Pharmacodynamics
Reading File
Asking for Preferences
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Here is a complete, exam-ready overview of Pharmacodynamics, sourced from Lippincott Illustrated Reviews: Pharmacology.
Pharmacodynamics - Exam-Ready Overview
Definition: Pharmacodynamics describes the actions of a drug on the body - what the drug does, and how it does it. (Compare with pharmacokinetics = what the body does to the drug.)
1. Drug-Receptor Basics
Most drugs exert effects by binding to specialized macromolecules called receptors on or inside cells. This binding triggers signal transduction - a cascade of biochemical events that produces the drug's effect.
Key concept: Affinity = the strength with which a drug binds to its receptor (measured by the dissociation constant, Kd). The lower the Kd, the higher the affinity.
Receptor Types & Signal Transduction Mechanisms
| Receptor Type | Mechanism | Speed | Examples |
|---|---|---|---|
| Ligand-gated ion channels (Type I) | Ion flux across membrane | Fastest (milliseconds) | Nicotinic ACh receptor, GABA-A |
| G protein-coupled receptors (Type II) | Activate second messengers (cAMP, IP3/DAG, cGMP) | Seconds-minutes | Adrenergic, muscarinic, opioid |
| Receptor tyrosine kinases (Type III) | Autophosphorylation of tyrosine residues | Minutes-hours | Insulin receptor, growth factors |
| Nuclear receptors / Intracellular (Type IV) | Alter gene transcription | Hours-days (slowest) | Steroid hormones, thyroid hormone |
Second Messengers (high-yield):
- Gs (stimulatory) → adenylyl cyclase ↑ → cAMP ↑ → PKA activated (e.g., β-adrenergic)
- Gi (inhibitory) → adenylyl cyclase ↓ → cAMP ↓ (e.g., M2 muscarinic, opioid)
- Gq → phospholipase C → IP3 + DAG → Ca²⁺ release + PKC (e.g., α1-adrenergic, M1/M3)
2. Dose-Response Relationships
As drug concentration increases, pharmacologic effect increases until all receptors are occupied (maximum effect = Emax).
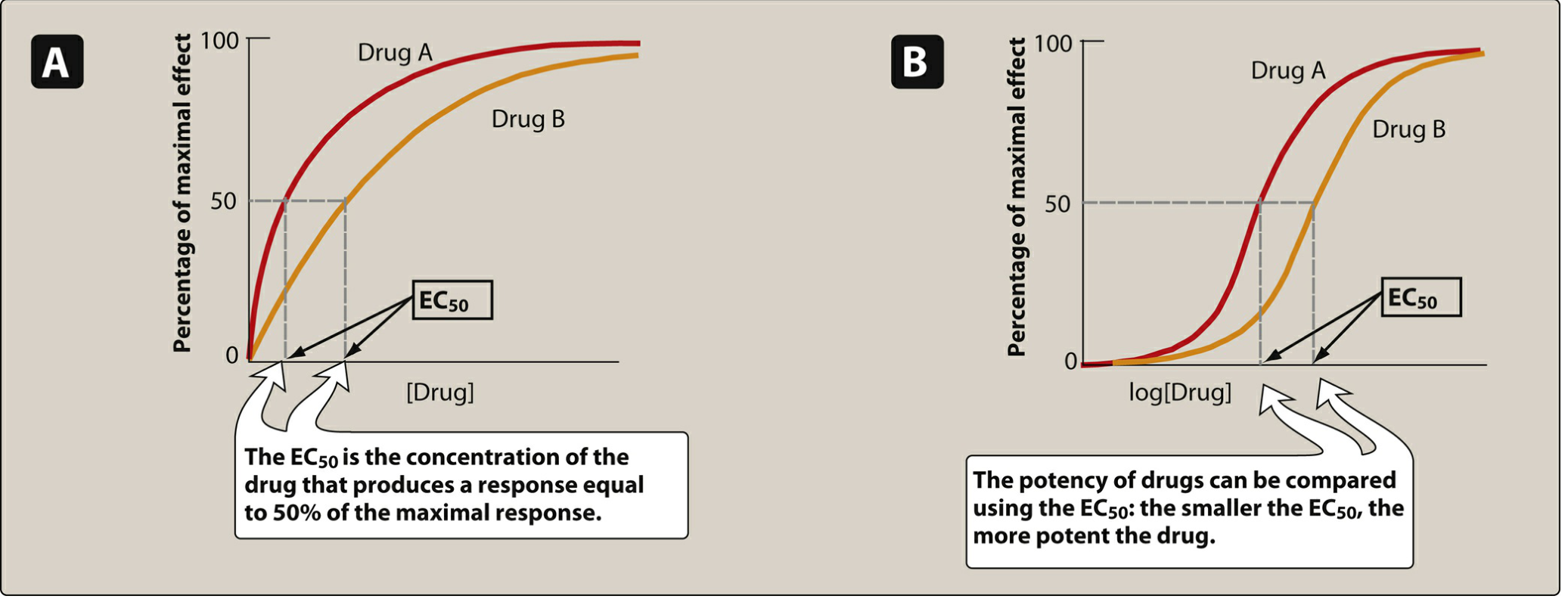
Potency vs. Efficacy
| Parameter | Definition | Measured By | Key Point |
|---|---|---|---|
| Potency | Amount of drug needed to produce an effect | EC50 (lower = more potent) | Clinically less important than efficacy |
| Efficacy | Maximum effect a drug can produce | Emax | More clinically important |
- Drug A is more potent than Drug B if Drug A has a lower EC50 (its curve is shifted left)
- Two drugs can have equal efficacy (same Emax) but different potency
Therapeutic Index (TI)
$$TI = \frac{TD_{50}}{ED_{50}}$$
- Wide TI = safer drug (e.g., penicillin)
- Narrow TI = careful dosing required (e.g., warfarin, digoxin, lithium, aminoglycosides)
3. Agonists, Partial Agonists & Antagonists

Types of Drug Activity (Intrinsic Activity)
| Type | Intrinsic Activity | Effect | Example |
|---|---|---|---|
| Full agonist | = 1 | Binds and produces maximal response (same Emax as endogenous ligand) | Morphine (opioid), phenylephrine (α1) |
| Partial agonist | 0 < IA < 1 | Produces sub-maximal response even at 100% receptor occupancy; can act as partial antagonist in the presence of a full agonist | Buprenorphine (opioid), buspirone (5-HT1A) |
| Inverse agonist | < 0 | Produces effect below baseline (reduces constitutive activity) | Some benzodiazepines in certain contexts |
