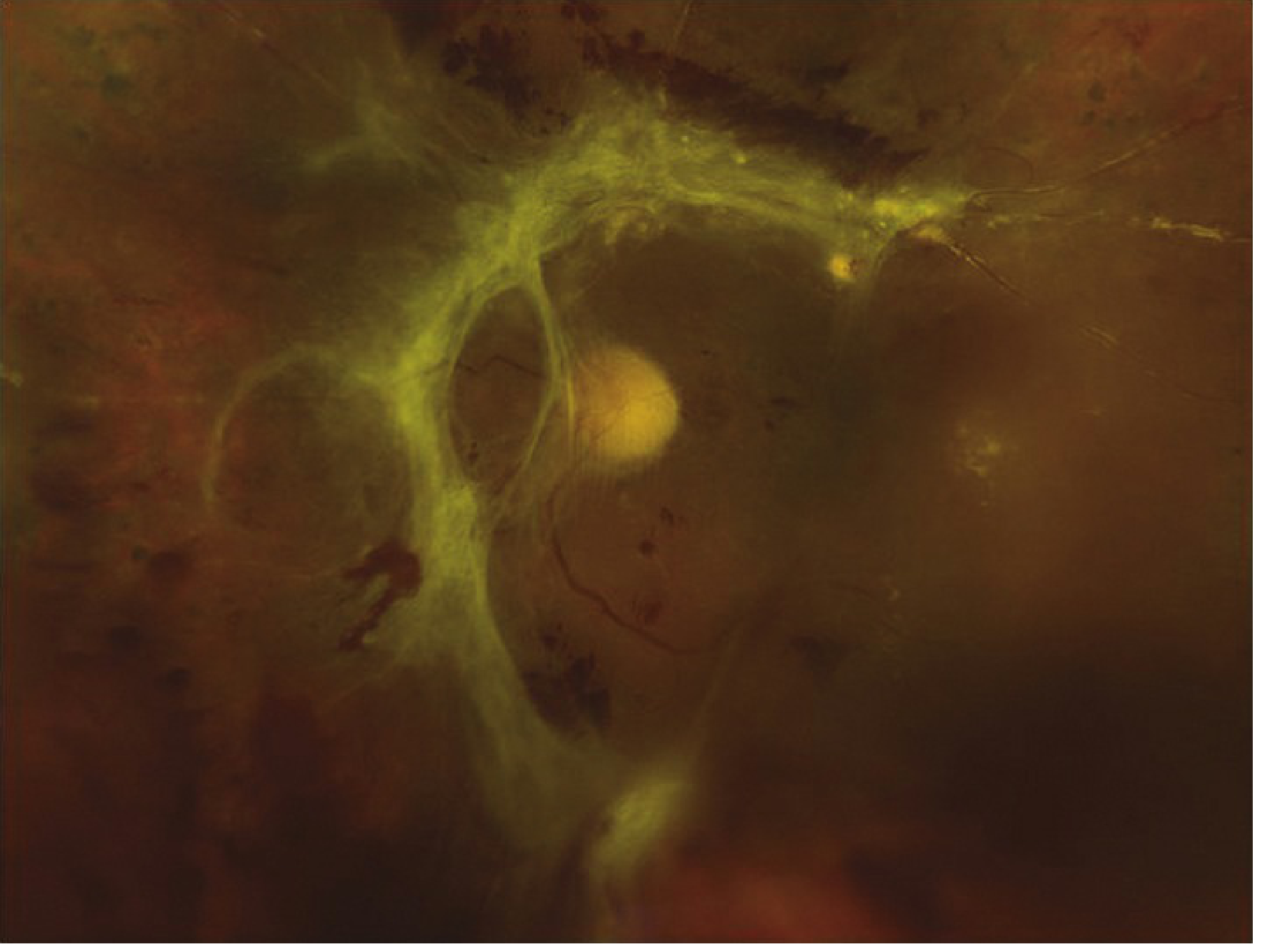
- The detached retina has a concave, tent-like configuration with a smooth surface (cf. rhegmatogenous RD which is convex/bullous)
- Cellular and vitreous fibrovascular membranes are visible exerting traction on the retina
- Retinal striae (folds) radiate from areas of traction
- The retina is immobile (does not shift with eye movement)
- Detachment rarely extends to the ora serrata
- A mild relative afferent pupillary defect (RAPD) may be present in large detachments
- If a retinal tear develops within the TRD, it converts to a combined TRD/rhegmatogenous RD — now convex and more bullous (urgent)
— The Wills Eye Manual, p. 770–771
Comparison with Other Types of Retinal Detachment
| Feature | Rhegmatogenous (RRD) | Traction (TRD) | Exudative/Serous |
|---|---|---|---|
| Mechanism | Retinal break → subretinal fluid | Fibrovascular traction | Fluid from RPE/choroid |
| Shape | Convex, bullous | Concave, tent-like | Convex, shifting |
| Surface | Corrugated, mobile | Smooth, immobile | Smooth |
| Extends to ora serrata | Yes | Rarely | Variable |
| Vitreous cells/PVR | Common | Fibrovascular membranes | No |
| Break present | Yes | No (unless combined) | No |
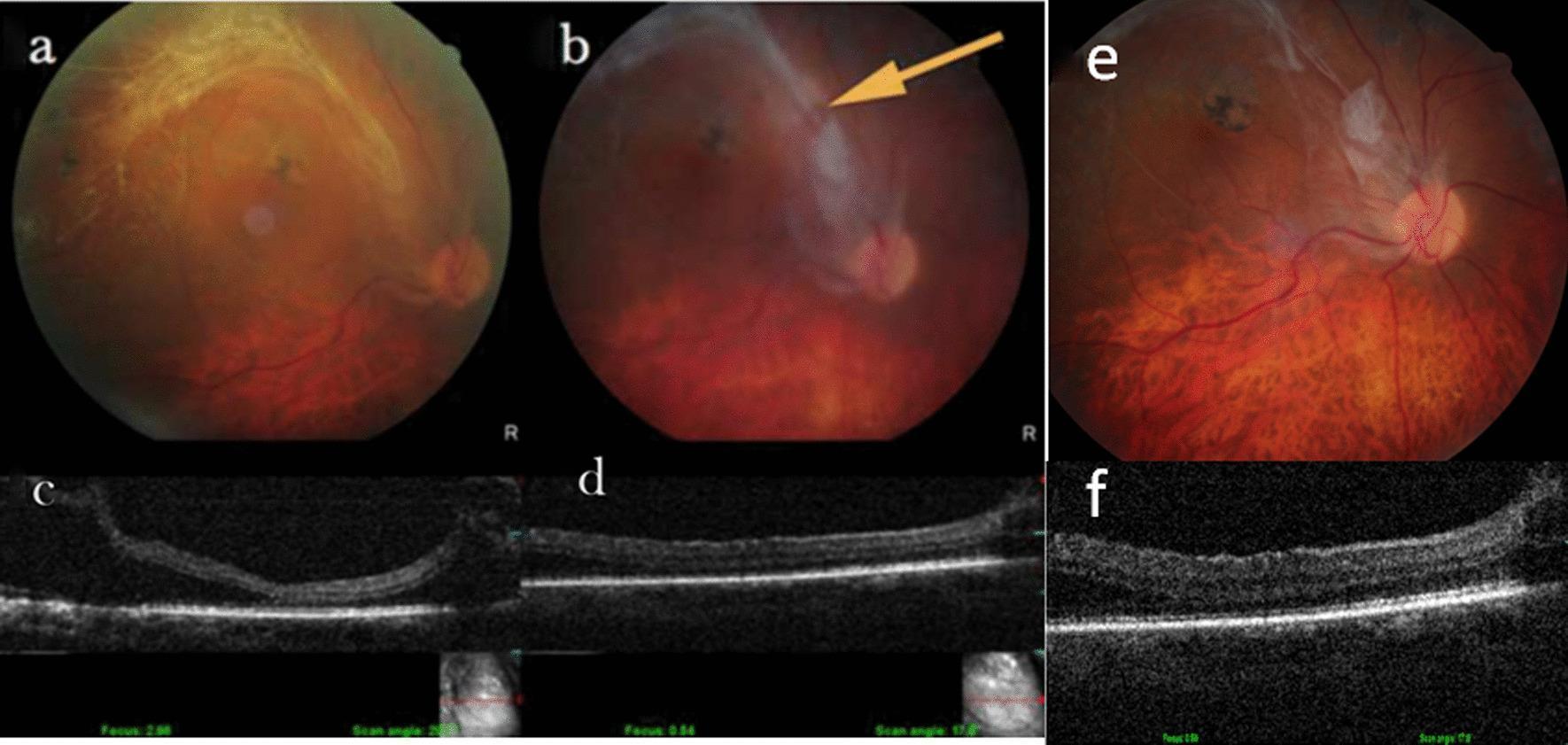
Workup
- Slit lamp examination — assess lens status, neovascularization of the iris (rubeosis), and posterior vitreous detachment (PVD)
- Indirect ophthalmoscopy with scleral depression of both eyes; slit lamp + 90D or widefield lens for peripheral breaks
- B-scan ultrasound — essential when media opacities (vitreous hemorrhage, cataract) are present
- OCT — identifies tractional membranes, differentiates membranes from detached retina, essential for evaluating macular involvement
— The Wills Eye Manual, p. 770
Management
Observation
- Extramacular TRDs (not involving the fovea) can often be observed — they tend to remain stationary for prolonged periods
- Decision depends on: etiology, fellow eye status, extent/location of traction
Surgical Indications
Surgery is indicated for:
- TRD threatening or involving the macula — treat without delay
