Ctg
Asking for Preferences
Goiter
Reading File
Finding Sources
Searching PubMed
goiter thyroid enlargement
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Here is a thorough overview of Goiter drawn from multiple authoritative medical textbooks.
Goiter
Definition
A goiter is any enlargement of the thyroid gland. In common clinical usage the term most often refers to benign causes - diffuse toxic goiter (Graves' disease), toxic multinodular goiter, or nontoxic multinodular goiter. Malignant thyroid enlargement is usually called a mass or nodule rather than a goiter.
- Goldman-Cecil Medicine, p. 3271
- Current Surgical Therapy 14e, p. 880
Types
| Type | Description |
|---|---|
| Diffuse goiter | Uniform gland enlargement; almost always benign; seen in Graves' disease and congenital hormone synthesis defects |
| Multinodular goiter (MNG) | Multiple nodules, solid or partially cystic (colloid cysts), with areas of fibrosis; may be toxic (hyperthyroid) or nontoxic (euthyroid) |
| Endemic goiter | Occurs in geographic regions of iodine deficiency |
| Retrosternal / intrathoracic goiter | Extension into the chest; can cause superior vena cava syndrome or anterior mediastinal mass |
Causes / Pathogenesis
The most common cause worldwide is iodine deficiency. The pituitary responds to low thyroid hormone by increasing TSH secretion, which drives thyroid enlargement. Other causes include:
- Goitrogens (dietary): bamboo shoots, maize, sweet potatoes
- Genetic factors and dyshormonogenesis (enzyme defects in thyroid hormone synthesis)
- Graves' disease (autoimmune, TSH-receptor stimulation)
- Hashimoto's thyroiditis (autoimmune destruction with compensatory enlargement)
- Drugs: amiodarone (can cause either hypo- or hyperthyroidism depending on iodine status), lithium
- Sporadic: in iodine-sufficient areas, the specific cause is often not identified
The thyroid undergoes cycles of activity and regression, leading to nodule formation - some solid, some cystic.
- Textbook of Family Medicine 9e, p. 315
- Current Surgical Therapy 14e, p. 880
- Gray's Anatomy for Students, p. 7340
Clinical Features
-
Painless neck swelling is the classic presentation - the mass moves upward on swallowing (attached to larynx by pretracheal fascia)
-
Compressive symptoms with large goiters:
- Dyspnea, stridor (inspiratory "crowing" sound from tracheal compression)
- Dysphagia (esophageal compression)
- Hoarseness (pressure on larynx or stretching of recurrent laryngeal nerve)
- Venous congestion / neck discomfort with movement
-
Pemberton's sign: raising both arms above the head causes facial plethora and redness from venous obstruction - a sign of significant substernal extension
-
Tracheal deviation (away from a large unilateral lobe)
-
Hypothyroid symptoms (in large nontoxic MNG): weight gain, bradycardia, lethargy
-
Hyperthyroid symptoms (in toxic MNG or Graves'): palpitations, weight loss, heat intolerance
-
Goldman-Cecil Medicine, p. 3278
-
Current Surgical Therapy 14e, p. 1829
-
Gray's Anatomy for Students, p. 7340-7360
Evaluation
- Thyroid function tests: TSH, free T4, T3 - to identify hypo-, hyper-, or euthyroid state