| Competitive antagonist | 0 | Binds reversibly; shifts dose-response curve to the right (↑ EC50); Emax unchanged | Naloxone, atropine, propranolol |
| Non-competitive (irreversible) antagonist | 0 | Binds permanently; ↓ Emax (Emax is reduced); EC50 may not change | Phenoxybenzamine (α-blocker) |
Key exam pearl: Competitive antagonism is surmountable (increasing agonist dose can overcome it). Non-competitive is insurmountable (Emax can never recover).
4. Receptor Regulation
Downregulation (Desensitization)
- Caused by prolonged agonist exposure
- Receptors are phosphorylated → rendered unresponsive
- Receptors may be internalized (removed from cell surface)
- Clinical example: Opioid tolerance - repeated morphine use decreases opioid receptor number and responsiveness, requiring higher doses for same pain relief
Upregulation
- Caused by prolonged antagonist exposure
- More receptors are inserted into the membrane
- Cells become hypersensitive to agonists
- Clinical example: Rebound hypertension when β-blockers are stopped abruptly (upregulated β-receptors → exaggerated catecholamine response)
Tachyphylaxis
- Rapidly developing tolerance after just a few doses (e.g., repeated use of indirect-acting sympathomimetics like amphetamine depletes norepinephrine stores)
5. Drug Interactions (Pharmacodynamic)
| Type | Mechanism | Result | Example |
|---|---|---|---|
| Synergism / Additivity | Both drugs act on same pathway | Effect ≥ sum of individual effects | Alcohol + benzodiazepines (CNS depression) |
| Potentiation | One drug enhances another's effect without having the effect itself | Enhanced effect | Probenecid + penicillin |
| Antagonism | Opposing actions at same or different receptors | Reduced net effect | Naloxone reversing morphine overdose |
6. Special Populations - Altered Pharmacodynamics
- Elderly patients: Decreased β-receptor sensitivity to both agonists and antagonists; increased CNS sensitivity to benzodiazepines and opioids (receptor changes); increased risk of anticholinergic toxicity (↓ ACh synthesis); greater warfarin-induced vitamin K inhibition at same plasma levels
- Calcium channel blockers cause greater BP and HR drops in elderly due to diminished homeostatic reserve
High-Yield Summary Table
| Concept | Key Value/Definition |
|---|---|
| EC50 | Concentration causing 50% maximal effect; measures potency |
| Emax | Maximum effect achievable; measures efficacy |
| Kd | Dissociation constant; inversely related to affinity |
| Full agonist | Intrinsic activity = 1, same Emax as endogenous ligand |
| Partial agonist | Intrinsic activity < 1, can antagonize full agonist |
| Competitive antagonist | Shifts curve right, Emax preserved |
| Non-competitive antagonist | Decreases Emax, curve does not recover with more agonist |
| Downregulation | Prolonged agonist → fewer receptors, tolerance |
| Upregulation | Prolonged antagonist → more receptors, rebound effect |
| Narrow TI drugs | Warfarin, digoxin, lithium, aminoglycosides, phenytoin |
Source: Lippincott Illustrated Reviews: Pharmacology, Chapter 2 - Drug-Receptor Interactions and Pharmacodynamics
This is a shared conversation. Sign in to Orris to start your own chat.