Monthly period cycle disturb in identify investigation
Reading File
Finding Sources
Searching PubMed
"menstrual irregularity" AND "diagnosis"
Searching the Web
menstrual cycle disturbance investigation causes workup 2025
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a thorough, structured overview of menstrual cycle disturbances - identification and investigation.
Menstrual Cycle Disturbances: Identification and Investigation
Normal Cycle - Reference Point
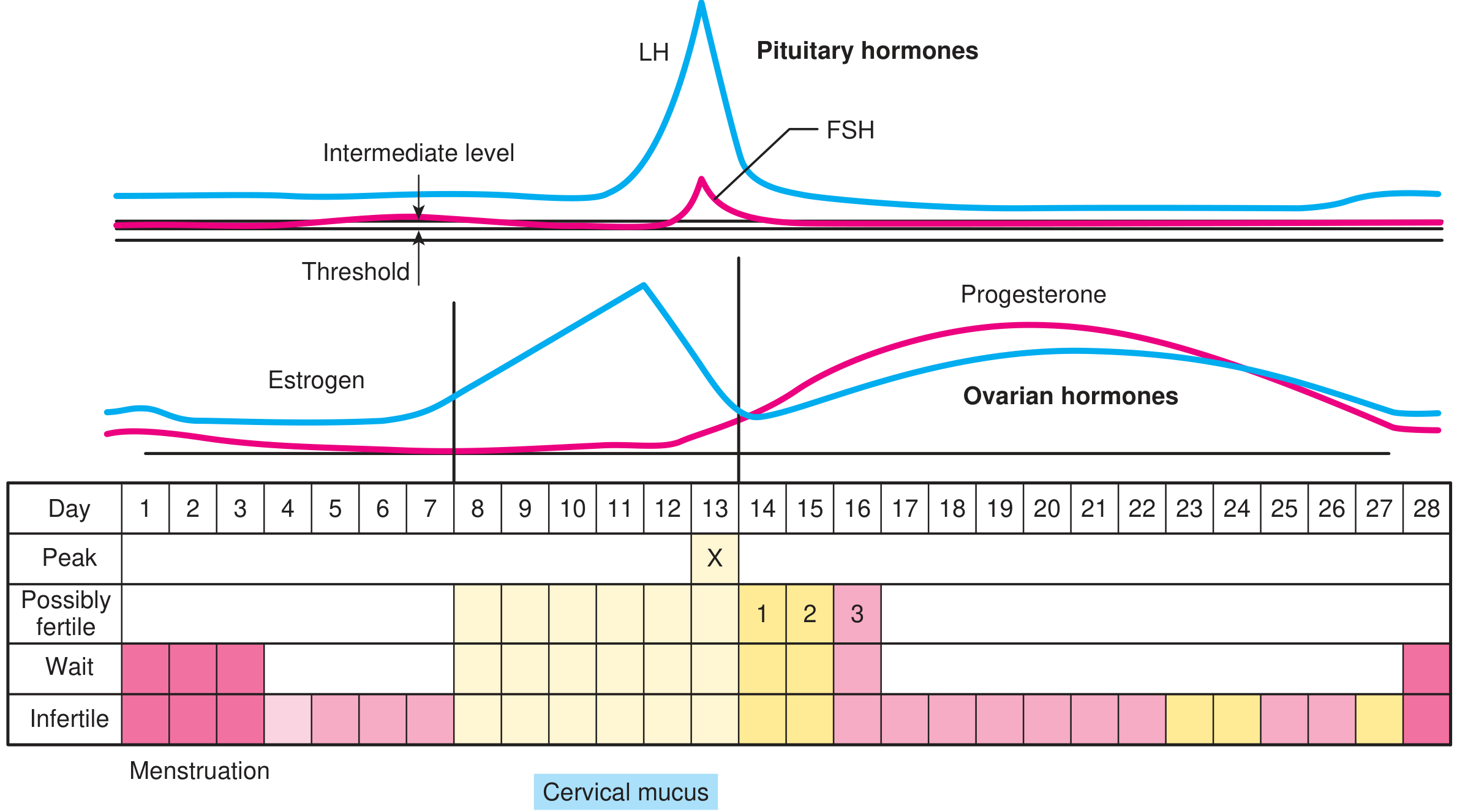
A normal menstrual cycle is 21-35 days long, with bleeding lasting 2-7 days and blood loss of 20-80 mL. Ovulation normally occurs around day 14 in a 28-day cycle. The hormonal interplay is shown below:
Classification of Menstrual Disturbances
| Term | Definition |
|---|---|
| Primary amenorrhea | No menses by age 15 with secondary sexual characteristics, or age 13 without |
| Secondary amenorrhea | Absence of menses for 3 cycles or 3 months in a previously menstruating woman |
| Oligomenorrhea | Fewer than 9 cycles/year, or cycle length >35 days |
| Menorrhagia | Heavy or prolonged menstrual bleeding |
| Dysmenorrhea | Painful menstruation |
| Metrorrhagia | Irregular bleeding between periods |
A woman with regular cycles and even a week's delay warrants a pregnancy test. Evaluation is advisable if a woman has fewer than 9 cycles per year or cycle length longer than 35 days. (Berek & Novak's Gynecology)
WHO Classification of Amenorrhea
The World Health Organization classifies amenorrhea into three groups, plus a fourth added later:
- WHO Group I - Hypogonadotropic hypogonadism: no endogenous estrogen, normal/low FSH, normal prolactin, no hypothalamic-pituitary lesion
- WHO Group II - Normogonadotropic anovulation (e.g. PCOS): evidence of estrogen production, normal FSH and prolactin
- WHO Group III - Hypergonadotropic hypogonadism: elevated FSH indicating gonadal failure (e.g. premature ovarian insufficiency)
- WHO Group IV (added later) - Hyperprolactinemic anovulation: anovulation due specifically to elevated prolactin
(Berek & Novak's Gynecology, Tietz Textbook of Laboratory Medicine 7e)
Common Causes
Hypothalamic / Functional
- Excessive exercise, stress, nutritional disorders, weight loss
- Hypothalamic tumors or infiltrative disease
- Functional hypothalamic amenorrhea (HPO axis suppression)
Pituitary
- Hyperprolactinemia (prolactinoma, drug-induced) - presents with galactorrhea + oligomenorrhea/amenorrhea
