Differentiate the pox viruses
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
I now have all the information needed for a comprehensive answer. Let me compile it:
Differentiation of Poxviruses
Poxviruses belong to the family Poxviridae, subfamily Chordopoxvirinae. They are large, double-stranded DNA viruses that replicate entirely in the cytoplasm, producing characteristic intracytoplasmic inclusion bodies. All human poxvirus infections are zoonotic except molluscum contagiosum and variola (smallpox), which are exclusively human pathogens.
Key lab differentiating point: G+C content varies by genus - Orthopoxviruses ~33%, Yatapoxviruses ~32%, Molluscum contagiosum virus ~60%, Parapoxviruses ~63%. PCR and DNA sequencing are the most precise identification tools. - Goldman-Cecil Medicine, p. 3589
1. Classification by Genus
| Genus | Human Pathogens | G+C Content |
|---|---|---|
| Orthopoxvirus | Variola, Vaccinia, Monkeypox (Mpox), Cowpox | ~33% |
| Parapoxvirus | Orf virus, Pseudocowpox, Bovine papular stomatitis | ~63% |
| Molluscipoxvirus | Molluscum contagiosum virus (MCV 1-4) | ~60% |
| Yatapoxvirus | Tanapox, Yabapox | ~32% |
2. Orthopoxviruses - Detailed Comparison
A. Smallpox (Variola)
- Virus: Orthopoxvirus variola
- Reservoir: Humans only (eradicated 1980; the only poxvirus reportable under International Health Regulations)
- Transmission: Inhalation of respiratory droplets; fomites; direct contact with rash lesions
- Incubation: 10-17 days (mean 12 days)
- Prodrome: High fever (38-40°C), headache, backache, vomiting, prostration
- Rash:
- Centrifugal distribution - lesions more numerous on face and extremities than trunk
- Lesions appear on palms and soles
- All lesions in the same stage of development in any one area (synchronous)
- Progresses: macule → papule → vesicle (day 4-5) → pustule (day 7) → crust (day 14)
- Deep-seated, hard, raised lesions
- Lymphadenopathy: Absent (key differentiator from monkeypox)
- Clinical subtypes: Ordinary (90%), Modified (5%, vaccinated), Flat (5%, nearly fatal), Hemorrhagic (<1%, always fatal)
- Mortality: Varied; ordinary type ~30% in unvaccinated
- Secondary attack rate: ~60% in unvaccinated contacts; ~4% in vaccinated
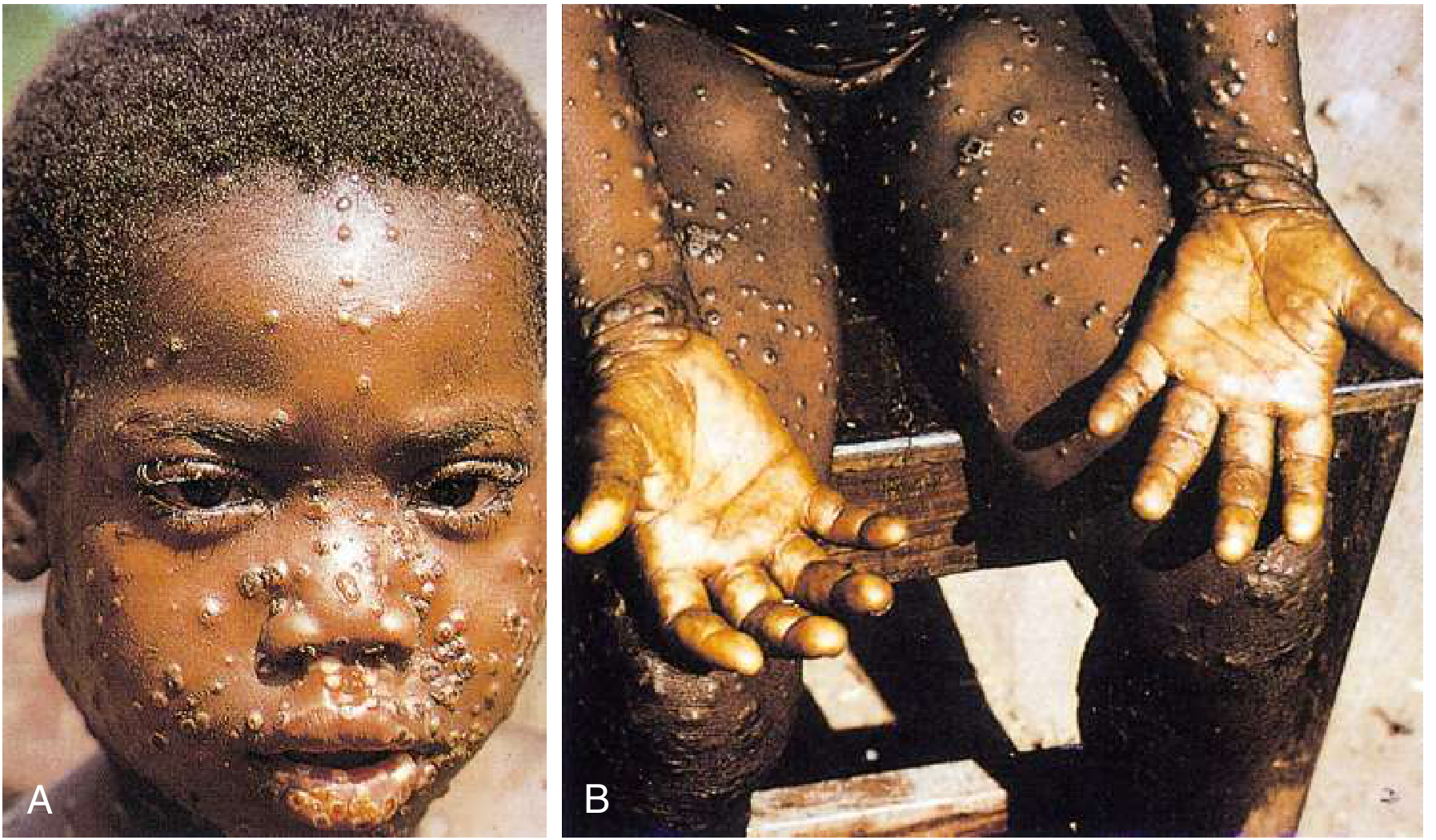
B. Monkeypox (Mpox)
- Virus: Orthopoxvirus monkeypox (two clades: Central African/Congo Basin and West African)
- Reservoir: Central/West African rodents (squirrels, Cricetomys); NOT monkeys despite name
- Transmission: Zoonotic (direct contact with animals); human-to-human via respiratory droplets, direct lesion contact, sexual contact
- Incubation: 7-17 days (mean 12 days)
- Prodrome: Fever, headache, backache, fatigue
- Rash: Very similar to smallpox - centrifugal, synchronous, macule → papule → vesicle → pustule → crust; involves palms and soles
- Key differentiator from smallpox: Pronounced lymphadenopathy (cervical, postauricular, submandibular, inguinal) - this is the hallmark clinical distinction
- Other features: Hypopigmentation followed by hyperpigmentation post-healing; pharyngitis, anorectal pain in recent outbreaks; 25-30% subclinical infection in contacts
- Clades: Congo Basin clade = more severe, higher mortality; West African clade = milder, no documented human-to-human transmission in 2003 US outbreak
