Osteoarthritis
Reading File
Finding Sources
Searching PubMed
"osteoarthritis"[MeSH Terms] AND "management"[MeSH Terms]
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Now I have comprehensive content from multiple authoritative sources. Let me compile the full, detailed response on osteoarthritis.
Osteoarthritis (OA)
Definition
Osteoarthritis is characterized by failed repair of synovial joint tissues after intra-articular stress. The resulting breakdown of cartilage and bone produces pain, stiffness, and functional disability. Notably, structural changes on imaging often correlate poorly with patient-reported symptoms.
- Goldman-Cecil Medicine
It is primarily a degenerative disorder of articular cartilage, with inflammation acting as a secondary contributor rather than the primary driver - hence the term "osteoarthritis" is somewhat misleading.
- Robbins & Kumar Basic Pathology
Epidemiology
- Affects >500 million people worldwide; women are disproportionately affected
- Prevalence increases exponentially after age 50; ~40% of people older than 70 are affected
- Global burden rose 48% from 1990 to 2019; now the 15th highest cause of years lived with disability worldwide
- Lifetime risk of symptomatic knee OA: ~40% in men, ~47% in women; rises to 60% among those above a healthy weight
- Knee OA accounts for approximately 85% of the total OA burden
- An estimated 25% of the U.S. adult population will have physician-diagnosed OA by 2040
- Goldman-Cecil Medicine
Classification
| Type | Description |
|---|---|
| Primary (Idiopathic) OA | No apparent underlying cause; an aging phenomenon; oligoarticular, affecting weight-bearing joints |
| Secondary OA | Younger patients with a predisposing condition; accounts for ~5% of cases |
Secondary causes include: trauma (acute/chronic repetitive), metabolic disorders (hemochromatosis, Wilson disease, ochronosis), endocrine (acromegaly, hypothyroidism, hyperparathyroidism, diabetes mellitus), crystal deposition (CPPD, gout), rheumatoid arthritis, Paget disease, and bone/joint dysplasias.
- Grainger & Allison's Diagnostic Radiology
Typical distribution of primary OA: hands (DIP and PIP joints), thumb bases (1st CMC), hips, knees, and first metatarsophalangeal joint.
Pathogenesis
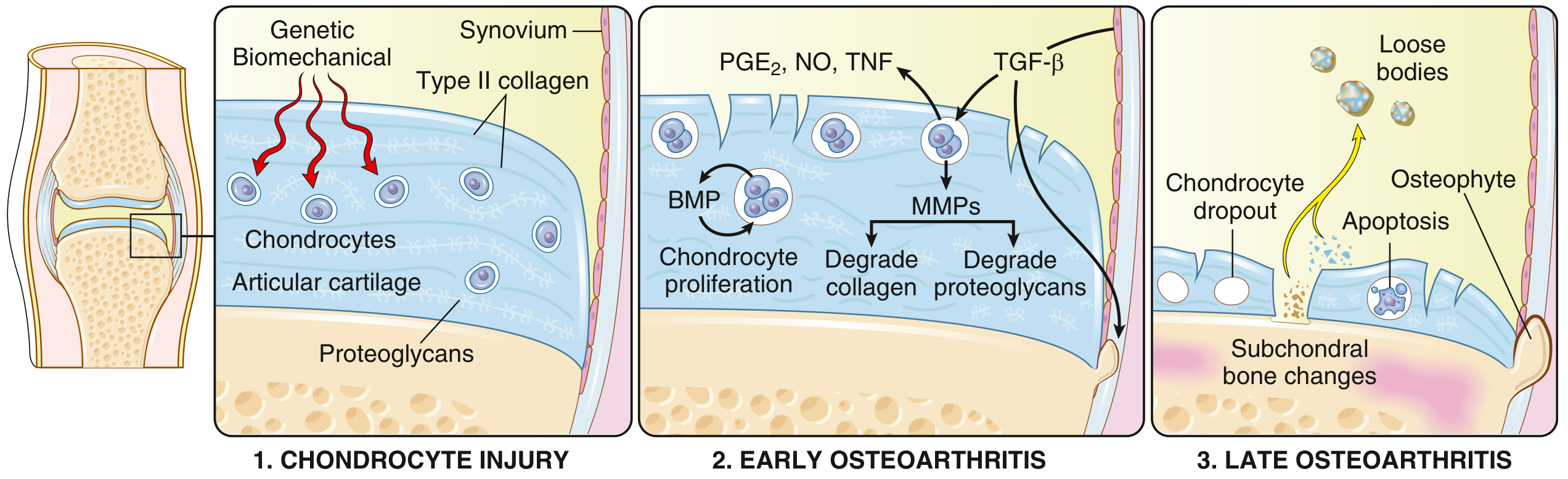
Fig. 19.31 - Schematic of OA progression (Robbins & Kumar Basic Pathology)
OA results from an imbalance between repair and destruction of joint tissues, driven by mechanical, inflammatory, and metabolic pathways:
Step 1 - Chondrocyte Injury:
Biomechanical stress is the principal mechanism. Genetic factors (polymorphisms in matrix components, signaling molecules) increase susceptibility. Initial injury affects the extracellular matrix of articular cartilage.
