PVD
"peripheral vascular disease"[MeSH Terms] AND management
Peripheral Vascular Disease (PVD)
Definition
- Goldman-Cecil Medicine, Chapter 65
Epidemiology
- Prevalence in adults aged 40+ years: ~4.3%; rises to 14.5% in those aged 70+
- Affects approximately 4 million Americans over age 70
- Prevalence in patients with diabetes: 20-30%
- Disproportionately affects older adults, non-Hispanic Blacks, smokers, diabetics, and those with renal dysfunction
- Over 1/3 of PAD patients have significant concomitant coronary artery disease; up to 1/4 have carotid artery disease
Risk Factors
| Risk Factor | Notes |
|---|---|
| Cigarette smoking | 2-3x more likely to cause PAD than CAD; accounts for ~50% of all cases |
| Diabetes mellitus | 2-4x increased risk; risk rises 28% per 1% increase in HbA1c |
| Hypertension | Independent risk factor |
| Dyslipidemia | Risk rises 5-10% per 10 mg/dL increase in total cholesterol |
| Elevated homocysteine | 2-3x increased risk |
| Age, family history, CKD | Additional factors |
- Age ≥65 years
- Age 50-64 with atherosclerotic risk factors or family history
- Age <50 with diabetes + 1 additional risk factor
- Known atherosclerosis in another vascular bed (coronary, carotid, renal, mesenteric, or AAA)
Pathophysiology
- Chronic stable ischemia (claudication) - reversible ischemia during exertion
- Critical limb-threatening ischemia (CLTI) - inadequate resting perfusion; tissue viability at risk
- Acute limb ischemia (ALI) - abrupt cessation of flow, limb-threatening emergency
Clinical Manifestations
Intermittent Claudication (Chronic Stable)
- Reproducible muscle pain, cramping, or fatigue with walking that resolves with rest (typically within 10 minutes)
- Most commonly affects the calf (superficial femoral artery disease), thigh/buttock (iliac disease)
- Note: Patients with diabetes may have minimal symptoms due to concomitant neuropathy
Critical Limb-Threatening Ischemia
- Rest pain - typically in the forefoot, worse at night, partially relieved by dependency
- Tissue loss - non-healing ulcers, gangrene
Acute Limb Ischemia - "The 6 P's"
- Pain, Pallor, Pulselessness, Paresthesias, Poikilothermia (coolness), Paralysis
- Paralysis is a late, ominous sign indicating advanced ischemia - requires urgent revascularization
- Motor deficits progress distal to proximal; complete paralysis can indicate irreversible injury
Physical Examination Findings
- Diminished or absent pulses
- Dependent rubor; pallor on leg elevation
- Absent hair growth on lower limbs
- Dystrophic toenails
- Cool, dry, fissured skin
Diagnosis
Ankle-Brachial Index (ABI)
| ABI Value | Interpretation |
|---|---|
| >0.90 | Normal |
| 0.71-0.90 | Mild obstruction |
| 0.41-0.70 | Moderate obstruction |
| 0.00-0.40 | Severe obstruction |
- Sensitivity: 95% for angiogram-positive PAD
- ABI >1.30-1.40 suggests vessel non-compressibility (calcification in diabetics/elderly) - toe-brachial index preferred in this case
Additional Tests
- Segmental limb pressures and pulse volume recordings - localize stenosis level
- Duplex ultrasound - assess anatomy and flow velocities
- CT angiography / MR angiography - detailed vascular mapping before revascularization
- Conventional angiography - gold standard when intervention planned
Management
1. Cardiovascular Risk Reduction (Primary for ALL patients)
- Statins - LDL-C reduction is mandatory; target LDL <70 mg/dL in high-risk patients
- Antiplatelet therapy - aspirin (75-325 mg/day) or clopidogrel 75 mg/day (preferred in PAD patients, especially those with diabetes)
- ACE inhibitors/ARBs - reduce CV events independent of BP effect
- Smoking cessation - single most impactful intervention; significantly reduces failure rates of bypass surgery
- Tight glycemic control - every 1% rise in HbA1c increases PAD risk by 28%
- BP control - target <130/80 mmHg
2. Symptom Management for Claudication
- Supervised exercise rehabilitation - structured walking programs are first-line; improve walking distance and quality of life
- Cilostazol 100 mg BID - phosphodiesterase-3 inhibitor; improves claudication distance; contraindicated in heart failure
- Pentoxifylline - less effective; second-line option
3. Revascularization
- Endovascular (preferred first-line where anatomy permits): percutaneous transluminal angioplasty (PTA) ± stenting
- Surgical bypass: autologous vein graft preferred for below-knee disease; synthetic grafts for above-knee
- Hybrid procedures may combine both
- PVD with or without diabetes is the most common indication for amputation; diabetics with PAD are 7-15x more likely to require major amputation than non-diabetics
4. Acute Limb Ischemia (Emergency)
- Immediate anticoagulation with unfractionated heparin
- Urgent vascular surgery consultation
- Options: catheter-directed thrombolysis, surgical embolectomy, or bypass
- Paralysis = irreversible ischemia looming; act before this stage
Prognosis
- Risk of MI, stroke, and death are increased several-fold vs. those without PAD
- Diabetics with PAD: annual major amputation risk up to 15x that of non-diabetics
- With aggressive medical management, the 5-year mortality is approximately 15-30%, mostly from cardiovascular events
- Goldman-Cecil Medicine, Chapter 65 (Atherosclerotic Peripheral Arterial Disease)
- Washington Manual of Medical Therapeutics (PVD in Diabetes)
- Grainger & Allison's Diagnostic Radiology, Chapter 77
- Textbook of Family Medicine, 9e (Smoking and PVD)
TB cervical lymphadentis
"tuberculous lymphadenitis"[MeSH Terms] AND cervical
Tuberculous Cervical Lymphadenitis (Scrofula)
Definition & Overview
Epidemiology
