Anaesthesia topics
Asking for Preferences
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Here is a comprehensive overview of Anaesthesia Monitoring & Equipment, drawn from Miller's Anesthesia (10e), Morgan & Mikhail's Clinical Anesthesiology (7e), Barash's Clinical Anesthesia (9e), and Schwartz's Principles of Surgery (11e).
Anaesthesia Monitoring & Equipment
1. The Anaesthesia Workstation
The anaesthesia machine receives medical gases from a supply, controls flow and reduces pressure, vaporises volatile agents, and delivers the gas mixture to the patient's airway via a breathing circuit.
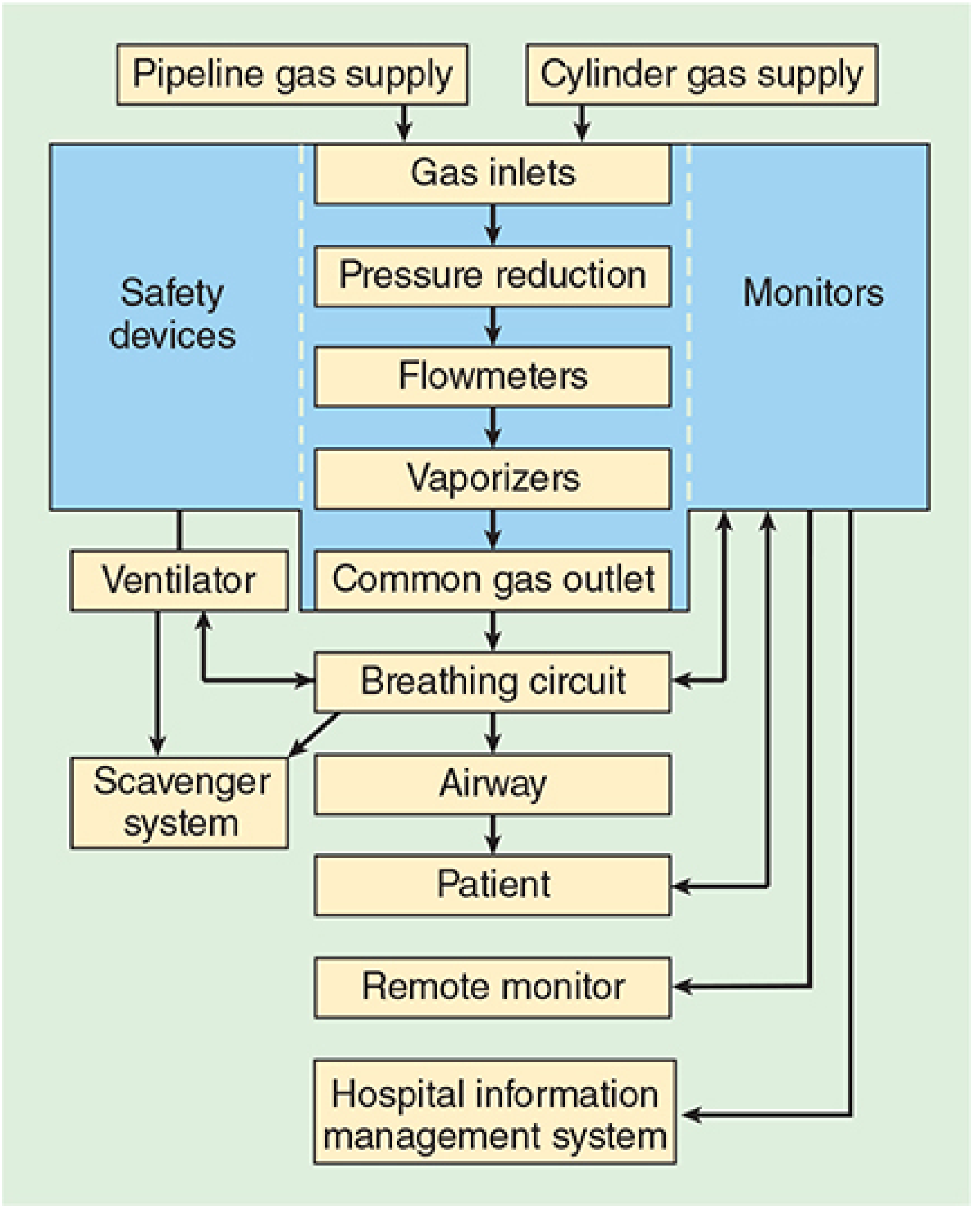
Functional schematic of the anaesthesia workstation — Morgan & Mikhail's Clinical Anesthesiology, 7e
Essential Safety Features (ASTM F1850 Standards)
| Feature | Purpose |
|---|---|
| DISS fittings (non-interchangeable pipeline inlets) | Prevent incorrect gas pipeline connections |
| Pin Index Safety System (cylinders) | Prevent wrong cylinder attachment |
| Low O₂ pressure alarm | Detect oxygen supply failure |
| Hypoxic guard (min O₂/N₂O ratio controller) | Prevent delivery of <21% O₂ |
| O₂ failure safety device | Shuts off N₂O if O₂ fails |
| Vaporiser interlock | Prevents simultaneous delivery of >1 volatile agent |
| Capnography + anaesthetic gas measurement | Guides ventilation; prevents overdose; reduces awareness |
| Breathing circuit pressure monitor + alarm | Prevents barotrauma; detects disconnection |
| Exhaled volume monitor | Prevents hypo-/hyperventilation |
Gas Supply
- Pipeline: ~50 psig, colour-coded, DISS fittings
- Cylinders (backup): E-cylinders at 45 psig; O₂ = 1900 psig full (600 L); N₂O = 745 psig full (1590 L)
- Colour codes (North America): O₂ = green; N₂O = blue; CO₂ = grey; Air = yellow; He = brown; N₂ = black
2. ASA Standards for Basic Intraoperative Monitoring
Standard 1: Qualified anaesthesia personnel present throughout.
Standard 2: Continuous evaluation of four domains:
| Domain | Monitors Required |
|---|---|
| Oxygenation | Inspired O₂ analyser, pulse oximetry, clinical observation |
| Ventilation | Auscultation, observation of chest/reservoir bag, end-tidal CO₂ (ETCO₂) |
| Circulation | Continuous ECG, NIBP every ≤5 minutes, pulse assessment |
| Temperature | Core (oesophageal/nasopharyngeal) or skin probe |
3. Key Monitors — Functions & Details
Pulse Oximetry (SpO₂)
- Non-invasive, continuous measure of arterial O₂ saturation