- Sheehan syndrome (postpartum pituitary necrosis)
- Pituitary apoplexy, empty sella syndrome
- Acquired hypopituitarism (trauma, tumor)
Ovarian
- PCOS (most common cause of oligomenorrhea) - hyperandrogenism + oligo/amenorrhea + polycystic ovaries (Rotterdam criteria: 2 of 3 required)
- Premature Ovarian Insufficiency (POI) - ovarian failure before age 40, hypergonadotropic state
- Gonadal dysgenesis (Turner syndrome 45,X - most common in primary amenorrhea)
- Autoimmune oophoritis
Uterine / Outflow Tract
- Asherman syndrome - intrauterine adhesions from D&C or infection; normal hormones but no bleeding
- Endometrial damage, cervical stenosis
Endocrine / Systemic
- Thyroid disease (hypothyroidism or hyperthyroidism)
- Congenital adrenal hyperplasia (21-hydroxylase deficiency most common)
- Cushing syndrome
- Chronic disease, cancer
Drugs / Iatrogenic
- Antipsychotics (phenothiazines, haloperidol, clozapine) - cause hyperprolactinemia
- Antidepressants (tricyclics, MAOIs)
- Antihypertensives (methyldopa, calcium channel blockers, reserpine)
- Drugs with estrogenic activity (digitalis, marijuana, oral contraceptives)
- Cytotoxic chemotherapy (busulfan, cyclophosphamide, cisplatin)
Physiological
- Pregnancy (most common cause of secondary amenorrhea)
- Lactation
- Perimenopause
Investigation Algorithm
Step 1: History
- Complete menstrual history (age at menarche, cycle regularity, flow, pain)
- Galactorrhea, hot flashes, hirsutism, acne
- Symptoms of hypothyroidism
- Weight changes, exercise habits, nutritional status, stress
- Prior pelvic surgery or trauma, infections (PID)
- Current medications
- Contraceptive history
Step 2: Physical Examination
- BMI, weight, signs of androgen excess (hirsutism, acne, virilization)
- Thyroid palpation
- Breast examination (galactorrhea)
- Visual fields (pituitary tumor may cause bitemporal hemianopia)
- Pelvic examination (uterus, ovaries, outflow tract)
- Secondary sexual characteristics (absent in Turner syndrome)
Step 3: First-Line Laboratory Tests
| Test | What it detects |
|---|---|
| Urine/serum hCG | Pregnancy (always first) |
| FSH + LH | Ovarian reserve; elevated = ovarian failure; low/normal = hypothalamic/pituitary cause |
| Prolactin | Hyperprolactinemia (prolactinoma, drug-induced) |
| TSH | Thyroid dysfunction |
| Total testosterone + androstenedione | Hyperandrogenism (PCOS, adrenal, tumor) |
| DHEA-S | Adrenal androgen excess; very high = adrenal tumor |