- Most common in children, adolescents, and young adults; slight female predominance
- Highly prevalent in the Indian subcontinent, sub-Saharan Africa, Southeast Asia
- Risk groups: recent immigrants from endemic areas, HIV-infected individuals, immunocompromised patients
- A young person from an endemic area presenting with cervical lymphadenopathy should be presumed to have TB lymphadenitis until proven otherwise
- HIV co-infection increases the likelihood of TB (vs. NTM) lymphadenitis
Pathology and Stages (S Das Classification)
| Stage | Features |
|---|---|
| Stage 1 - Lymphadenoid | Simple enlargement without matting; difficult to distinguish from chronic septic lymphadenitis |
| Stage 2 - Periadenitis / Matting | Enlarged nodes become adherent to each other (matted); most characteristic feature of TB lymphadenitis |
| Stage 3 - Caseation / Cold abscess | Nodes soften due to caseation necrosis; forms a cold abscess; eventually bursts through fascia |
- A TB sinus - non-healing, discharging pus
- A TB ulcer - watery discharge with characteristic undermined (overhanging) edges (bacilli destroy subcutaneous tissue faster than the skin above)
Clinical Features
Nodes Involved (in order of frequency)
- Jugulodigastric
- Submandibular
- Supraclavicular (posterior cervical)
- Posterior triangle
- Mediastinal, mesenteric, axillary, and inguinal nodes may also be involved
Local Features
- Painless cervical lymphadenopathy - the hallmark
- Matted nodal mass (most characteristic)
- Cold abscess: fluctuant, not warm, no signs of acute inflammation (no redness, no warmth) - reflects underlying caseation
- Collar-stud abscess in late stages
- Sinus/ulcer formation with undermined edges if untreated
Systemic Features
- Evening pyrexia (afternoon/evening low-grade fever)
- Malaise and weight loss
- Night sweats
- Cough (if concurrent pulmonary TB)
- Failure to thrive (in children)
Clinical Images


Investigations
Blood Tests
- Raised ESR and CRP
- Low haemoglobin (anaemia of chronic disease)
- Lymphocytosis
Immunological Tests
- Tuberculin skin test (TST/Mantoux): Positive in most cases, but of limited value in patients from endemic areas (may reflect past exposure/BCG vaccination)
- Interferon-gamma release assays (IGRAs - e.g. QuantiFERON-TB Gold, T-SPOT.TB): Now supersede the Mantoux test; in vitro blood test measuring T-cell IFN-gamma release in response to M. tuberculosis-specific antigens; helps identify latent or subclinical TB; not confounded by BCG vaccination
Microbiological
- Aspiration of pus from cold abscess for:
- Culture and sensitivity (takes weeks)
- Ziehl-Neelsen (ZN) stain for acid-fast bacilli (AFB) - faster result
- FNAC (Fine Needle Aspiration Cytology): First-line minimally invasive test; shows caseating granulomas with Langhans giant cells and epithelioid histiocytes
- Sputum for AFB smear and culture (even without respiratory symptoms)
Tissue Diagnosis
- Excision biopsy: If mass is in early stage (no fluctuation); specimen should be sent fresh and unfixed immediately for mycobacterial culture (lab must be pre-warned)
- Histology: caseating granulomas with Langhans-type multinucleated giant cells, epithelioid cells, and central necrosis
Molecular
- GeneXpert MTB/RIF (Xpert): Rapid PCR-based detection of M. tuberculosis and rifampicin resistance directly from aspirated material or biopsy; increasingly used as first-line diagnostic
Imaging
- CXR: to identify concurrent pulmonary TB (present in up to 50%)
- Ultrasound neck: characterize node consistency, guide aspiration
- CT neck: assess extent, collar-stud anatomy, compressive effects
Differential Diagnosis
| Condition | Distinguishing Features |
|---|---|
| Chronic non-specific lymphadenitis | History of acute episode; oral sepsis source; nodes elastic, mildly tender - early TB impossible to distinguish clinically |
| Lymphoma | Firm, rubbery nodes; systemic B symptoms; no cold abscess; FNAC/biopsy diagnostic |
| Metastatic carcinoma | Hard, fixed nodes; primary tumor identifiable; older age group |
| NTM lymphadenitis | Clinically identical; violaceous overlying skin; treatment is surgical excision (not anti-TB drugs) |
| Cat-scratch disease (Bartonella henselae) | History of cat scratch; inoculation site; serology positive |
| Infectious mononucleosis (EBV) | Painful nodes; pharyngitis, splenomegaly; positive monospot |
| Syphilitic lymphadenitis | Painless, discrete, firm, shotty; no suppuration; genital chancre; RPR/VDRL positive |
| Actinomycosis | Woody-hard induration; "sulfur granules" in pus |
Treatment
Medical (Mainstay)
- Intensive phase (2 months): HRZE - Isoniazid (H) + Rifampicin (R) + Pyrazinamide (Z) + Ethambutol (E) daily
- Continuation phase (4 months): HR - Isoniazid + Rifampicin daily
- Total duration: 6 months for most extrapulmonary TB including lymphadenitis
- Duration extends to 8-12 months if treatment for non-TB mycobacteria (M. tuberculosis lymphadenitis treated 8-12 months per Tintinalli)
- In HIV co-infected patients: continuation phase extended to 7 months (total 9 months)
Surgical
- Aspiration of cold abscess: Diagnostic and therapeutic; repeat aspirations may be needed
- Excision biopsy: For diagnosis when nodes are firm (not fluctuant); avoid incision and drainage of intact nodes (risks sinus formation)
- Excision of sinus tract: Once infection is controlled medically
- Incision and drainage is generally avoided as it promotes non-healing sinus tract formation
- NTM lymphadenitis: Surgical excision is the treatment of choice (anti-TB drugs are largely ineffective)
Always exclude and treat TB at other sites before completing management.
