Clinical methods: complete cardiovascular system examination as per Hutchinson and other accurate resources comprehensive
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have all the content needed. Let me compile the comprehensive cardiovascular examination guide.
Complete Cardiovascular System Examination
Sources: Harrison's Principles of Internal Medicine 22e (2025); Fuster and Hurst's The Heart 15e; Braunwald's Heart Disease
I. GENERAL INSPECTION (Before Touching the Patient)
Look for signs that betray cardiovascular disease at a glance:
Facies and body habitus
- Malar flush (mitral stenosis)
- Marfanoid habitus (tall, long extremities, pectus excavatum/carinatum - aortic root disease, MVP)
- Down syndrome (AV canal, VSD, ASD)
- Turner syndrome (coarctation of aorta, bicuspid aortic valve)
- Noonan syndrome (pulmonary stenosis, HCM)
- Acromegaly (cardiomegaly, hypertension)
- Cushing syndrome (hypertension, cardiomegaly)
Skin and extremities
- Central cyanosis: bluish discoloration of lips/tongue - right-to-left shunts, severe pulmonary disease
- Peripheral cyanosis: fingertips/toes - reduced peripheral circulation
- Clubbing: infective endocarditis, cyanotic congenital heart disease, Eisenmenger syndrome
- Splinter haemorrhages (infective endocarditis)
- Janeway lesions (painless palmar/plantar embolic lesions - infective endocarditis)
- Osler nodes (painful nodules on fingertips - infective endocarditis)
- Xanthelasma and tendon xanthomata (hypercholesterolaemia, premature atherosclerosis)
- Arcus senilis (significant if <45 years)
- Koilonychia (iron-deficiency anaemia causing high-output state)
Respiratory signs
- Dyspnoea at rest, tachypnoea
- Cheyne-Stokes breathing (severe LV failure)
II. BLOOD PRESSURE
Technique (Harrison's)
- Patient seated, arm at heart level, feet on floor, back supported; 5-10 min rest
- Cuff bladder: length 80%, width 40% of arm circumference
- Inflate 30 mmHg above expected systolic; deflate at 2-3 mmHg/s
- Systolic = Phase I Korotkoff sound; Diastolic = Phase V (disappearance); record both Phase IV and Phase V when diastolic near zero (severe AR, large AV fistula)
Both arms - difference should be <10 mmHg; if >10 mmHg, suspect atherosclerotic/inflammatory subclavian disease, supravalvular AS, aortic coarctation, or aortic dissection.
Leg pressures - Systolic leg pressure normally 20 mmHg higher than arm; increased further in chronic severe AR and calcified lower limb vessels.
Ankle-Brachial Index (ABI) - Dorsalis pedis or posterior tibial systolic / higher brachial systolic; a powerful predictor of long-term cardiovascular mortality.
Pulse pressure - Narrow: shock, severe AS (low output). Wide: hypertension, severe AR (low diastolic from runoff), patent ductus arteriosus, dialysis fistula.
Pulsus alternans - Beat-to-beat variation in systolic BP or Korotkoff sound intensity, regular rhythm; sign of severe LV systolic dysfunction. Both palpation and auscultation can detect it (patient breathes calmly).
Pulsus paradoxus - Fall >10 mmHg in systolic BP with inspiration. Inflate cuff 15-20 mmHg above systolic; slowly deflate; note the first Korotkoff sounds (expiration only), then when heard with every beat regardless of phase. The difference is the "pulsus." Classic in cardiac tamponade, constrictive pericarditis, massive PE, severe COPD, morbid obesity.
Orthostatic hypotension - Fall >20 mmHg systolic or >10 mmHg diastolic within 3 minutes of standing from supine; lack of compensatory tachycardia suggests autonomic insufficiency (diabetes, Parkinson disease).
III. ARTERIAL PULSE EXAMINATION
Sites to examine routinely (Harrison's): subclavian, brachial, radial, ulnar, femoral, popliteal, dorsalis pedis, posterior tibial. Add temporal arteries if temporal arteritis/PMR suspected.
Assess: Rate, rhythm, volume (amplitude), character (contour), symmetry, timing, duration.
Best character assessment: at the carotid artery level. Never palpate both carotids simultaneously; always use light pressure (avoid carotid hypersensitivity syndrome).