- Combined TRD + rhegmatogenous RD — treat urgently
- Dense, non-clearing vitreous hemorrhage preventing adequate visualization or laser
- Macular epiretinal membranes or vitreomacular traction causing significant symptoms
- Severe fibrovascular proliferation unresponsive to laser/anti-VEGF
Surgical Approach: Pars Plana Vitrectomy (PPV)
- The mainstay of treatment for TRD
- Goals: remove vitreous, segment and delaminate fibrovascular membranes, relieve traction
- Combined with endolaser photocoagulation (PRP) in diabetic cases
- Intravitreal anti-VEGF agents (e.g., aflibercept, bevacizumab) may be given preoperatively (1–7 days before surgery) to reduce intraoperative bleeding from fibrovascular membranes
- DRCR.net Protocol AB: initial vitrectomy + PRP leads to faster visual recovery vs. aflibercept, with similar 2-year outcomes
— Kanski's Clinical Ophthalmology, p. 537; The Wills Eye Manual, p. 771, 815
Follow-Up
- After surgery, patients are typically seen at 1 day → 1 week → 1 month → 2–3 months → every 6–12 months
- TRD follow-up schedule depends on underlying etiology and patient factors
- Retinal specialist referral is required for all cases
Key Points to Remember
- TRD is always secondary to another process — treat the underlying cause (e.g., control DM, treat PDR with PRP)
- The characteristic concave, immobile, smooth surface distinguishes TRD from RRD
- A TRD that develops a retinal break becomes a combined TRD/RRD, which behaves differently (more bullous, requires urgent repair)
- Macular involvement is the surgical tipping point — extramacular TRDs are often observed; macular TRDs require prompt vitrectomy
- Young type 1 diabetics have more aggressive PDR and benefit from earlier intervention
ETDRS study
Finding Sources
Finding Sources
Searching PubMed
ETDRS "Early Treatment Diabetic Retinopathy Study"
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
I now have comprehensive material. Let me compile a complete answer on the ETDRS study.
ETDRS — Early Treatment Diabetic Retinopathy Study
Overview
