ABG
Reading File
Asking for Preferences
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Here is a complete reference on ABG normal values and their clinical significance, sourced from authoritative medical textbooks.
Arterial Blood Gas (ABG) - Normal Values & Clinical Significance
Normal Reference Ranges
| Parameter | Normal Value | Normal Range |
|---|---|---|
| pH | 7.40 | 7.35 - 7.45 |
| PaCO₂ | 40 mm Hg | 35 - 45 mm Hg (4.5 - 6.0 kPa) |
| PaO₂ | ~95-100 mm Hg | 75 - 100 mm Hg (10.6 - 13.3 kPa) |
| HCO₃⁻ (bicarbonate) | 24 mEq/L | 22 - 26 mEq/L |
| Base Excess/Deficit | 0 | 0 ± 3 mmol/L |
| O₂ Saturation (SaO₂) | ~98% | 95 - 100% |
- Current Surgical Therapy 14e, p.1608 | Pye's Surgical Handicraft
What Each Parameter Tells You
1. pH (7.35 - 7.45)
- < 7.35 = Acidemia
- > 7.45 = Alkalemia
- The pH is your first and most important number - it tells you the net acid-base state of the blood.
2. PaCO₂ (35 - 45 mm Hg) - The "Respiratory Component"
Reflects alveolar ventilation. In respiratory disorders, PaCO₂ moves opposite to pH:
- ↑ PaCO₂ (hypercapnia) + ↓ pH = Respiratory acidosis (hypoventilation)
- ↓ PaCO₂ (hypocapnia) + ↑ pH = Respiratory alkalosis (hyperventilation)
In metabolic disorders, PaCO₂ moves in the same direction as pH (compensatory).
3. PaO₂ (75 - 100 mm Hg) - Oxygenation
- The gold standard measure of oxygenation (better than pulse oximetry)
- Affected by altitude: PaO₂ in Denver (~1500 m altitude) is ~20 mm Hg lower than at sea level
- Decreases with age: PaO₂ = 109 - 0.43 × (age in years)
- Decreases in supine position due to diaphragm displacement and V/Q mismatch
- Causes of low PaO₂: hypoventilation, V/Q mismatch, diffusion impairment, shunt
- Fishman's Pulmonary Diseases and Disorders
4. HCO₃⁻ (22 - 26 mEq/L) - The "Metabolic Component"
- ↓ HCO₃⁻ = Metabolic acidosis
- ↑ HCO₃⁻ = Metabolic alkalosis
- Note: The HCO₃⁻ on an ABG report is a calculated value, not directly measured. Always confirm with a simultaneous electrolyte panel.
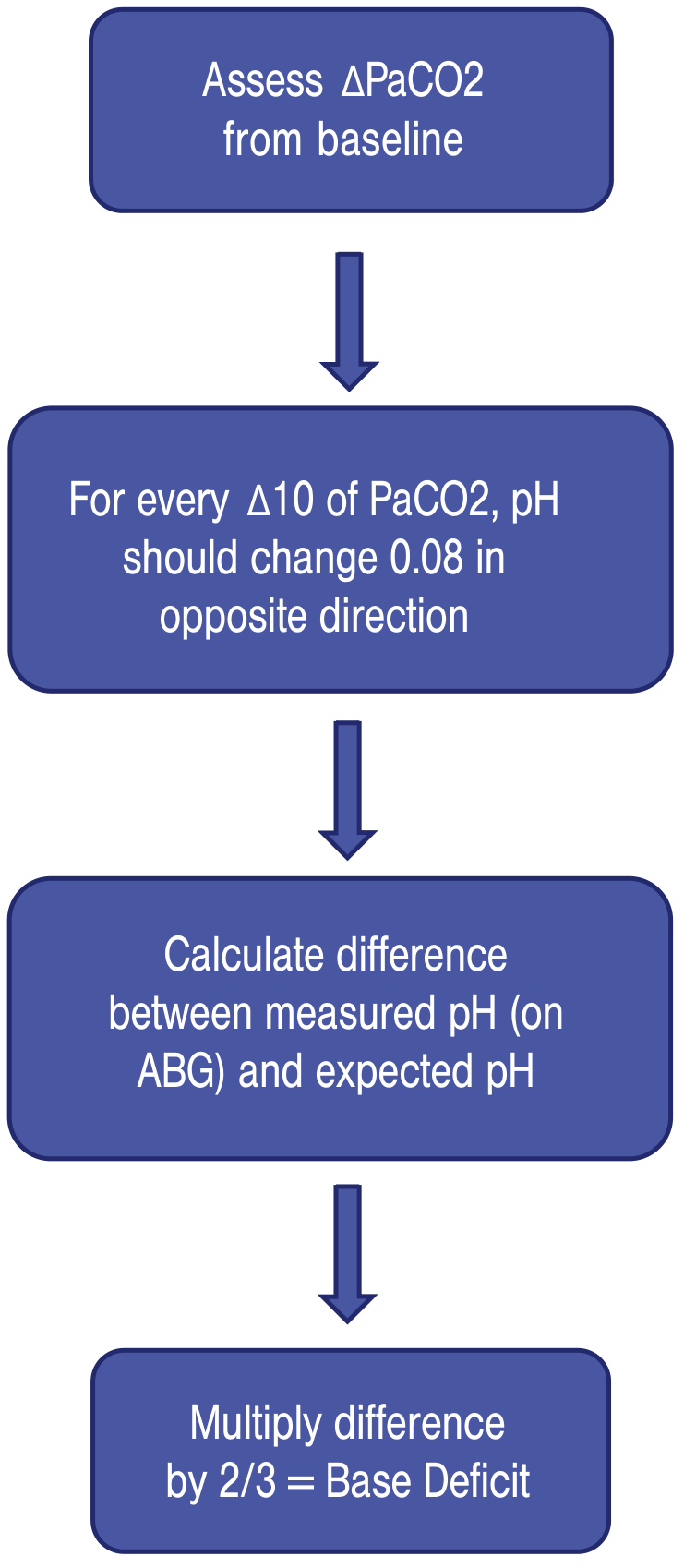
5. Base Excess / Base Deficit (0 ± 3 mmol/L)
- Defined as the amount of base needed to titrate 1 L of blood to pH 7.4 at 37°C
- > +3 = Metabolic alkalosis
- < -3 (base deficit) = Metabolic acidosis
- Purely reflects the metabolic component of acid-base balance
Calculating base deficit:
ABG vs. Other Blood Gas Methods
| Test | Use | Key Difference |
|---|---|---|