Step 2 - Early OA:
- Proteoglycan changes attract water → swelling of articular cartilage → disruption of the type II collagen matrix
- Chondrocytes proliferate and attempt repair but release destructive mediators: MMPs (degrade collagen and proteoglycans), PGE2, NO, TNF
- TGF-β and BMPs attempt counterregulation
- Surface erosions develop; deep cartilage fissures appear; the calcified cartilage zone expands
Step 3 - Late OA:
- Chondrocyte dropout (apoptosis) - repair fails to keep pace with destruction
- Full-thickness cartilage loss; subchondral bone changes (sclerosis, cysts)
- Osteophyte formation at joint margins
- Loose bodies shed into the joint space
- Robbins & Kumar Basic Pathology
Key genetic loci
- The best-investigated locus is GDF5 (chromosome 20), encoding a growth factor important in chondrogenesis and bone growth
- Other susceptibility genes: RUNX2, SMAD3, PTHLH - all involved in skeletal and bone development
- Large GWAS (>800,000 samples) identified >52 OA risk loci; Mendelian randomization confirmed a causative effect of BMI on OA risk
- Firestein & Kelley's Textbook of Rheumatology
OA vs. Rheumatoid Arthritis - Key Comparison
| Feature | Osteoarthritis | Rheumatoid Arthritis |
|---|---|---|
| Primary pathogenic abnormality | Mechanical injury to articular cartilage | Autoimmunity |
| Role of inflammation | Secondary; exacerbates cartilage damage | Primary - cartilage destroyed by T cells and antibodies |
| Joints involved | Weight-bearing (knees, hips) primarily | Often starts with small joints of fingers; multiple joints |
| Pathology | Cartilage degeneration, bone spurs, subchondral cysts; minimal inflammation | Inflammatory pannus; severe chronic inflammation; ankylosis |
| Serum antibodies | None | ACPA, rheumatoid factor |
| Extra-articular involvement | No | Yes (lungs, heart, other organs) |
- Robbins & Kumar Basic Pathology, Table 19.2
Clinical Features
- Pain: Use-related (worsens with activity, improves with rest); in advanced disease may be present at rest and at night
- Stiffness: Morning stiffness lasting <30 minutes (helps distinguish from RA where it lasts >1 hour)
- Functional disability: limitations in walking, stair climbing, sit-to-stand, balance
- Bony enlargement: Heberden's nodes (DIP joints), Bouchard's nodes (PIP joints) in hand OA
- Crepitus on joint movement
- Decreased range of motion
- Valgus/varus deformity in advanced knee OA
- Synovitis (joint effusion, warmth) can occur, especially during flares
Important: Structural pathology and imaging changes correlate poorly with pain intensity - pain in OA fits within a biopsychosocial model involving peripheral sensitization, spinal cord sensitization, altered cortical processing, and psychological factors.
Diagnosis
Diagnosis is primarily clinical, with little need for imaging or laboratory investigation in typical cases.
Clinical criteria for knee OA (ACR):
- Knee pain + at least 3 of: age >50, stiffness <30 min, crepitus, bony tenderness, bony enlargement, no palpable warmth
When to investigate:
- Atypical features (e.g., inflammatory signs suggesting another diagnosis)
- Young patient (rule out secondary causes)
- Rapid worsening of symptoms
Laboratory tests: Rheumatoid factor, synovial fluid analysis - to exclude inflammatory/infectious arthritis. No specific blood test for OA.