| 17-hydroxyprogesterone | Congenital adrenal hyperplasia (21-hydroxylase deficiency) |
| AMH (Anti-Mullerian Hormone) | Ovarian reserve; elevated in PCOS, very low in POI |
Note on androgen testing: Androstenedione has better sensitivity (88.3%) and specificity (97.7%) for detecting androgen excess in PCOS than testosterone alone. Liquid chromatography-tandem mass spectrometry (LC-MS/MS) is preferred over immunoassay for androgen measurement in women due to the low concentrations involved. (Tietz Textbook of Laboratory Medicine 7e)
Note on PCOS diagnosis: Serum AMH >35 pmol/L (5 ng/mL) has been proposed as a surrogate for polycystic ovarian morphology, but the 2018 International PCOS Network recommends against using AMH alone as a standalone diagnostic test. (Tietz Textbook of Laboratory Medicine 7e)
Step 4: Imaging
- Pelvic ultrasound - uterine structure, endometrial thickness, ovarian morphology (polycystic ovaries), follicle count
- MRI pituitary - if prolactin elevated or pituitary tumor suspected
Step 5: Additional / Targeted Tests
| Situation | Additional test |
|---|---|
| Elevated FSH, age <25 or short stature | Karyotype / chromosomal microarray (rule out Turner syndrome, Y chromosome) |
| Elevated FSH, POI | FMR1 premutation screening (fragile X) |
| Elevated FSH, POI | Autoimmune antibodies (adrenal, thyroid, ovarian) |
| Suspected Asherman syndrome | Hysteroscopy or sonohysterogram |
| Virilization | DHEA-S, pelvic/adrenal imaging (rule out tumor) |
| Suspected CAH | 17-hydroxyprogesterone, ACTH stimulation test |
| Cushing suspected | 24-hour urinary free cortisol, dexamethasone suppression |
Key Diagnostic Points
- Pregnancy must always be excluded first before any other workup.
- Oligomenorrhea etiologies largely overlap with amenorrhea; the distinction between primary and secondary amenorrhea should not be overemphasized clinically. (Berek & Novak's Gynecology)
- In PCOS, the LH:FSH ratio is often elevated, but this ratio should not be used as a routine diagnostic test.
- Women with POI younger than 25 or shorter than 5 feet should have karyotyping to rule out chromosomal abnormalities, including a Y chromosome (gonadoblastoma risk).
- Asherman syndrome presents with normal hormones but absent menses - the outflow tract is structurally blocked.
Sources: Berek & Novak's Gynecology; Tietz Textbook of Laboratory Medicine 7e; Textbook of Family Medicine 9e; Goldman-Cecil Medicine.
This is a shared conversation. Sign in to Orris to start your own chat.