Pulse Characters and Their Clinical Significance
| Pulse | Character | Condition |
|---|---|---|
| Normal | Smooth upstroke, well-defined peak, gentle dicrotic notch | - |
| Pulsus parvus et tardus | Weak, small amplitude, slow delayed upstroke (anacrotic) | Severe aortic stenosis |
| Corrigan/water-hammer | Sharp rapid rise, then abrupt collapse | Severe aortic regurgitation |
| Bisferiens | Two systolic peaks (percussion + tidal wave) | Severe AR, HOCM |
| Dicrotic | One systolic + one diastolic peak | Sepsis, IABP counterpulsation |
| Pulsus paradoxus | >10 mmHg fall in systole with inspiration | Tamponade, constrictive pericarditis, massive PE |
| Pulsus alternans | Beat-to-beat amplitude variation (regular rhythm) | Severe LV systolic dysfunction |
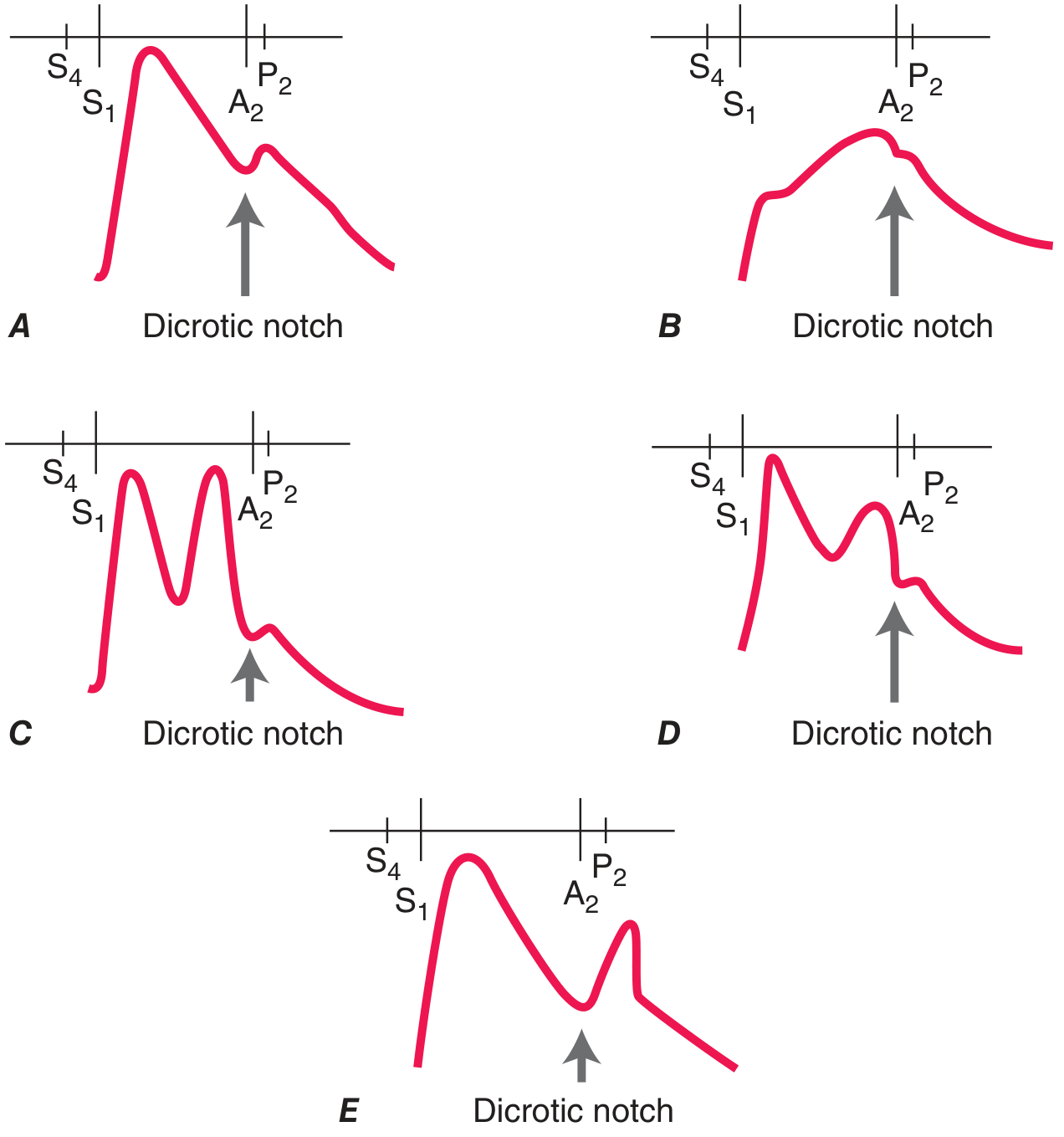
Harrison's Fig. 246-2: Schematic carotid pulse configurations. A. Normal. B. Aortic stenosis - anacrotic, slow upstroke (tardus), reduced peak (parvus). C. Bisferiens with two systolic peaks in severe AR. D. Bisferiens in HOCM - rapid upstroke to percussion wave then tidal wave. E. Dicrotic pulse (systolic + diastolic peaks, as in sepsis or IABP).