The Early Treatment Diabetic Retinopathy Study (ETDRS) was a landmark multicenter, randomized controlled trial sponsored by the National Eye Institute (NEI), USA. It enrolled over 3,700 patients with mild-to-severe NPDR or early PDR in both eyes, randomizing them to answer two primary clinical questions:
- When should photocoagulation be initiated in diabetic retinopathy — early (before high-risk PDR develops) or deferred?
- Is aspirin effective in altering the course of diabetic retinopathy?
It also established the ETDRS classification of diabetic retinopathy and defined clinically significant macular oedema (CSMO), both of which remain in universal clinical use today.
Study Design
| Feature | Detail |
|---|---|
| Study type | Randomized controlled trial |
| Enrollment | ~3,711 patients (mild-to-severe NPDR or early PDR) |
| Eye allocation | Each eye randomized independently — one eye to early photocoagulation, fellow eye deferred |
| Aspirin arm | Patients randomized to aspirin 650 mg/day vs. placebo |
| Primary outcome | Severe visual loss (≥doubling of visual angle, e.g., 6/12 → 6/24) |
| Follow-up | Up to 9 years |
Key Findings
1. Photocoagulation Timing
| Finding | Detail |
|---|---|
| Macular laser for CSMO | Focal/grid photocoagulation reduced the risk of moderate visual loss (loss of ≥3 lines) by ~50% compared with observation |
| When to treat CSMO | Treat immediately when CSMO is present — do not defer |
| Early scatter (PRP) in severe NPDR/early PDR | Reduced risk of severe visual loss but was not uniformly beneficial at early stages — recommended to defer PRP in eyes with less than high-risk PDR, unless close follow-up is not possible |
| High-risk PDR | Prompt PRP is indicated; reduces risk of severe visual loss by >50% (building on the DRS findings) |
| Early PRP in mild-moderate NPDR | Not recommended — risks of early treatment (mild visual field loss, slight reduction in VA) outweigh benefits at this stage |
Key conclusion: "In eyes with CSMO, initiate focal photocoagulation. In eyes with high-risk PDR, initiate PRP promptly. In eyes with less severe retinopathy, careful observation is acceptable if follow-up is reliable."