Complications
- Chronic non-healing sinus
- Disfiguring scarring
- Collar-stud abscess formation
- Upper airway obstruction (large intrathoracic/cervical nodes)
- Treatment failure / drug resistance (MDR-TB)
- Paradoxical reaction during treatment
- Bailey & Love's Short Practice of Surgery, 28th Ed., Chapter 6
- Goldman-Cecil Medicine, Chapter on Extrapulmonary TB
- Harrison's Principles of Internal Medicine, 22nd Ed., Chapter 186
- Tintinalli's Emergency Medicine (Mycobacterial Lymphadenitis)
- S Das - Manual on Clinical Surgery, 13th Ed.
Fibroadenous breast
"fibroadenoma"[MeSH Terms] AND breast
Fibroadenous / Benign Breast Disease
ANDI Framework (Aberrations of Normal Development and Involution)
| Phase | Age Range | Normal Process | Aberration | Disease |
|---|---|---|---|---|
| Lobular development | 15-25 yr | Lobule formation | Lobular hyperplasia | Fibroadenoma |
| Cyclical changes | 15-50 yr | Hormonal cycling | Exaggerated response | Cyclical mastalgia, diffuse nodularity |
| Involution | 35-55 yr | Lobular involution | Cyst formation; sclerosing adenosis | Breast cysts, sclerosing adenosis |
Part 1: Fibroadenoma
Definition
Histological Types
| Type | Histology | Age | Size/Consistency |
|---|---|---|---|
| Pericanalicular | Fibrous tissue surrounding small tubular glands | 15-30 yr | Smaller, hard |
| Intracanalicular | Glands stretched into elongated spidery shapes, indented by fibrous tissue | 35-50 yr | Larger, comparatively soft |
Clinical Features
- Painless breast lump - the hallmark
- Slow-growing; may remain stable in size for years
- More often in the lower half of the breast (though can occur anywhere)
- On examination:
- Smooth, firm, well-defined margin
- Not fixed to skin or deep structures
- Highly mobile - "slips away" from fingers - hence called a "breast mouse" or "floating tumour"
- Not tender, no local warmth
- Axillary nodes not enlarged
Special Variants
-
5 cm diameter; occurs during puberty; rapidly growing
- Difficult to distinguish from phyllodes tumor - excision recommended
- Can be enucleated through a submammary (inframammary) incision
- Young women; may grow rapidly; excision recommended as hard to distinguish from phyllodes
- Contains cysts >3mm, sclerosing adenosis, epithelial calcifications, or papillary apocrine change
- Higher malignancy risk (see below)
Malignant Potential (Relative Risk for Cancer)
| Type | Relative Risk |
|---|---|
| Simple fibroadenoma | 1.5-1.7x |
| Fibroadenoma + epithelial hyperplasia | 3.4-3.7x |
| Complex fibroadenoma + family history of breast cancer | 3.0-4.0x (especially lobular carcinoma) |
Investigations (Triple Assessment)
- Clinical examination
- Imaging:
- Ultrasound (USG) - first-line in women <35 years; shows well-defined, homogenous, hypoechoic oval mass with gentle lobulations
- Mammography - in women >35 years (dense breast tissue limits its use in young women)