Peripheral vascular examination: Auscultate for bruits over carotid, subclavian, abdominal aorta, and femoral arteries. A bruit extending into diastole or accompanied by a thrill indicates severe obstruction. A normal oximetry difference >2% between finger and toe suggests lower limb arterial disease. Simultaneous radial-femoral palpation detects femoral delay in aortic coarctation.
IV. JUGULAR VENOUS PRESSURE AND WAVEFORM
Patient Positioning
- Begin in semi-recumbent position (30-45°)
- Examine the internal jugular vein (preferred - directly in line with SVC and right atrium; the external jugular is valved)
- Measure the vertical height of venous pulsation above the sternal angle (angle of Louis); >4.5 cm at 30-45° is abnormal
- The sternal angle reference underestimates CVP - use it to distinguish normal from elevated rather than to quantify precisely
- Alternatively, pulsations above the clavicle in the sitting position are clearly abnormal (clavicle-to-RA distance >10 cm)
- Convert cmH₂O to mmHg: 1.36 cmH₂O = 1.0 mmHg
Differentiating JVP from Carotid Pulse
- Venous pulsation is non-palpable (easily obliterated by light pressure); carotid is palpable
- JVP is usually biphasic (in sinus rhythm); carotid is monophasic
- JVP changes with posture and inspiration; carotid does not
- JVP can be abolished by pressing below the jaw
The JVP Waveform Components
| Component | Timing | Origin | Correlates with |
|---|---|---|---|
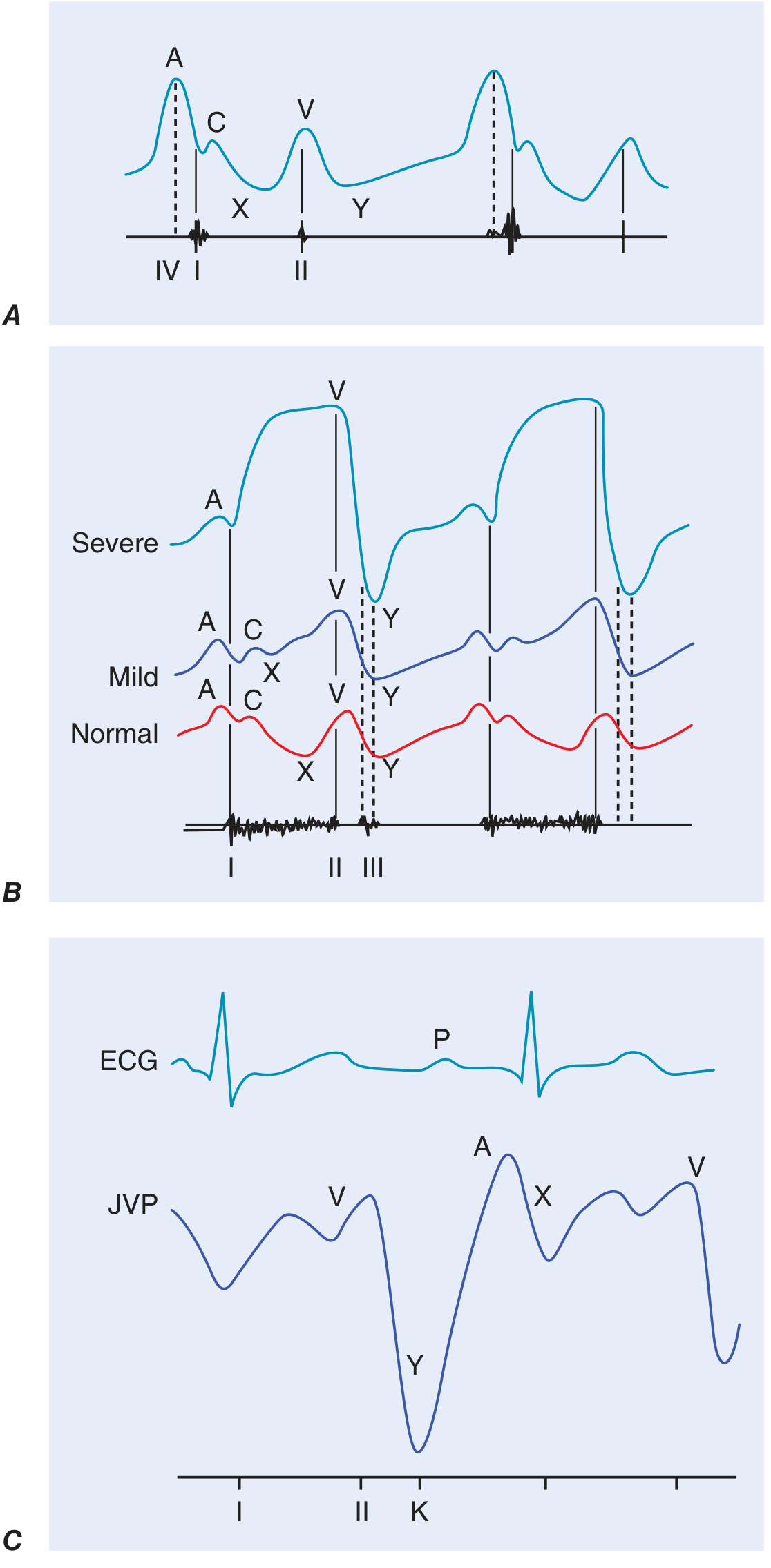
| a wave | Just after P wave, before S1 | Right atrial presystolic contraction | ECG P wave |
| c wave | Early systole | Tricuspid valve bulging into RA + carotid artifact | Follows a wave |
| x descent | Systole (after c) | Atrial relaxation + downward displacement of tricuspid annulus | Fall in RA pressure |
| v wave | Late systole / early diastole | Atrial filling while tricuspid closed | RA filling during ventricular systole |