2. Aspirin
- Aspirin 650 mg/day did NOT affect the progression of diabetic retinopathy — neither beneficial nor harmful on retinopathy outcomes
- Aspirin did not increase risk of vitreous hemorrhage
- Therefore: aspirin is NOT contraindicated in diabetic patients who require it for cardiovascular indications — do not withhold it to protect the eyes
3. ETDRS Classification of Diabetic Retinopathy
The ETDRS adopted the modified Airlie House classification, graded from 7-field stereoscopic fundus photographs. This is the internationally accepted grading system:
| ETDRS Category | Key Features | Risk of Progression |
|---|---|---|
| No DR | Normal | — |
| Very mild NPDR | Microaneurysms only | Low |
| Mild NPDR | MA + haemorrhages/exudates/CWS, below moderate NPDR threshold | Low–moderate |
| Moderate NPDR | Severe haemorrhages in 1–3 quadrants, OR mild IRMA, OR venous beading in ≤1 quadrant | PDR in 26%, high-risk PDR in 8% within 1 year |
| Severe NPDR | 4-2-1 rule: ≥1 of — haemorrhages in all 4Q / VB in ≥2Q / IRMA in ≥1Q | PDR in 50%, high-risk PDR in 15% within 1 year |
| Very severe NPDR | Two or more criteria of severe NPDR | PDR in 75% within 1 year |
| Early PDR | New vessels, mild | — |
| High-risk PDR | Any NV + VH/PRH; or NVD > ⅓ disc area; or NVE > ½ disc area | Immediate risk of severe visual loss |
| Advanced diabetic eye disease | TRD, persistent VH, NVG | — |
— Kanski's Clinical Ophthalmology, p. 522
4. Clinically Significant Macular Oedema (CSMO)
The ETDRS defined CSMO — still the standard clinical definition — as any one of the following:
- Retinal thickening within 500 μm (≈ ⅓ disc diameter) of the centre of the macula
- Hard exudates within 500 μm of the centre with adjacent retinal thickening (the thickening itself may extend beyond 500 μm)
- Retinal thickening ≥1 disc area, any part of which is within 1 disc diameter of the centre of the macula
CSMO is an indication for focal/grid laser photocoagulation, regardless of the level of visual acuity. (In contemporary practice, centre-involving CSMO is preferentially treated with anti-VEGF agents — DRCR.net Protocol I and T.)
— Kanski's Clinical Ophthalmology, p. 525
The 4-2-1 Rule (Severe NPDR) — ETDRS Derived
An easy mnemonic for severe NPDR (any one criterion present):
- 4 quadrants with severe intraretinal haemorrhages
- 2 quadrants with venous beading
- 1 quadrant with IRMA
Two or more = very severe NPDR.
ETDRS Visual Acuity Chart
A secondary legacy of the ETDRS is the standardized logMAR visual acuity chart used in clinical trials:
- Uses Sloan optotypes on a 5×5 grid
- Balanced rows: each row has equivalent legibility across letters
- Calibrated for 4 metres
- 5 letters per row; each letter = 1 logMAR unit ÷ 5 = 0.02 logMAR per letter
- Allows more precise measurement than Snellen charts — preferred for clinical trials
— Kanski's Clinical Ophthalmology, p. 18
Clinical Impact & Legacy
| Contribution | Impact |
|---|---|
| CSMO definition | Universal — still the benchmark for treatment threshold |
| DR classification | Modified Airlie House (ETDRS) grading adopted worldwide |
| Macular laser technique | Defined focal/grid laser parameters for 30+ years |
| Aspirin safety | Confirmed aspirin can be used safely in DR patients needing it |
| Timing of PRP | Established the principle: treat high-risk PDR promptly, observe early disease with reliable follow-up |
| logMAR chart | ETDRS chart became the gold standard for VA measurement in research |
The ETDRS, together with the Diabetic Retinopathy Study (DRS) for PRP and the subsequent DRCR.net protocols, forms the evidence foundation of diabetic eye disease management. Contemporary practice has evolved beyond the ETDRS macular laser findings with anti-VEGF therapy (Protocol I, T), but the ETDRS classification, CSMO definition, and aspirin conclusions remain foundational.