Holistic Assessment (Goldman-Cecil Table 241-1)
Assessment should cover:
- Social factors and impact on daily living
- Psychological factors (screen for depression)
- Attitudes to physical activity
- Pain assessment (nature, analgesic use)
- Functional capacity
- Comorbidities and fall risk
- Modifiable risk factors (obesity, joint alignment, injury)
Imaging
Plain Radiograph (Gold Standard for structural assessment)
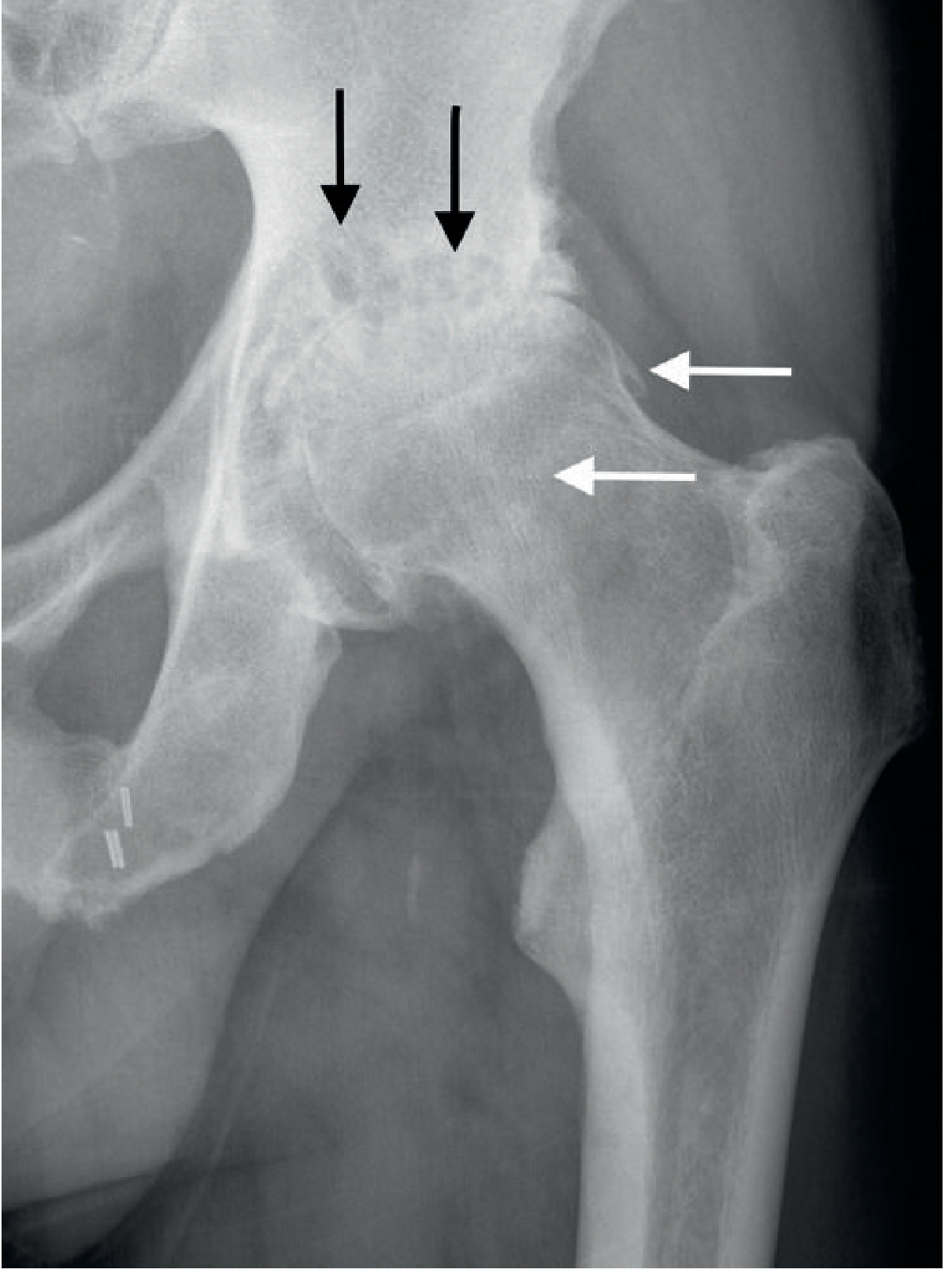
Fig. 44.7 - Severe hip OA. Note superior joint space narrowing (most common pattern), subchondral cysts (black arrows), and osteophytes (white arrows). (Grainger & Allison's Diagnostic Radiology)
The classic radiographic LOSS features:
- Joint space narrowing - asymmetric (in areas of stress), unlike the symmetric narrowing of RA
- Osteophytes - new bone formation at joint margins; represent the hypertrophic/reparative aspect
- Subchondral sclerosis - increased osteoblastic activity
- Subchondral cysts - synovial fluid tracking through damaged cartilage into bone
- Intra-articular loose bodies - shed cartilage/bone fragments; may proliferate
- Joint deformity and subluxation - from ligamentous laxity, bony collapse, and muscle weakness
MRI: Directly visualizes cartilage, bone marrow lesions, meniscal pathology, and synovitis - more sensitive for early changes.