- Mortality: Congo Basin clade >10%; West African clade <1%
- Smallpox vaccination: ~85% protective against monkeypox
C. Vaccinia
- Origin: Uncertain; likely hybrid of smallpox and cowpox, possibly derived from horsepox
- Reservoir: Used as live vaccine; variants include buffalopox (India) and dairy cattle variants (Brazil, Colombia)
- Transmission: Inoculation (vaccine); contact with vaccinees; zoonotic (buffalopox variant)
- Clinical use: The live virus in the smallpox vaccine; cross-protective against all orthopoxviruses (~33% sequence homology shared)
- Local reaction: Papule → vesicle (Jennerian vesicle) → pustule (days 7-9) → crust/scab (days 10-14) → scar
- Complications: Eczema vaccinatum, progressive vaccinia (in immunocompromised), generalized vaccinia, post-vaccinial encephalitis
- Immunity duration: Full protection 3-5 years; waning but significant immunity for decades
D. Cowpox
- Reservoir: Wild rodents (primary); cattle and cats are incidental hosts
- Transmission: Direct contact with infected animals (cat scratches are the most common source in Europe)
- Lesion: Usually restricted to hands and face; 70% have only ONE lesion; passes through macular → papular → vesicular → pustular → hard black crust (characteristic)
- Features: Very painful; significant erythema and edema; fever, malaise, lymphadenitis
- Severity: ~30% may require hospitalization; recovery takes 6-12 weeks; permanent scarring common
- Geography: Europe and western Asia
3. Parapoxviruses
E. Orf (Ecthyma Contagiosum)
- Virus: Orf virus
- Reservoir: Sheep and goats (occupational/contact zoonosis)
- Transmission: Direct contact with infected animals or their products; farmers, veterinarians, abattoir workers
- Lesion morphology (6 stages):
- Erythematous papule
- Target lesion - red center + white halo + outer inflamed halo
- Acute weeping nodule
- Nodular/papillomatous stage with "weeping" surface
- Regenerative/dry stage
- Papillomatous regression
- Number of lesions: Usually ONE (occasionally multiple with multiple inoculations)
- Systemic features: Relatively uncommon; lymphadenopathy in some
- Special complication: Erythema multiforme in up to one third of patients
- Self-limiting: Resolves in 4-6 weeks
F. Pseudocowpox (Milker's Nodule)
- Very similar to orf clinically
- Source: Cattle (milking contact)
- Occupational: Dairy farmers
4. Molluscipoxvirus
G. Molluscum Contagiosum (MCV)
- Virus: MCV types 1-4; the most common poxvirus affecting humans since smallpox eradication
- Reservoir: Humans only (like variola, but benign)
- Transmission: Skin-to-skin contact; fomites (towels, pools); sexual transmission in adults; autoinoculation/Koebnerization
- Population: Children (median age 5 years; most common <14 years); sexually active adults (genital lesions); HIV patients (severe, widespread disease)
- Lesion: 2-5 mm, discrete, dome-shaped, smooth, flesh-colored papule with central umbilication (pathognomonic)
- Histology: Henderson-Paterson bodies = large intracytoplasmic inclusion bodies (molluscum bodies) - diagnostic on biopsy
- Distribution: In children: exposed areas; in adults: genital area (STI)