Excudative retinal detachment 10 marks
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Searching Images
exudative serous retinal detachment shifting fluid fundus
Loading Image
Loading Image
Loading Image
I now have all material needed for a complete 10-mark answer. Here it is:
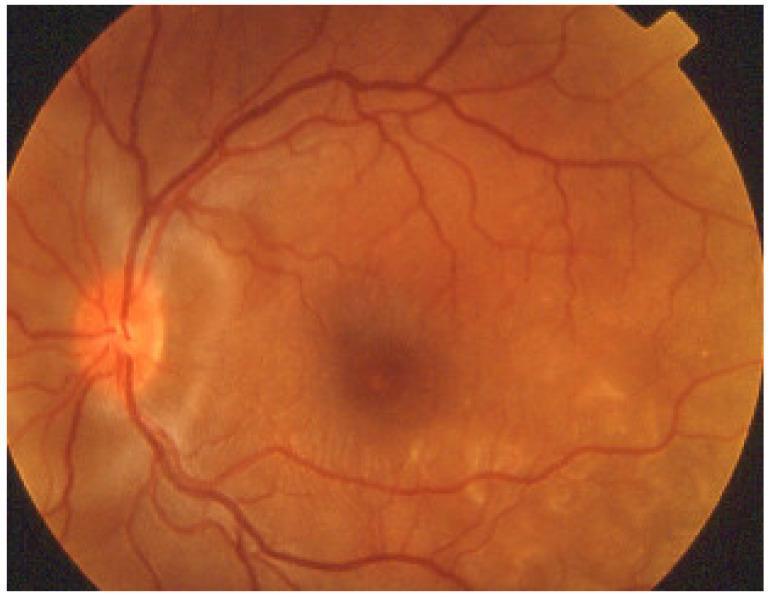
Exudative (Serous) Retinal Detachment — 10 Marks
Definition
Exudative retinal detachment (ERD), also called serous RD, is the separation of the neurosensory retina from the retinal pigment epithelium (RPE) by subretinal fluid (SRF) that accumulates in the absence of a retinal break or vitreoretinal traction. It occurs when fluid leaks from the choroidal or retinal vasculature and overwhelms the RPE's active fluid-pumping capacity.
Pathogenesis
The RPE normally maintains adhesion of the neurosensory retina by actively pumping fluid from the subretinal space into the choroidal circulation (outer blood-retinal barrier). ERD occurs when:
- Breakdown of the outer blood-retinal barrier (RPE or choriocapillaris) → excessive fluid leakage into the subretinal space
- RPE pumping overwhelmed by inflammatory, neoplastic, or vascular processes
- Choroidal venous outflow obstruction (e.g., nanophthalmos, uveal effusion syndrome)
As long as fluid leaks faster than the RPE can remove it, SRF accumulates and the retina detaches. Because there is no vitreoretinal traction, the detachment is freely mobile — this produces the pathognomonic shifting fluid sign.
— Kanski's Clinical Ophthalmology, p. 706
Aetiology / Causes
Neoplastic
- Choroidal malignant melanoma (most important — must be excluded first)
- Choroidal metastases (breast, lung most common)
- Choroidal haemangioma (circumscribed or diffuse)
- Retinal capillary haemangioblastoma
- Multiple myeloma
Key rule: An intraocular tumour should be considered the cause of an exudative RD until proved otherwise. — Kanski's
Inflammatory
- Vogt-Koyanagi-Harada (VKH) syndrome — multifocal bilateral exudative RD
- Posterior scleritis — serous macular detachment
- Sympathetic ophthalmia
- Other posterior uveitis
Vascular
- Choroidal neovascularization (CNV / wet AMD)
- Coats disease — massive lipid exudation
- Malignant hypertension / hypertensive choroidopathy
- Pre-eclampsia / toxaemia of pregnancy
- Familial exudative vitreoretinopathy (FEVR)
Idiopathic / Structural
- Bullous central serous chorioretinopathy (CSCR) — rare, more often pigment epithelial detachment
- Uveal effusion syndrome — bilateral, associated with nanophthalmos/high hyperopia; dilated episcleral vessels; leopard-spot RPE changes
- Congenital: optic pit, morning glory syndrome, choroidal coloboma
Iatrogenic
- Post-retinal detachment surgery
- Post-panretinal photocoagulation
— The Wills Eye Manual, p. 768–769; Kanski's, p. 706–707
Clinical Features
Symptoms
- Visual field defect — varies with head position (pathognomonic feature)
- Visual loss — variable severity
- Visual changes shift with posture (inferior field loss when upright → posterior field/macular when supine)
- No photopsia — because there is no vitreoretinal traction
- Floaters if there is associated vitritis
- May be bilateral depending on cause (e.g., VKH, malignant HTN)
Signs
| Feature | Description |
|---|---|
| Configuration | Convex (dome-shaped), similar to RRD |
| Surface | Smooth (not corrugated) |
| Mobility | Very mobile — shifts with gravity |