- A clinically typical fibroadenoma confirmed on USG may be observed without biopsy in women under 25
- Tissue diagnosis:
- FNAC (Fine Needle Aspiration Cytology) - rapid, minimally invasive
- Core needle biopsy - if atypical features or age >25
- Biopsy should be obtained if the patient is >25 years or if there are atypical USG features
Management
- Clinically typical fibroadenoma in women <25 with characteristic USG features
- Most fibroadenomas remain stable or regress spontaneously (particularly in postmenopausal women)
- Tamoxifen and ormeloxifene (selective estrogen receptor modulators) have shown regression in some studies
- Age >30 years
- Suspicious features on imaging (e.g., microlobulation)
- Atypia on histology/cytology
- Size >5 cm (giant fibroadenoma)
- Family history of breast cancer
- Patient's preference or significant anxiety
- Excision in elderly patients should include a rim of normal tissue as it may harbor malignancy or phyllodes tumor
- Vacuum-assisted excision (8G/11G needles) - effective for benign lumps including fibroadenoma
- Ultrasound-guided high-intensity focused ultrasound (HIFU) - recent systematic review (2024, PMID 39053900) supports its safety and efficacy
- Cryoablation - systematic review (2025, PMID 41061430) shows it as an effective non-surgical option for fibroadenoma management
Part 2: Fibrocystic Change (Fibroadenosis / ANDI)
Overview
Pathological Components
| Lesion | Risk of Cancer |
|---|---|
| Nonproliferative lesions (cysts, mild hyperplasia, apocrine change) | No increased risk |
| Proliferative without atypia (moderate/florid hyperplasia, sclerosing adenosis, fibroadenoma, papilloma) | 1.5-2x increased risk |
| Atypical ductal hyperplasia (ADH) | 4-5x increased risk |
| Atypical lobular hyperplasia (ALH) | 4-5x increased risk |
| ADH/ALH + family history of breast cancer | 8-10x increased risk |
Breast Cysts
- Most common nonproliferative lesion
- Arise from the TDLU when fluid accumulates due to distension/obstruction of ductules
- Peak incidence age 35-50 years
- Present as solitary, fluctuant masses; blue-domed cyst of Bloodgood (when superficial and tense)
- Simple cyst: Anechoic, posterior acoustic enhancement, no solid components - benign, no intervention needed unless symptomatic
- Complicated cyst: Low-level internal echoes, no solid components - <1% malignancy risk; aspiration/biopsy or 6-monthly follow-up
- Complex cyst: Solid components, thick walls/septa - 1-23% malignancy risk; biopsy mandatory
Clinical Features of Fibrocystic Change
- Mastalgia (50-70% of breast clinic attendees): breast pain, usually cyclical
- Diffuse nodularity: bilateral, upper outer quadrant predominance; rubbery/firm texture
- Nodules better palpated with fingers and thumb (not palmar surface)
- Not fixed to skin or pectoralis fascia
- Axillary nodes may be slightly enlarged and tender
- Possible green or serous nipple discharge
Mastalgia