| y descent | Diastole | Tricuspid valve opens, blood flows into RV | Early RV filling |
Abnormalities of Each Component
a wave abnormalities:
- Large (prominent) a wave: reduced RV compliance (pulmonary hypertension, pulmonary stenosis, tricuspid stenosis)
- Cannon a wave: AV dissociation - RA contracts against closed tricuspid valve (VT diagnosis clue!)
- Absent a wave: atrial fibrillation
x descent abnormalities:
- Blunted/absent: atrial fibrillation (no atrial relaxation), tricuspid regurgitation (replaced by v wave)
- Deep x descent: constrictive pericarditis (enhanced annular descent + preserved atrial relaxation)
v wave abnormalities:
- Large v wave (CV wave = ventricularization): severe tricuspid regurgitation - regurgitant volume raises RA pressure throughout systole; in extreme cases, single large positive systolic wave
y descent abnormalities:
- Rapid, prominent y descent: tricuspid regurgitation, constrictive pericarditis, restrictive cardiomyopathy (rapid early RV filling)
- Blunted/absent y descent: cardiac tamponade (elevated pericardial pressure prevents early diastolic RV filling), tricuspid stenosis
Kussmaul Sign: Rise (or failure to fall) of JVP with inspiration. Classic in constrictive pericarditis; also seen in restrictive cardiomyopathy, massive PE, RV infarction, advanced LV failure, post-cardiac surgery.
Abdominojugular (Hepatojugular) Reflux: Firm, steady pressure on the right upper quadrant (or around the umbilicus) for >15 seconds. Positive = sustained rise of >3 cm in JVP during pressure. Assess after 10 seconds to allow respiratory artifact/abdominal tensing to subside. Patient must not hold breath or Valsalva. Positive result predicts pulmonary artery wedge pressure >15 mmHg. An elevated JVP itself predicts wedge pressure >22 mmHg with positive predictive value of 88%.
Prognostic significance: Elevated JVP is associated with higher risk of HF hospitalization and death in both symptomatic and asymptomatic LV systolic dysfunction.