| Shifting fluid | ✅ Pathognomonic: SRF pools inferiorly when upright; shifts posteriorly/superiorly when supine |
| Extent | Rarely extends to ora serrata |
| Retinal break | ❌ Absent |
| Vitreous | Pigment cells absent; may have vitritis if inflammatory |
| RAPD | Mild, in large detachments |
| 'Leopard spots' | Scattered subretinal pigment clumping seen after detachment resolves |
Differential Diagnosis
| Feature | Exudative RD | Rhegmatogenous RD | Traction RD |
|---|---|---|---|
| Break | ❌ | ✅ | ❌ |
| Traction | ❌ | ❌ (PVD only) | ✅ |
| Shape | Convex, smooth | Convex, corrugated | Concave, smooth |
| Mobility | ✅ Very mobile | Mobile | ❌ Immobile |
| Shifting fluid | ✅ | ❌ | ❌ |
| Pigment in vitreous | ❌ | ✅ (Shafer's sign) | ❌ |
| Photopsia | ❌ | ✅ | ❌/mild |
| Extends to ora serrata | Rarely | Usually | Rarely |
Investigations / Workup
- Fundus examination — indirect ophthalmoscopy; scleral depression to rule out hidden break
- B-scan ultrasonography — identify underlying choroidal tumour, posterior scleritis ("T-sign" of fluid in Tenon's capsule), choroidal thickness; assess shifting fluid
- Intravenous fluorescein angiography (IVFA) — demonstrates pooling of dye in subretinal space (smokestack/inkblot pattern in CSCR); identifies leakage source; highlights CNV
- OCT — confirms subretinal fluid; identifies CNV, pigment epithelial detachments; quantifies extent
- Indocyanine green angiography (ICGA) — hypofluorescent spots in VKH; choroidal polyps in PCV; choroidal tumour vasculature
- Systemic workup — blood pressure, renal function, FBC; imaging for primary malignancy (chest X-ray/CT); inflammatory markers (ESR, CRP); skin/hair/neurological exam (VKH)
Treatment
Treatment is directed at the underlying cause — ERD has no primary surgical treatment.
| Cause | Treatment |
|---|---|
| Choroidal melanoma | Brachytherapy / proton beam / enucleation |
| Choroidal metastasis | Radiotherapy ± systemic chemotherapy |
| VKH / Posterior scleritis | Systemic corticosteroids (oral prednisolone); immunosuppression for refractory cases |
| Choroidal haemangioma | PDT (photodynamic therapy) / low-dose radiotherapy |
| Coats disease | Laser photocoagulation / cryotherapy to telangiectasia ± anti-VEGF |
| Wet AMD / CNV | Intravitreal anti-VEGF (aflibercept, ranibizumab, bevacizumab) |
| Bullous CSCR | PDT / laser to leaking RPE point; stop exogenous corticosteroids |
| Malignant HTN | Controlled blood pressure reduction |
| Uveal effusion syndrome | Sclerectomy / sclerotomy in nanophthalmos |
| Iatrogenic (post-PRP) | Observation — usually self-limiting |
Some cases (e.g., VKH, posterior scleritis) resolve completely with systemic steroids. Others (neoplastic) require specific oncological treatment. The prognosis depends entirely on the underlying aetiology and promptness of treatment.
— The Wills Eye Manual, p. 769–771; Kanski's Clinical Ophthalmology, p. 707
Key Points for Exam
- No break, no traction — defines exudative RD
- Shifting fluid is pathognomonic
- Smooth, convex, very mobile retina
- Tumour must be excluded first — especially choroidal melanoma
- No photopsia — distinguishes from RRD
- Treatment = treat the cause; surgery has no primary role
- Leopard spots after resolution indicate prior exudative RD (e.g., VKH, uveal effusion)
This is a shared conversation. Sign in to Orris to start your own chat.