- Starts day 14, worsens until day 27-28, relieved by onset of menses
- Usually bilateral; may radiate to upper arm (can mimic angina)
- Cause is unclear - hormonal imbalance, dietary factors not consistently proven
- No relationship to menstrual cycle; may be unilateral
- Causes: chest wall musculoskeletal pain (Tietze's syndrome), referred pain
- Evening primrose oil (gamma-linolenic acid) - mild effect, first-line in many guidelines
- Danazol (weak androgen) - most effective; side effects limit long-term use
- Bromocriptine - reduces prolactin; effective but side effects common
- Tamoxifen - effective; used in severe cases
- Topical NSAIDs - for non-cyclical mastalgia
- GnRH analogues - no established role in fibrocystic disease
Part 3: Phyllodes Tumor (Related Entity)

- Previously called cystosarcoma phyllodes
- True mixed neoplasm (epithelial + mesenchymal); resembles fibroadenoma histologically but larger
- Age group: usually >30 years; can be massive
- Mobile on chest wall (despite size); rarely infiltrates skin until late
- Overlying skin may ulcerate from pressure necrosis
| Grade | Mitotic Rate | Behavior |
|---|---|---|
| Benign | <4 per 10 HPF | Low recurrence |
| Borderline | 4-9 per 10 HPF | Intermediate |
| Malignant | >10 per 10 HPF | May metastasize via bloodstream |
Differential Diagnosis of a Breast Lump
| Feature | Fibroadenoma | Fibrocystic | Carcinoma | Phyllodes |
|---|---|---|---|---|
| Age | 15-25 yr | 35-50 yr | >40 yr | >30 yr |
| Pain | Painless | Cyclical pain | Painless | Painless |
| Consistency | Firm, smooth | Rubbery, nodular | Stony hard, irregular | Bosselated |
| Mobility | Very mobile (breast mouse) | Mobile | Fixed (late) | Mobile |
| Skin/nipple changes | None | None | Dimpling, peau d'orange | Late ulceration |
| Axillary nodes | Normal | Occasionally enlarged | Enlarged (late) | Normal |
- Bailey & Love's Short Practice of Surgery, 28th Ed., Chapter 58 (Benign Breast Disease, Fibroadenoma, Phyllodes)
- S Das - Manual on Clinical Surgery, 13th Ed. (Breast Tumors)
- Mulholland & Greenfield's Surgery, 7th Ed. (Proliferative Breast Lesions)
- Recent PubMed: HIFU for fibroadenoma [PMID 39053900]; Cryoablation [PMID 41061430]
Congenital hydrocephalus
"hydrocephalus"[MeSH Terms] AND congenital
Congenital Hydrocephalus
Definition
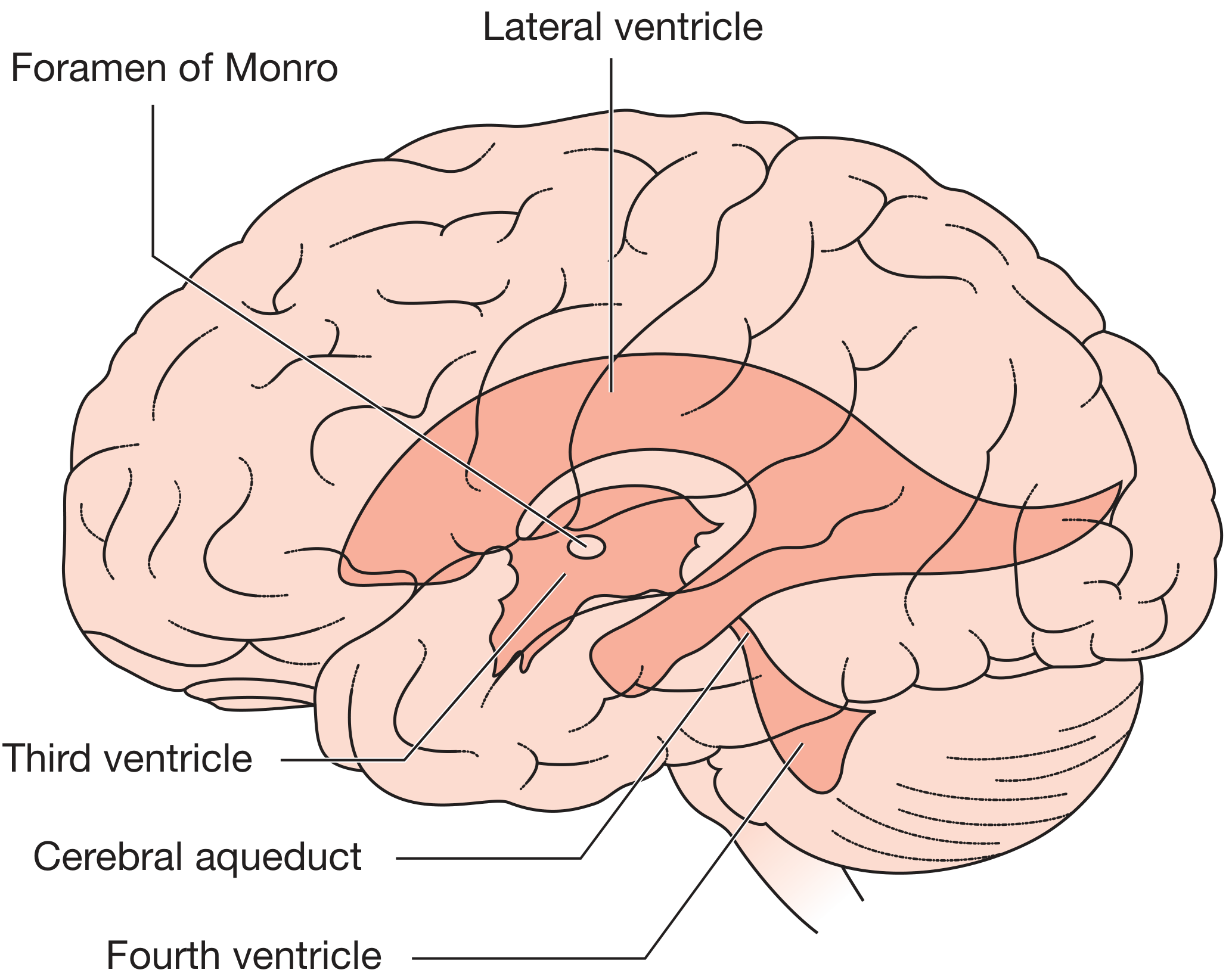
CSF Physiology (Essential Background)
Classification
1. Non-Communicating (Obstructive) Hydrocephalus
- Obstruction lies within the ventricular system - ventricles proximal to the block enlarge, distal ones remain normal
- Most common form in congenital disease
- Causes: aqueductal stenosis (most common), Chiari II malformation, Dandy-Walker malformation, colloid cysts, tumors at foramina of Monro, tectal plate gliomas
- LP is dangerous - risk of transtentorial herniation ("coning") due to differential pressure
2. Communicating (Non-Obstructive) Hydrocephalus