| ABG (arterial) | Most accurate - oxygenation, ventilation, acid-base | Gold standard |
| VBG (venous) | Quick screen for acid-base | PvCO₂ is ~6-8 mmHg higher; pH slightly lower than arterial |
| CBG (capillary) | Pediatric/bedside use | Correlates best for pH, moderate for PCO₂, worst for PO₂ |
- Harriet Lane Handbook, 23rd ed.
In Vitro Changes (Sample Handling)
If the sample is not iced and analyzed immediately, the values drift over time at 37°C:
| Parameter | Change per 10 min |
|---|---|
| pH | -0.01 |
| PCO₂ | +1.0 mm Hg |
| O₂ content | -0.001 vol% |
Blood cell metabolism (especially WBCs) consumes O₂ and produces CO₂, so samples must be kept on ice or analyzed promptly. Air bubbles in the syringe will also artificially raise PaO₂ and lower PaCO₂.
- Fishman's Pulmonary Diseases and Disorders
Quick Clinical Significance Summary
| Finding | Meaning | Common Causes |
|---|---|---|
| pH < 7.35, ↑ PaCO₂ | Respiratory acidosis | COPD, opioids, neuromuscular disease |
| pH > 7.45, ↓ PaCO₂ | Respiratory alkalosis | Anxiety, PE, pain, mechanical overventilation |
| pH < 7.35, ↓ HCO₃⁻ | Metabolic acidosis | MUDPILES: Methanol, Uremia, DKA, Propylene glycol, INH, Lactic acidosis, Ethylene glycol, Salicylates |
| pH > 7.45, ↑ HCO₃⁻ | Metabolic alkalosis | Vomiting, diuretics, hyperaldosteronism |
| PaO₂ < 60 mm Hg | Hypoxemic respiratory failure | Pneumonia, ARDS, PE, pulmonary edema |
Compensation Formulas
When a primary disorder is present, the body compensates. Use these to check whether the compensation is appropriate or if a mixed disorder is present:
| Primary Disorder | Expected Compensation |
|---|---|
| Metabolic acidosis | PaCO₂ = 1.5 × [HCO₃⁻] + 8 ± 2 (Winter's Formula) |
| Metabolic alkalosis | PaCO₂ = 0.7 × [HCO₃⁻] + 20 ± 5 |
| Acute respiratory acidosis | ↑ HCO₃⁻ = ΔPaCO₂ / 10 |
| Chronic respiratory acidosis | ↑ HCO₃⁻ = 4 × (ΔPaCO₂ / 10) |
| Acute respiratory alkalosis | ↓ HCO₃⁻ = 2 × (ΔPaCO₂ / 10) |
| Chronic respiratory alkalosis | ↓ HCO₃⁻ = 4 × (ΔPaCO₂ / 10) |
- Current Surgical Therapy 14e
Key takeaway: The ABG gives you four core values - pH, PaCO₂, PaO₂, and HCO₃⁻. Use pH to identify acidemia vs. alkalemia, PaCO₂ for the respiratory component, and HCO₃⁻/base excess for the metabolic component. Always check PaO₂ for concurrent hypoxemia, and apply compensation formulas to detect mixed disorders.
This is a shared conversation. Sign in to Orris to start your own chat.