V. PRECORDIAL EXAMINATION
1. Inspection
- Scars: median sternotomy (previous cardiac surgery), lateral thoracotomy
- Visible apex beat (normally 5th ICS, midclavicular line)
- Visible pulsation at left sternal border (RV heave), upper left sternal border (pulmonary artery dilation in pulmonary hypertension), right parasternal (aortic aneurysm)
- Chest deformities: pectus excavatum (Marfan, MVP), pigeon chest
2. Palpation
Palpation is "perhaps the most underemphasized part of the cardiovascular examination" (Fuster and Hurst's). It allows assessment of ventricular size, valve function, diastolic function (palpable S3/S4), and pulmonary hypertension.
Apex beat (apical impulse)
- Normal: 5th intercostal space, just medial to the midclavicular line; brief, non-sustained tap
- Displaced laterally and/or downward: LV dilatation (volume overload - MR, AR, DCM)
- Sustained/heaving impulse: LV hypertrophy (pressure overload - AS, hypertension)
- Double impulse (bifid apex): HOCM (palpable S4 + systolic impulse), severe MR
- Tapping apex: palpable S1 (mitral stenosis)
- Hyperdynamic apex: high-output states, volume overload
Left parasternal palpation (right ventricular impulse)
- Place heel of hand at left sternal border (3rd-4th ICS)
- RV heave/lift = sustained outward thrust: RV hypertrophy or dilatation (pulmonary hypertension, pulmonary stenosis, severe MR with enlarged right heart)
Pulmonary artery palpation (2nd left ICS)
- Palpable P2 = pulmonary hypertension
- Diastolic shock in pulmonary hypertension
Thrills = palpable murmurs (Grade 4+)
- 2nd right ICS: AS, aortic sclerosis
- 2nd left ICS: pulmonary stenosis
- Lower left sternal border: VSD
- Apex: MR, MS (diastolic thrill)
3. Percussion
Cardiac percussion (to estimate cardiac dullness) is not routinely necessary in current practice - chest radiography and echocardiography provide this information more accurately (Fuster and Hurst's). It may still be used to confirm dextrocardia.
VI. AUSCULTATION
Technique
Use both the diaphragm (high-pitched sounds - S1, S2, AS murmur, MR, TR, AR murmur, pericardial friction rub) and the bell (low-pitched sounds - S3, S4, MS rumble). The bell must be applied with light skin contact; firm pressure converts it into a diaphragm and eliminates low-frequency sounds.
Classical auscultatory areas:
- Aortic area: 2nd right ICS
- Pulmonary area: 2nd left ICS
- Tricuspid area: Lower left sternal border / xiphoid
- Mitral area (apex): 5th ICS, MCL
Note: Murmurs do not respect these areas strictly. Always auscultate the entire precordium and track radiation into the axilla, neck, and back.
Patient positions for auscultation:
- Supine: baseline assessment
- Left lateral decubitus: brings LV apex closer to chest wall; enhances S3, S4, and MS rumble
- Sitting forward, breath held in expiration: brings aortic valve close; enhances AR diastolic murmur and pericardial rub
Heart Sounds
S1 (First Heart Sound)
- Produced by closure of mitral (M1) and tricuspid (T1) valves
- M1 precedes T1; normally heard as a single sound at apex
- Best heard: apex with diaphragm
Intensity of S1:
- Loud S1: mitral stenosis (mobile leaflets), short PR interval, high cardiac output states
- Soft S1: calcified/immobile mitral leaflets (advanced MS), long PR interval (1st degree AV block), severe MR (early valve closure), LV systolic dysfunction
- Variable S1: complete heart block (PR interval changes beat-to-beat), AF
Splitting of S1: Wide splitting suggests RBBB or Ebstein anomaly.