- Obstruction is outside the ventricular system - entire ventricular system enlarged; CSF can still exit ventricles but fails to be reabsorbed
- Ventricular system remains in continuity with subarachnoid space
- Causes: post-hemorrhagic (germinal matrix hemorrhage in prematurity), post-infective (bacterial meningitis causing arachnoid fibrosis), raised CSF protein
- LP is diagnostic (measures opening pressure) and therapeutic
3. Hydrocephalus Ex Vacuo
- Compensatory increase in CSF volume secondary to loss of brain parenchyma (infarction, neurodegeneration)
- NOT true hydrocephalus - normal or low ICP; no treatment required
4. Overproduction (Very Rare)
- Choroid plexus papilloma/carcinoma - excessive CSF production
Etiology of Congenital Hydrocephalus
| Category | Specific Cause |
|---|---|
| Aqueductal stenosis | Most common cause; may be developmental or acquired via fetal CMV/toxoplasma; rarely X-linked recessive |
| Chiari II malformation | Hindbrain herniation; almost universal after repair of lumbosacral myelomeningocele |
| Dandy-Walker malformation | Cystic expansion of 4th ventricle, hypoplasia of cerebellar vermis, posterior fossa enlargement |
| Post-hemorrhagic | Germinal matrix hemorrhage in preterm infants → arachnoid fibrosis |
| Post-infective | Congenital TORCH infections; neonatal meningitis |
| Vein of Galen malformation | High-flow AV fistula causing venous hypertension |
| Midline tumors | Rare congenital masses at foramina of Monro |
| Failure of arachnoid villi development | Impaired absorption pathway from birth |
Pathological Changes
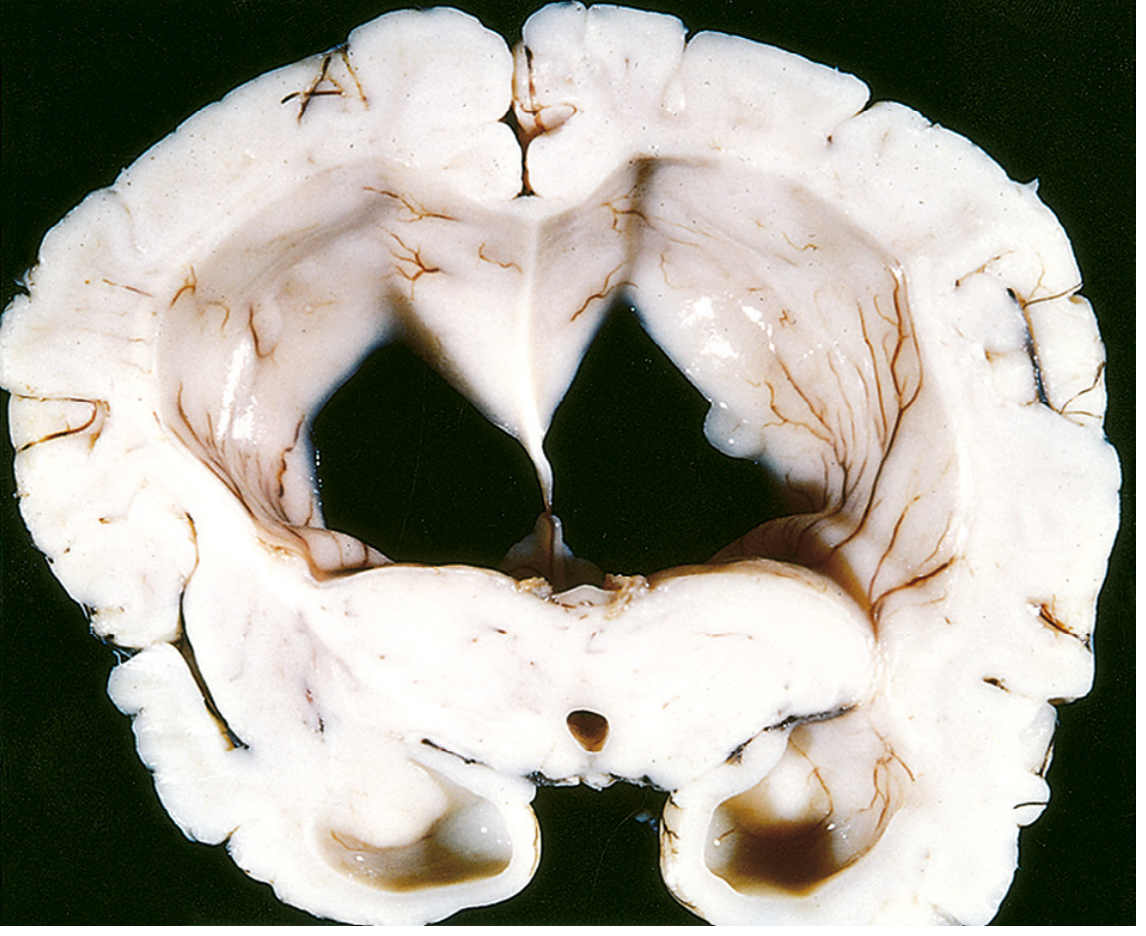
- Expansion of ventricles proximal to obstruction
- Thinning of cerebral cortex and white matter (atrophy)
- Transependymal (periventricular) edema - CSF seeps through ependyma into adjacent white matter
- Compression of basal ganglia and diencephalon
- Before suture fusion (infants <2 years): skull expands, sutures widen - head enlarges
- After suture fusion (older children/adults): skull cannot expand - ICP rises without head enlargement
Clinical Features
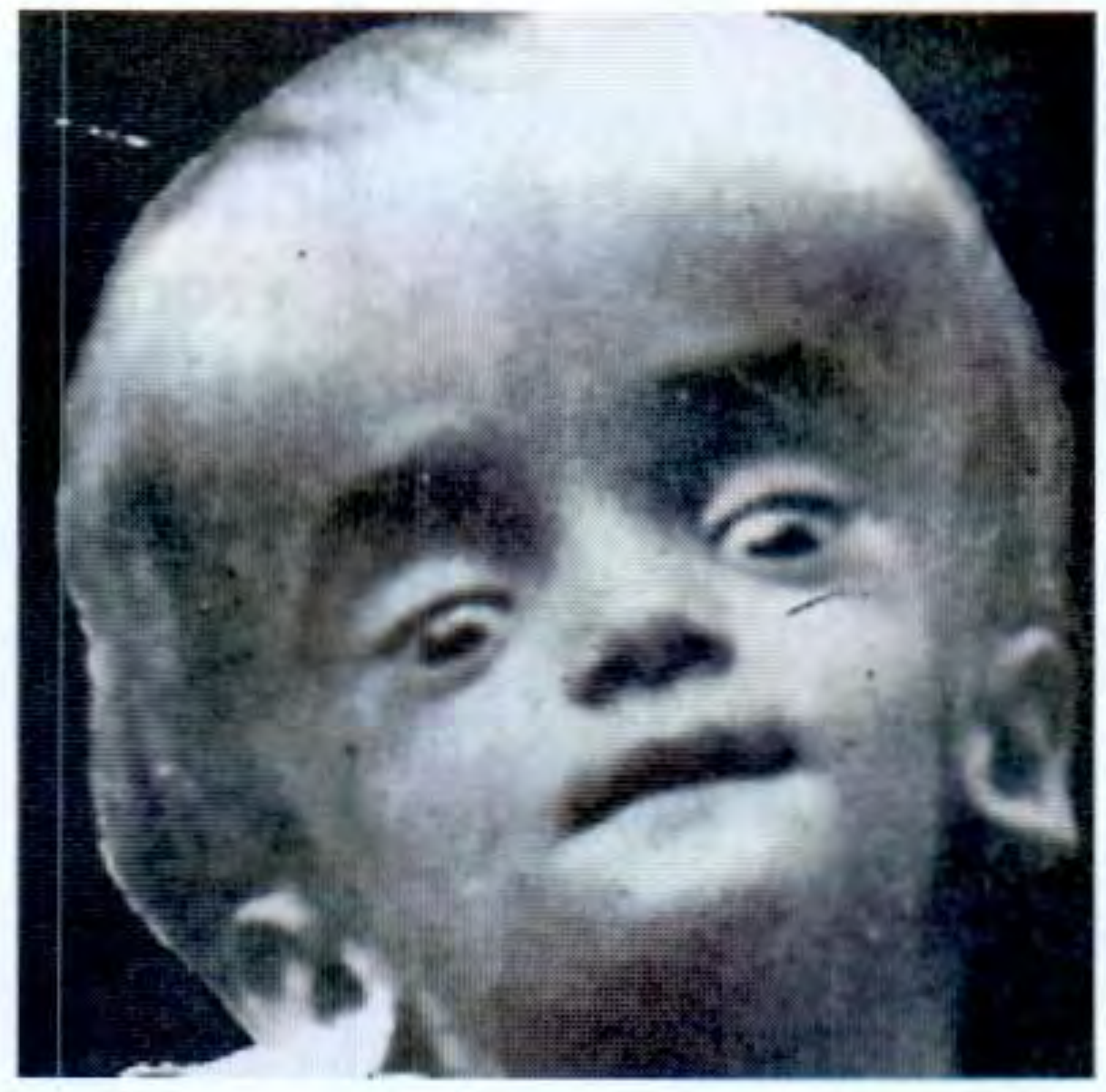
In Infants (Before Fontanelle Closure - up to ~2 years)
| Sign | Description |
|---|---|
| Macrocephaly | Most reliable sign - progressive increase in head circumference crossing centiles on growth charts; serial measurements essential |
| Frontal bossing | Prominence of the forehead |
| Tense, bulging anterior fontanelle | Non-pulsatile, full fontanelle at rest |
| Sutural diastasis | Widened cranial sutures visible/palpable |
| Scalp vein enlargement | Dilated scalp veins from obstructed venous drainage |
| Calvarial thinning | "Copper-beaten" skull on X-ray in chronic cases |
| "Sunset sign" | Eyes deviated downward with failure of upward gaze; upper sclera visible (Parinaud-like from tectal compression) |
| Lateral rectus palsy (VI nerve) | Stretching of abducens - false localizing sign |