- Uses differential light absorption of oxyhaemoglobin vs deoxyhaemoglobin at 660 nm and 940 nm
- Limitations: inaccurate with motion, poor perfusion, methaemoglobinaemia, carboxyhaemoglobinaemia
Capnography (ETCO₂)
- Monitors exhaled CO₂ waveform continuously
- Confirms endotracheal intubation (gold standard alongside direct visualisation)
- ETCO₂ ≈ PaCO₂ − 2–5 mmHg in normal lungs (gradient increases with V/Q mismatch)
- During CPR: sudden rise in ETCO₂ signals return of spontaneous circulation (ROSC)
- Also detects oesophageal intubation, apnoea, air embolism, malignant hyperthermia (sudden rise)
ECG
- Continuous display; detects arrhythmias, ischaemia (ST changes), and rate
- Lead II: best for arrhythmia detection (P-wave visibility)
- Lead V5: most sensitive for detecting left ventricular ischaemia
Non-Invasive Blood Pressure (NIBP)
- Oscillometric method; recorded at minimum every 5 minutes per ASA standards
Arterial Line (Invasive BP)
- Indications: haemodynamically unstable patients, major surgery (cardiac, thoracic, vascular), frequent ABG sampling
- Provides beat-to-beat BP and access for blood gas analysis
- Radial artery is the most common site
Temperature
- Core temperature via oesophageal probe (most accurate intraoperatively) or nasopharyngeal probe
- Bladder (Foley) catheter with temperature sensor for core measurement
- Prevents undetected hypothermia or malignant hyperthermia (rapid rise)
4. Depth of Anaesthesia Monitoring
Awareness under general anaesthesia affects approximately 1–2 per 1000 patients. Several EEG-based monitors have been developed:
| Monitor | Signal Used | Target Range | Principle |
|---|---|---|---|
| BIS (Bispectral Index) | 1-channel EEG | 40–60 | Weighted sum: α/β ratio, bicoherence, burst suppression |
| Patient State Index (PSI) | 4-channel EEG | 25–50 | Discriminant analysis of power spectrum, hemispheric symmetry |
| Narcotrend Index (NI) | EEG | — | Pattern classification A–F |
| ETAG (end-tidal anaesthetic gas) | Volatile agent concentration | MAC >0.7 | Pharmacodynamic proxy |
Note: A landmark RCT of >6,000 patients (B-Aware trial) showed BIS-guided anaesthesia was not superior to titrating depth using end-tidal anaesthetic gas concentration (MAC >0.7) for preventing awareness. — Schwartz's Principles of Surgery, 11e
As anaesthesia deepens: beta activation → slowing → burst suppression → isoelectricity.