- Grainger & Allison's Diagnostic Radiology
Management
Management should be individually tailored, focusing on core treatments. The framework is:
Non-pharmacological (First-line, core treatments)
| Intervention | Evidence |
|---|---|
| Exercise therapy (aerobic, strengthening, aquatic) | Strong evidence; comparable efficacy to NSAIDs and opioids for pain relief (network meta-analysis) |
| Weight loss (if overweight/obese) | Diet + exercise reduces knee pain (JAMA 2022 RCT); BMI is causatively linked to OA |
| Self-management education | Reduces pain and disability |
| Physical and occupational therapy | Restores functional status; critical component of care |
| Assistive devices | Walking aids, knee braces, orthotics |
Pharmacological
| Drug | Notes |
|---|---|
| Topical NSAIDs (e.g., diclofenac gel) | First-line for knee/hand OA; fewer systemic side effects |
| Oral NSAIDs | Effective; use at lowest effective dose due to GI/CV/renal risks |
| Paracetamol (acetaminophen) | Modest effect; safer than NSAIDs in many patients |
| Duloxetine | For central sensitization/widespread pain phenotype |
| Intra-articular corticosteroids | Short-term pain relief; physical therapy shown to be equally effective long-term (NEJM 2020) |
| Intra-articular hyaluronic acid (viscosupplementation) | Modest benefit; BMJ 2022 systematic review showed small effect |
| Intra-articular PRP | RESTORE trial (JAMA 2021) showed no significant benefit over placebo for pain or cartilage volume |
| Opioids | Only if other treatments fail; risk of dependence |
Surgical
-
Joint replacement (arthroplasty) - indicated when functional status interferes with activities of daily living and when supportive/pharmacological care is ineffective
-
Arthroscopy - NOT routinely recommended for OA; evidence does not support lavage or debridement
-
Goldman-Cecil Medicine, Grainger & Allison's Diagnostic Radiology
Risk Factors Summary
| Modifiable | Non-modifiable |
|---|---|
| Obesity/overweight | Age (>50 years) |
| Joint injury | Female sex |
| Occupational repetitive stress | Genetic predisposition (GDF5, RUNX2, etc.) |
| Muscle weakness | Prior joint deformity |
| Poor proprioception | Race/ethnicity |
Key Takeaways
- OA is the most common joint disease - >500 million people affected globally
- Primarily a mechanical/degenerative disease of cartilage with secondary inflammation
- Pain correlates poorly with structural damage - always assess the whole person (biopsychosocial model)
- Exercise and weight loss are the most evidence-supported treatments
- Radiographic hallmarks: asymmetric joint space narrowing, osteophytes, subchondral sclerosis/cysts
- Joint replacement is reserved for refractory cases with functional impairment
Sources: Goldman-Cecil Medicine International Edition, Robbins & Kumar Basic Pathology, Firestein & Kelley's Textbook of Rheumatology, Grainger & Allison's Diagnostic Radiology
This is a shared conversation. Sign in to Orris to start your own chat.