S2 (Second Heart Sound)
- Produced by closure of aortic (A2) and pulmonary (P2) valves
- A2 normally precedes P2; best heard at base (2nd ICS)
- P2 normally audible only at 2nd left ICS; if heard at apex or widely - pulmonary hypertension
Splitting of S2:
- Physiological splitting: normal with inspiration (increased RV stroke volume delays P2); disappears on expiration
- Wide fixed splitting: ASD (constant volume overload of right heart)
- Wide splitting (not fixed): RBBB, pulmonary stenosis, MR (early A2 from reduced LV output), VSD
- Paradoxical (reversed) splitting: A2 comes after P2; heard in expiration, disappears with inspiration. Causes: LBBB, severe AS (delayed A2), HOCM, RV pacing, PDA
P2 intensity:
- Loud P2: pulmonary hypertension
- Soft P2: severe pulmonary stenosis (immobile valve)
- A2-P2 interval inversely proportional to severity of pulmonary hypertension (narrower with increasing PHTN)
S3 (Third Heart Sound)
- Low-pitched, heard in early diastole during rapid ventricular filling phase
- Best heard: LV apex, with bell, left lateral decubitus
- Rhythm: "Ken-tuc-ky"
- Normal: children, young adults, athletes, pregnancy (physiological)
- Pathological: heart failure (predicts HF morbidity/mortality), dilated cardiomyopathy, volume overload (MR, AR)
- Right-sided S3: lower left sternal border, louder with inspiration; seen in severe RV dysfunction, severe TR
- S3 equally prevalent in HFpEF and HFrEF
S4 (Fourth Heart Sound)
- Low-pitched, heard in late diastole (atrial filling phase) - presystolic
- Best heard: LV apex with bell
- Rhythm: "Ten-nes-see"
- Indicates reduced ventricular compliance; LV presystolic expansion
- Causes: LV hypertrophy (hypertension, AS, HOCM), active myocardial ischemia/infarction, hypertrophic cardiomyopathy
- Absent with: atrial fibrillation (no active atrial contraction)
- Right-sided S4: louder with inspiration; pulmonary hypertension, pulmonary stenosis
Gallop Rhythms
- S3 gallop: tachycardia + S3 (heart failure)
- S4 gallop: tachycardia + S4 (ischemia, hypertrophy)
- Summation gallop: tachycardia with both S3 + S4 occurring simultaneously (fast heart rate merges them); analogous to fused E+A waves on echo Doppler
Opening Snap (OS) - Mitral Stenosis
- High-pitched, early diastolic sound; heard after S2
- Heard best: lower left sternal border and apex; wide radiation (can be heard at aortic area)
- Distinguished from S3: OS is high-pitched (unlike low-pitched S3); louder with diaphragm; heard at sternal border not just apex
- A2-OS interval: inversely proportional to LA-LV diastolic pressure gradient and severity of MS
- Short A2-OS (<70 ms): severe MS (elevated LA pressure, early MV opening)
- Long A2-OS (>100 ms): mild MS
- Crisp/loud OS: mobile, pliable leaflets - amenable to balloon valvuloplasty
- Soft/absent OS: calcified, immobile leaflets - not suitable for valvuloplasty
Pericardial Knock
- High-pitched early diastolic sound, slightly later than OS
- Corresponds to abrupt cessation of ventricular expansion after tricuspid valve opening
- Associated with prominent rapid y descent on JVP
- Constrictive pericarditis
Tumor Plop
- Lower-pitched diastolic sound; atrial myxoma prolapsing across mitral valve
- Position-dependent
Ejection Sounds (Clicks)
- High-pitched, early systolic, corresponds to upstroke of carotid pulse
- Aortic ejection sound: bicuspid aortic valve, aortic root dilation; becomes softer as valve calcifies
- Pulmonary ejection sound: pulmonary valve stenosis, pulmonary root dilation
- Only right-sided acoustic event that decreases with inspiration
- Moves closer to S1 as PS severity increases
- Both heard best at lower left sternal border, not just the base
Non-Ejection Click (Mid-Systolic Click) - Mitral Valve Prolapse
- High-pitched click after carotid upstroke
- May be single or multiple; may introduce a late systolic murmur
- Moves toward S2 (away from S1) with maneuvers that increase LV preload (squatting)
- Moves toward S1 with maneuvers that decrease preload (standing, Valsalva)
Heart Murmurs
Grading system (Levine scale):
| Grade | Description |
|---|---|
| 1 | Barely audible; requires careful auscultation in a quiet room |
| 2 | Soft but immediately audible |
| 3 | Moderately loud; no thrill |
| 4 | Loud; thrill present |
| 5 | Very loud; heard with stethoscope edge tilted off chest |
| 6 | Heard without stethoscope |
A thrill = Grade 4 or greater.