| Leg spasticity | Stretching of corticospinal tracts around dilated ventricles |
| Irritability, poor feeding, vomiting | Non-specific signs of raised ICP |
| "Cracked pot" (Macewen's) sign | Resonant note on skull percussion from separated sutures |
In Older Children (After Suture Fusion)
- Early morning headache - worse on waking, Valsalva, lying flat
- Nausea and vomiting (may be projectile)
- Papilloedema on fundoscopy
- Leg spasticity and cranial nerve palsies
- Altered level of consciousness
- No head enlargement (skull rigid)
- Most common causes: posterior fossa tumors, aqueductal stenosis
Investigations
Imaging
- First-line in neonates and infants (open fontanelle = acoustic window)
- Shows ventricular size; detects germinal matrix hemorrhage
- Serial scans to document progression
- Fast; widely available; shows ventricular dilatation, periventricular lucency (transependymal edema), cause identification
- Avoids in neonates when possible (radiation); used emergently if acute deterioration
- Scout view useful for assessing shunt tubing integrity
- Best for identifying cause (aqueductal stenosis, Chiari, Dandy-Walker, tumors)
- Sagittal view: shows aqueductal stenosis; level and morphology of obstruction
- T2 periventricular signal = transependymal edema (active hydrocephalus marker)
- Small or obliterated sulcal spaces, major fissures, and basal cisterns in obstructive hydrocephalus
- Can confirm ETV patency: flow void through 3rd ventricle floor on T2
- Phase-contrast MRI: quantifies aqueductal CSF flow
Radiology Features of Obstructive Hydrocephalus
- Dilatation of temporal horns (earliest/most sensitive sign of increased ICP)
- Enlargement of anterior and posterior recesses of third ventricle
- Inferior convexity of floor of third ventricle
- Transependymal periventricular edema
- Obliterated sulci, basal cisterns
- Dilated aqueduct proximal to stenosis
Fetal Diagnosis
- Antenatal ultrasound (from 18-20 weeks): ventriculomegaly when lateral ventricular width >10 mm; triggers detailed anomaly scan and fetal MRI
Important Associated Conditions
| Condition | Details |
|---|---|
| Spina bifida cystica (myelomeningocele) | Chiari II malformation; hydrocephalus develops after surgical repair of spinal defect in ~80% |
| Dandy-Walker malformation | Triad: 4th ventricle cyst + cerebellar vermis hypoplasia + enlarged posterior fossa; hydrocephalus from obstruction at foramina of Magendie/Luschka |
| X-linked hydrocephalus | LICAM gene mutation; males only; severe aqueductal stenosis; adducted thumbs; intellectual disability |
| Holoprosencephaly | Incomplete forebrain separation; fused ventricles form a monoventricle |
Treatment
Medical (Temporizing Only)
- Acetazolamide (carbonic anhydrase inhibitor) ± furosemide: reduces CSF production; temporary measure in premature infants or post-hemorrhagic hydrocephalus while awaiting definitive surgery