- Ultrasound: primary imaging for nodule characterization; features raising malignancy risk:
- Hypoechogenicity
- Microcalcifications
- Hypervascularity
- Solid component of complex nodule
- Regional lymphadenopathy
- Fine-needle aspiration (FNA): for any sonographically suspicious nodule
- CT scan (non-contrast): best for assessing tracheal compression, retrosternal extension, airway geometry - contrast is avoided to prevent iodine load precipitating acute hyperthyroidism
- Chest X-ray: tracheal deviation, retrosternal/retrotracheal extension, calcification
- Fiber-optic laryngoscopy: for any patient with voice change or prior neck surgery
- Flow-volume loop: can detect external tracheal compression
- Goldman-Cecil Medicine, p. 3278
- Current Surgical Therapy 14e, p. 1838-1842
CT Imaging Example
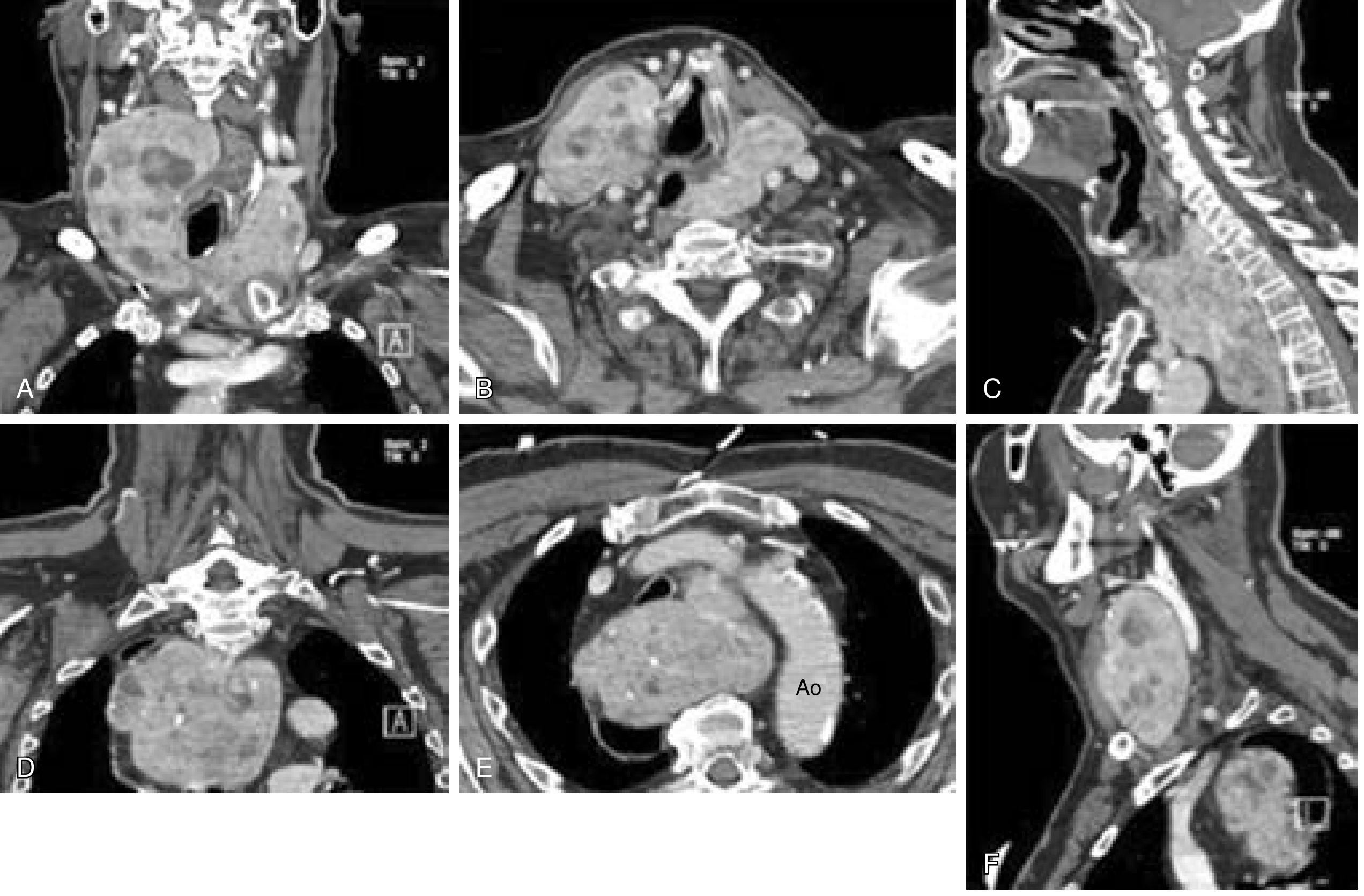
CT of an 82-year-old man with massive bilateral multinodular goiter (A,B), retrosternal left lobe (C,D), extension below the aortic arch (E, Ao = aorta), and displacement of the right common carotid artery (F). Required manubriotomy for safe resection. - Current Surgical Therapy 14e
Treatment
Indications for Intervention
- Local compressive symptoms (choking, dyspnea, dysphagia)
- Partial obstruction of the upper aerodigestive tract
- Substantial substernal extension (even if asymptomatic) - relative indication, as further growth may require more disruptive surgery later
- Cosmesis (rarely the sole indication)
Treatment Modalities
| Modality | Role |
|---|---|
| Total or subtotal thyroidectomy | Definitive treatment for large/compressive goiters |
| Radioactive iodine (RAI) | Reduces goiter size ~40-50%; useful in high-risk surgical patients; can transiently worsen compressive symptoms by causing swelling |
| TSH-suppression with thyroxine | Limited role in established MNG; prospective trials show little benefit; side effects (bone loss, arrhythmias) outweigh benefit especially in elderly |
| Thyroid hormone replacement | Indicated when hypothyroidism is present |
- Current Surgical Therapy 14e, p. 1856-1863
- Goldman-Cecil Medicine, p. 3283
Surgical Complications (Post-Thyroidectomy)
-
Hypocalcemia / tetany: from inadvertent removal or devascularization of parathyroid glands (manifests as tingling in hands, feet, perioral area, and carpopedal spasm)
-
Recurrent laryngeal nerve (RLN) injury: hoarseness, vocal cord paralysis
-
Hemorrhage / hematoma
-
Hypothyroidism: requires lifelong levothyroxine replacement after total thyroidectomy
-
Gray's Anatomy for Students, p. 7368
Key Points at a Glance
- Goiter = thyroid enlargement; most are benign
- Leading global cause = iodine deficiency
- Diffuse goiters are almost always benign; asymmetric/nodular goiters require malignancy workup
- Pemberton's sign flags substernal compression
- Non-contrast CT is the gold standard for airway and mediastinal assessment
- Surgery is the mainstay for compressive or cosmetically significant goiter; TSH suppression has minimal evidence benefit
This is a shared conversation. Sign in to Orris to start your own chat.