Systolic Murmurs
Holosystolic (pansystolic) murmurs:
- Start immediately at S1 (at mitral valve closure) and extend to S2
- High-pitched, plateau (constant intensity), harsh or blowing quality
- Mechanism: pressure gradient from ventricle to atrium (or VSD) throughout entire systole
- Mitral regurgitation (MR): best at apex; radiation to axilla (anteriorly directed jet from posterior leaflet prolapse radiates to base; posteriorly directed jet from anterior leaflet prolapse radiates to back/spine)
- Tricuspid regurgitation (TR): lower left sternal border; louder with inspiration (Carvallo's sign)
- VSD: lower left sternal border; may be associated with thrill
Systolic ejection (midsystolic) murmurs:
- Start after S1 (after semilunar valve opens = end of isovolumetric contraction), end before or at S2
- Crescendo-decrescendo (diamond-shaped) configuration; harsh quality
- Aortic stenosis (AS): 2nd right ICS; radiates to carotids and apex; late-peaking, harsh
- Severe AS: parvus et tardus carotid upstroke, late-peaking Grade ≥3, soft A2, sustained LV impulse, S4
- Pulmonary stenosis (PS): 2nd left ICS; preceded by ejection click; radiates to left shoulder
- HOCM: lower left sternal border/apex; Brockenbrough sign; responds dramatically to bedside maneuvers (see below)
- ASD: pulmonary area; due to increased pulmonary flow (not the defect itself); fixed split S2
- Flow murmurs: fever, anemia, thyrotoxicosis, pregnancy, high-output states
Late systolic murmurs:
- Begin in mid-late systole; introduced by non-ejection click
- MVP: click + late systolic murmur; apex + left sternal border
Diastolic Murmurs
Early diastolic (decrescendo):
- Begin immediately at S2; high-pitched; best heard with diaphragm
- Aortic regurgitation (AR): 3rd left ICS (left sternal border); best heard sitting forward, breath held in expiration; radiation to apex; Austin Flint murmur (low-pitched mid-diastolic rumble at apex due to AR jet hitting mitral leaflet)
- Pulmonary regurgitation: 2nd left ICS; Graham Steell murmur (high-pressure PR in pulmonary hypertension)
Mid-diastolic / Late diastolic (rumbles):
- Mitral stenosis: apex; low-pitched, rumbling; best heard with bell, left lateral decubitus; preceded by OS; presystolic accentuation in sinus rhythm (absent in AF); louder after exercise
- Tricuspid stenosis: lower left sternal border; louder with inspiration; preceded by OS
Continuous Murmurs
- Heard in both systole and diastole, peak around S2
- Patent ductus arteriosus (PDA): 2nd left ICS; "machinery" murmur
- Arteriovenous fistula; coronary arteriovenous fistula; rupture of sinus of Valsalva aneurysm
Bedside Maneuvers to Identify Murmurs
| Maneuver | Effect on LV preload | Murmur changes |
|---|---|---|
| Standing | Decreases | HOCM ↑; MVP click moves toward S1; AS/MR ↓ |
| Squatting | Increases | HOCM ↓; MVP click moves toward S2; AS/MR ↑ |
| Valsalva (strain phase) | Decreases | HOCM ↑; MVP ↑; AS ↓; MR ↓ |
| Valsalva (release phase) | Increases | All murmurs transiently loud |
| Passive leg raising | Increases | HOCM ↓ |
| Inspiration | Right heart filling increases | TR ↑ (Carvallo's); right-sided S3, S4 ↑; pulmonic ejection click ↓ |
| Expiration | Left heart effects | AR murmur louder; aortic click louder |
| Handgrip | Increases afterload | MR ↑; AR ↑; HOCM ↓; AS unchanged |
| Amyl nitrite | Decreases afterload/BP | AS ↑; AR ↓; HOCM ↑ |
Brockenbrough sign (HOCM): Post-extrasystolic beat - in AS the pulse pressure increases after the extra beat (more filling time); in HOCM the pulse pressure paradoxically decreases (more obstruction from increased contractility).