- Serial lumbar punctures: for communicating hydrocephalus (post-hemorrhagic) in premature infants; not appropriate for obstructive disease
Surgical (Definitive)
- Catheter from lateral ventricle → subcutaneous → peritoneal cavity
- Contains a one-way pressure-sensitive valve
- CSF drains into peritoneum where it is absorbed
- Requires lifelong follow-up; patients are shunt-dependent
- Drains to right atrium via internal jugular vein
- Used when peritoneum unsuitable (adhesions, peritonitis)
- Higher cardiac and thromboembolic complication rate
- Endoscopic perforation of the floor of the third ventricle → CSF drains into suprasellar cistern, bypassing the obstruction
- Treatment of choice for aqueductal stenosis in children >6 months
- Avoids shunt dependency and its complications
- Confirmed on MRI by flow void through 3rd ventricle floor on T2
- Higher failure rate in infants <6 months (choroid plexus papilloma, post-hemorrhagic causes)
- Temporary emergency CSF diversion
- Used acutely; allows ICP monitoring
- Bridge to definitive treatment
Shunt Complications
| Complication | Features |
|---|---|
| Shunt blockage/malfunction | Recurrence of hydrocephalus symptoms; ventricular re-dilatation on imaging; obstruction by choroid plexus or glial tissue |
| Shunt infection | Incidence ~1-5%; ventriculitis with ependymal enhancement on MRI; devastating for developing brain |
| Overdrainage | "Slit ventricle" syndrome - chronic headaches without ventricular dilatation; subdural hematomas |
| Shunt fracture/disconnection | Seen on plain X-ray of shunt tract; calcification at fracture ends |
| Abdominal complications | Ascites, pseudocyst, bowel perforation (peritoneal end) |
Prognosis
- Untreated: progressive cortical atrophy, permanent spasticity, blindness, death
- With timely treatment: outcome depends on underlying cause, degree of cortical damage, and age at treatment
- Post-hemorrhagic hydrocephalus in premature infants: significant risk of neurodevelopmental impairment regardless of treatment
- Isolated aqueductal stenosis treated with ETV: good outcomes with normal development possible
- Serial head circumference monitoring (plotting on growth charts) is the most reliable clinical tool for follow-up
- Robbins, Cotran & Kumar Pathologic Basis of Disease (Hydrocephalus, Pathology)
- Grainger & Allison's Diagnostic Radiology (Paediatric Neuroradiology)
- Bailey & Love's Short Practice of Surgery, 28th Ed. (CSF Physiology, Hydrocephalus)
- The Developing Human - Clinically Oriented Embryology (Congenital Causes)
- S Das - Manual on Clinical Surgery, 13th Ed. (Clinical Features)
Congenital hydrocephalus
Congenital Hydrocephalus - Summary
- Non-communicating (obstructive): Block within ventricular system - most common; aqueductal stenosis is the #1 cause
- Communicating: Block outside ventricles (arachnoid fibrosis); entire ventricular system dilates
- Hydrocephalus ex vacuo: Compensatory - not true hydrocephalus, no treatment needed
| