A patient presented with loose stools since past 4 day and has no history of fever and HTN , DM OR THYROid and no surgical and family history
Reading File
Finding Sources
Finding Sources
Searching the Web
acute diarrhea loose stools management clinical approach 2024
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive information to give a thorough clinical answer. Here is the full structured response:
Clinical Assessment: Acute Loose Stools (4 Days)
Patient Summary: Adult with loose stools x 4 days, no fever, no HTN/DM/thyroid disease, no surgical or family history.
This presentation is consistent with acute diarrhea - defined as <4 weeks duration. With no fever, no blood in stool, no immunocompromise, and no co-morbidities, this most likely represents mild-to-moderate non-inflammatory (secretory/osmotic) infectious diarrhea, most commonly viral gastroenteritis or a food-related bacterial toxin.
Step 1: History to Clarify Etiology
Ask specifically about:
| Feature | Significance |
|---|---|
| Stool frequency / consistency | Severity assessment |
| Presence of blood or mucus | Suggests invasive (inflammatory) diarrhea - Shigella, Salmonella, Campylobacter, E. coli O157, Entamoeba |
| Nausea / vomiting | Suggests upper GI source (viral, S. aureus toxin, B. cereus) |
| Recent travel | Traveler's diarrhea - ETEC, Campylobacter |
| Recent antibiotic use | C. difficile |
| Food history (picnic, restaurant, seafood, undercooked meat, dairy) | Specific foodborne pathogens |
| Recent sick contacts | Viral outbreak |
| Abdominal pain/cramps | Character and location |
| Signs of dehydration (thirst, decreased urine, dizziness) | Guides rehydration urgency |
Step 2: Physical Examination
- Vitals: BP, HR, temperature, respiratory rate
- Hydration status: Skin turgor, mucous membranes, capillary refill, urine output
- Abdomen: Tenderness (diffuse vs localized), bowel sounds, signs of peritonism
- Signs of systemic infection: Lymphadenopathy, jaundice
Step 3: Severity Assessment
This patient's presentation (no fever) suggests mild disease based on the Harrison's algorithm:
- Mild: Normal activity, no dehydration - observe and treat symptomatically
- Moderate: Some activity limitation, mild dehydration - ORS + antidiarrheal agents
- Severe: Incapacitated, significant dehydration - IV fluids + stool workup
Step 4: Investigations
In this patient (no fever, no blood, no red flags), investigations are NOT immediately required.
Indications to order stool studies would include:
- Fever ≥38.5°C
- Overtly bloody stools
- Duration >48 h without improvement (this patient is at day 4 - borderline)
- Recent antibiotic use
- Immunocompromise
- Age >70 years
- Severe dehydration
If workup is needed, order:
- Stool culture / multiplex PCR (for bacteria, parasites, viruses)
- Stool for ova & parasites (if travel history, prolonged course)
- Stool C. difficile toxin (if recent antibiotics)
- CBC, electrolytes, renal function (if dehydrated)
Step 5: Management
This patient's presentation warrants symptomatic treatment:
A. Rehydration (Most Important)
- Oral Rehydration Solution (ORS) - the cornerstone of treatment
- WHO-ORS or sport drinks (iso-osmolar)
- Encourage fluids: water, dilute juices, rice water, coconut water
- Avoid: milk (transient lactase deficiency), caffeinated drinks, alcohol
- IV fluids (Normal Saline or Ringer's Lactate) only if unable to tolerate oral intake or profoundly dehydrated
B. Diet
- BRAT diet (Banana, Rice, Applesauce, Toast) initially
- Avoid fatty, spicy, high-fiber, or lactose-containing foods
- Resume normal diet gradually as tolerated
C. Antidiarrheal Agents (for moderate non-febrile, non-bloody diarrhea)
- Loperamide (Imodium): 4 mg initially, then 2 mg after each loose stool (max 16 mg/day)
- Avoid if fever or bloody stool (can prolong febrile dysentery)
- Bismuth subsalicylate: reduces stool frequency and nausea
- Avoid in renal impairment
D. Probiotics
- Lactobacillus and Saccharomyces boulardii - modest evidence for reducing duration
- Reasonable adjunct in acute infectious diarrhea
E. Antibiotics - NOT routinely indicated in this case
- No fever, no blood, no travel, not immunocompromised
- If empirical treatment is considered (febrile dysentery or traveler's diarrhea):
- Azithromycin 500 mg single dose, OR
- Ciprofloxacin 500 mg twice daily x 3-5 days
- For suspected Giardia: Metronidazole 250 mg four times daily x 7 days
Step 6: Red Flags - When to Escalate
Reassess if the patient develops:
- Fever (especially >38.5°C)
- Blood or mucus in stools
- Severe abdominal pain
- Signs of significant dehydration (sunken eyes, no urine output, altered consciousness)
- No improvement after 5-7 days - consider chronic causes
Differential Diagnosis to Keep in Mind
| Category | Examples |
|---|---|
| Viral (most common) | Norovirus, Rotavirus, Adenovirus |
| Bacterial (toxin-mediated) | S. aureus, B. cereus, C. perfringens |
| Bacterial (invasive) | Salmonella, Shigella, Campylobacter |
| Parasitic | Giardia lamblia, Entamoeba histolytica |
| Food intolerance | Lactose intolerance, FODMAP sensitivity |
| Drug-related | Recent NSAIDs, antibiotics, laxatives |
| Early IBD | Crohn's, Ulcerative Colitis (less likely at 4 days) |
Management Algorithm (from Harrison's 22nd Ed.)