- Complications: Eczematous reaction (molluscum dermatitis) around lesions; in HIV: giant molluscum (>1 cm), widespread hundreds of lesions; Gianotti-Crosti type reactions
- Treatment: Usually self-limiting (6-12 months); cryotherapy, curettage, topical agents
5. Yatapoxviruses
H. Tanapox / Yabapox
- Reservoir: Subhuman primates (Africa)
- Transmission: Direct contact; possibly insect vectors
- Lesion: 1-2 lesions, nodular, generally mild and self-limiting
- Geography: Restricted to Africa (Kenya, DR Congo)
- Key point: G+C ~32%; geographically restricted by reservoir distribution
6. Quick-Reference Comparison Table
| Feature | Smallpox | Monkeypox | Cowpox | Vaccinia | Orf | Molluscum |
|---|---|---|---|---|---|---|
| Genus | Orthopox | Orthopox | Orthopox | Orthopox | Parapox | Molluscipox |
| Reservoir | Humans | Rodents | Rodents | Lab/cattle | Sheep/goats | Humans |
| Incubation | 10-17 d | 7-17 d | 1-3 wks | - | 3-7 d | 2-8 wks |
| Rash distribution | Centrifugal | Centrifugal | Hands/face | Inoculation site | Hands/fingers | Any skin |
| Lesion stages | Synchronous | Synchronous | Synchronous | Synchronous | Target lesion | Dome + umbilication |
| Palms/soles | Yes | Yes | Yes | No | No | Rarely |
| Lymphadenopathy | No | Yes (prominent) | Yes (local) | Regional | Occasional | No |
| Number of lesions | Many | Many | Usually 1 | 1 (vaccine site) | Usually 1 | Multiple |
| Mortality | High (30%+) | Low-moderate | Low | Adverse reactions | Nil | Nil |
| Eradicated | Yes (1980) | No | No | Lab use only | No | No |
| Vaccination cross-protects | N/A | Yes (~85%) | Yes | N/A | No | No |
7. Key Diagnostic Differentiators
- Smallpox vs. Monkeypox: Lymphadenopathy distinguishes monkeypox (present) from smallpox (absent). Epidemiologic context (zoonotic exposure, geographic origin) is also key.
- Smallpox/Monkeypox vs. Chickenpox (varicella): Poxvirus lesions are synchronous (all same stage); varicella lesions are asynchronous (different stages simultaneously). Pox lesions are deep-seated; varicella lesions are superficial. Electron microscopy can distinguish poxvirus particles from herpesviruses in ~1 hour. - Jawetz Medical Microbiology
- Cowpox vs. Orf: Cowpox forms a hard black eschar; orf forms a target lesion with weeping surface. Both are occupational zoonoses.
- Molluscum: Pathognomonic central umbilication + Henderson-Paterson inclusion bodies; no systemic illness.
- Laboratory: PCR - non-variola orthopoxvirus (NVO) assay, generic orthopoxvirus PCR, mpox-specific PCR; G+C ratio by sequencing helps genus-level classification.
8. Treatment Summary
| Condition | Treatment |
|---|---|
| Orthopoxvirus (severe) | Tecovirimat (drug of choice; 600 mg PO q12h x14 days) |
| Orthopoxvirus (adjunct) | Brincidofovir or Cidofovir + Tecovirimat |
| Vaccinia adverse reactions | Vaccinia Immune Globulin (VIG) 6000 U/kg IV |
| Mpox with HIV | Optimize ART; avoid immunosuppressants |
| Molluscum | Cryotherapy, curettage, topical cidofovir (mixed results) |
| Orf/Cowpox | Supportive; large lesions may need surgical debridement |
- Goldman-Cecil Medicine, Chapter 343
- Harrison's Principles of Internal Medicine 22E, p. 1652
- Sherris & Ryan's Medical Microbiology, 8th Ed, p. 439
- Fitzpatrick's Dermatology, p. 3116
This is a shared conversation. Sign in to Orris to start your own chat.