Pericardial Friction Rub
- Scratching, leathery, superficial sound with up to 3 components (atrial systole, ventricular systole, early diastole)
- Best heard: sitting forward, breath held in expiration, diaphragm pressed firmly
- Variable from examination to examination
- Present in acute pericarditis, post-MI (Dressler syndrome), post-cardiac surgery, uraemia
VII. PERIPHERAL EXAMINATION
Lower Limbs
- Oedema: pitting bilateral ankle/leg oedema; if JVP elevated = volume overload (CHF, constrictive pericarditis); if JVP normal = hypoalbuminaemia, venous insufficiency, CCB (dihydropyridine) side effect, lymphoedema
- Venous signs: varicosities, venous ulcers (medial, with brown hemosiderin discolouration - "eburnation")
- Arterial signs: pallor, cool skin, hair loss, muscular atrophy, absent pulses (peripheral arterial disease)
- Homans sign: posterior calf pain on active dorsiflexion against resistance for DVT - neither specific nor sensitive; should not be relied upon
Hepatomegaly
- Tender hepatomegaly = acute hepatic congestion from right heart failure
- Pulsatile liver = severe tricuspid regurgitation
- Systolic hepatic pulsation corresponds to regurgitant v waves
Splenomegaly
- Infective endocarditis (septic emboli)
VIII. SPECIAL SIGNS OF SYSTEMIC DISEASE AFFECTING THE HEART
| Sign | Association |
|---|---|
| Argyll Robertson pupils | Syphilitic aortitis |
| Roth spots (retinal haemorrhages with white centre) | Infective endocarditis |
| High-arched palate, lens dislocation | Marfan syndrome (aortic root, MVP) |
| Hereditary haemorrhagic telangiectasia | Pulmonary AV fistulae |
| Café-au-lait spots, axillary freckling | Neurofibromatosis (renal artery stenosis, carcinoid) |
| Lentigines | LEOPARD syndrome (hypertrophic CM) |
| Ehlers-Danlos skin | Aortic dissection |
IX. SYSTEMATIC ORDER OF CARDIOVASCULAR EXAMINATION (as per Hutchinson's Scheme)
- General inspection - position, distress, dyspnoea, body habitus, skin, face
- Hands - clubbing, cyanosis, peripheral signs of endocarditis, temperature, radial pulse
- Arms - blood pressure (both arms), brachial pulse
- Face/Eyes - xanthelasma, corneal arcus, conjunctival pallor/petechiae (anaemia, endocarditis), Roth spots, malar flush, cyanosis of lips, dental hygiene
- Neck - JVP (height and waveform), carotid pulse (character), carotid bruits
- Chest inspection - shape, scars, apex beat visibility, visible pulsations
- Palpation - apex beat (position, character), left sternal border heave, thrills, palpable P2
- Auscultation - systematic across all areas, appropriate positions, maneuvers as indicated
- Back - sacral oedema (bedridden), bibasal crepitations (pulmonary oedema), pleural effusion (dullness)
- Abdomen - hepatomegaly (size, tenderness, pulsatility), splenomegaly, ascites, abdominal aorta palpation and auscultation, renal bruits
- Lower limbs - femoral/popliteal/pedal pulses, femoral bruits, ankle/leg oedema, venous/arterial signs
- Fundoscopy - hypertensive/diabetic retinopathy, Roth spots
- Temperature/other vitals as indicated
Summary of Key Clinical Correlations
| Finding | Most Likely Cause |
|---|---|
| Cannon a waves in JVP | VT or complete heart block (AV dissociation) |
| Large v waves in JVP + pulsatile liver | Severe tricuspid regurgitation |
| Absent a wave in JVP | Atrial fibrillation |
| Kussmaul sign | Constrictive pericarditis (most specific), also severe RHF |
| Prominent y descent + pericardial knock | Constrictive pericarditis |
| Fixed wide split S2 | Atrial septal defect |
| Reversed split S2 | LBBB, severe AS, HOCM, RV pacing |
| Opening snap + diastolic rumble | Mitral stenosis |
| Short A2-OS interval | Severe MS (high LA pressure) |
| Ejection click + decreases with inspiration | Pulmonary valve stenosis |
| Click moves toward S1 on standing | Mitral valve prolapse |
| HOCM murmur increases with standing/Valsalva | Dynamic LVOTO |
| Pulsus paradoxus >10 mmHg | Cardiac tamponade (first choice) |
| Pulsus alternans | Severe LV systolic failure |
| Parvus et tardus carotid pulse | Severe aortic stenosis |
| Water-hammer (Corrigan) pulse | Severe aortic regurgitation |
| Bisferiens pulse | Severe AR, HOCM |
Sources: Harrison's Principles of Internal Medicine 22e, p. 1904-1910 (Chapter 246); Fuster and Hurst's The Heart 15e, Chapter 2 (Clinical Cardiovascular Examination, pp. 49-76, William R. Miranda & Rick A. Nishimura)
This is a shared conversation. Sign in to Orris to start your own chat.