5. Neuromuscular Blockade Monitoring
Train-of-Four (TOF) stimulation: four successive stimuli at 2 Hz over 2 seconds applied (typically) to the ulnar nerve, observing adductor pollicis.
| TOF Findings | Interpretation |
|---|---|
| 4 twitches, no fade, T4/T1 ratio ≥ 0.9 | Adequate reversal — safe for extubation |
| 2–3 twitches | ~75–80% receptor occupancy — sufficient for abdominal/thoracic relaxation |
| 0–1 twitches | Deep block |
| Phase I succinylcholine block | No fade; no posttetanic potentiation |
| Phase II block (prolonged sux) | Resembles non-depolarising block (fade present) |
Objective monitoring (acceleromyography) is preferred over subjective methods. A 2018 consensus statement recommends documenting a TOF ratio ≥ 0.90 as the only reliable indicator of safe recovery from neuromuscular blockade. — Morgan & Mikhail's, 7e
6. Advanced Haemodynamic Monitoring
| Monitor | Use Case | Notes |
|---|---|---|
| Central Venous Pressure (CVP) | Volume status, RV preload | Via internal jugular or subclavian; risk of pneumothorax, infection |
| Pulmonary Artery Catheter (PAC) | Complex cardiac cases, pulmonary hypertension | Measures PCWP, CO, mixed venous O₂ saturation |
| Transoesophageal Echocardiography (TEE) | Cardiac surgery, haemodynamic instability | Assesses myocardial function, volume status, valvular disease; also guides valve replacement surgery |
7. PACU Monitoring (Post-Anaesthesia Care Unit)
Mandatory monitoring in PACU per Morgan & Mikhail includes:
- SpO₂ (pulse oximetry)
- ECG
- Automated NIBP
- Respiratory rate and airway patency
- Capnography where available
Summary: Monitor Types at a Glance
| Monitor | What is Measured | Invasiveness | Complication Risk |
|---|---|---|---|
| Pulse oximetry | Arterial O₂ saturation | Non-invasive | None |
| Capnography | Ventilatory/circulatory status | Non-invasive | None |
| ECG | Cardiac rhythm, rate, ischaemia | Non-invasive | None |
| NIBP | Blood pressure | Non-invasive | Minimal |
| Arterial catheter | Continuous BP + ABG | Invasive | ++ |
| BIS / EEG-based | Depth of anaesthesia | Non-invasive | Minimal |
| Temperature probe | Core body temp | Minimally invasive | Minimal |
| CVP / PA catheter | Cardiac function, filling pressures | Invasive | +++ |
| TEE | Cardiac function, volume status | Invasive | +++ |
| TOF / nerve stimulator | Neuromuscular blockade depth | Non-invasive | None |
— Adapted from Schwartz's Principles of Surgery, 11e (Table 46-3)
Sources: Morgan & Mikhail's Clinical Anesthesiology, 7e | Miller's Anesthesia, 10e | Barash's Clinical Anesthesia, 9e | Schwartz's Principles of Surgery, 11e
Would you like to go deeper into any specific area — e.g., the anaesthesia machine gas circuits, vaporisers, breathing circuits, specific advanced monitors, or equipment for airway management?
This is a shared conversation. Sign in to Orris to start your own chat.