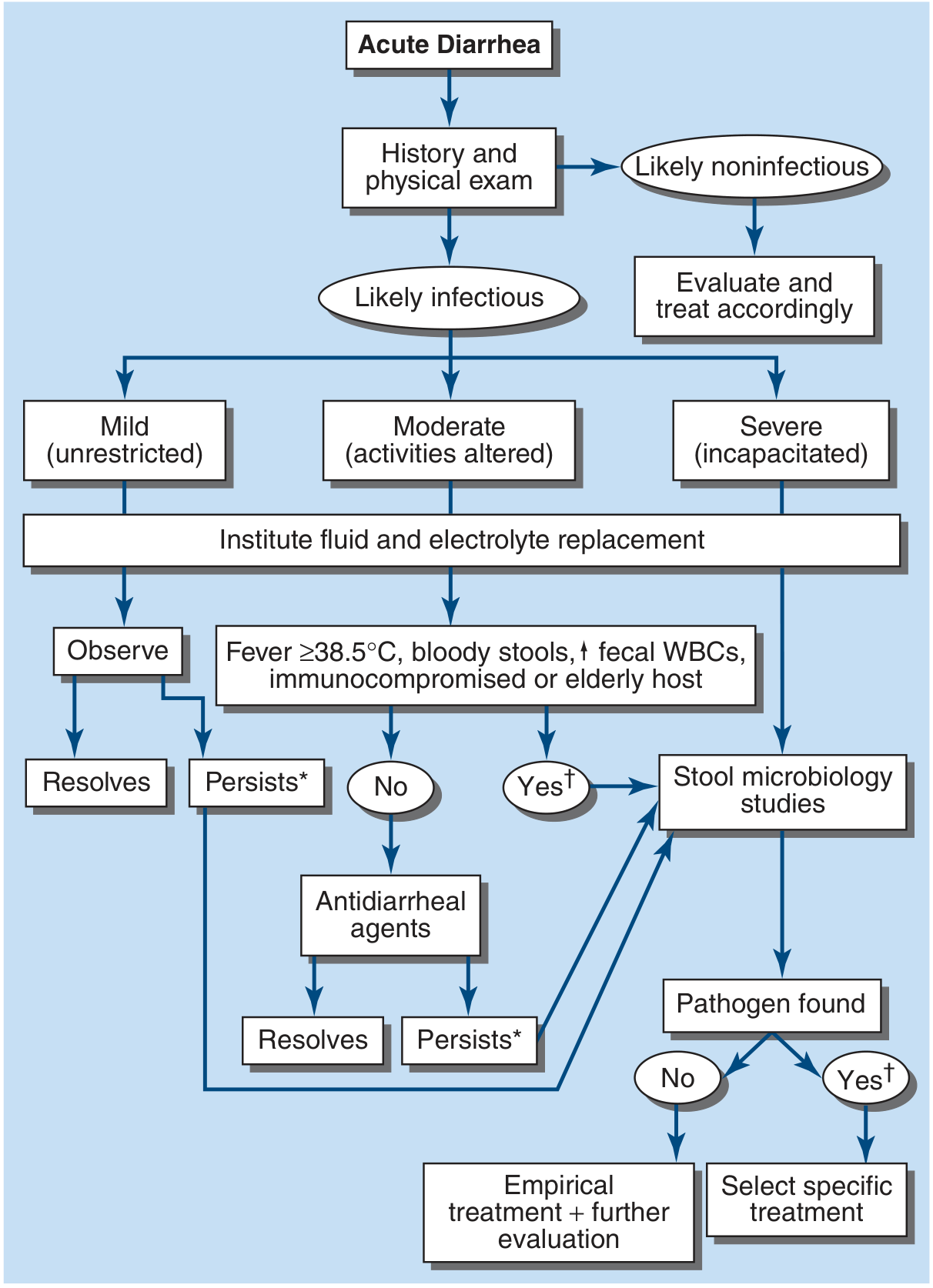
Note: * = Consider empirical metronidazole; † = Consider empirical quinolone
Summary Plan for This Patient
- ORS - encourage oral fluids aggressively
- BRAT diet - bland, low-fiber foods
- Loperamide 4 mg stat, then 2 mg after each unformed stool (since no fever/blood)
- Monitor for red flags - return if fever, blood in stools, or worsening dehydration
- Stool studies only if no improvement in 48-72 h or new alarm features develop
- No antibiotics at this stage
Since the patient is at day 4 with no alarm features, this is likely self-limiting and should resolve within 5-7 days total.
- Harrison's Principles of Internal Medicine 22E, pp. 349-350 (Acute Diarrhea - Approach & Treatment)
- Sleisenger and Fordtran's Gastrointestinal and Liver Disease (Causes of Acute Diarrhea)
This is a shared conversation. Sign in to Orris to start your own chat.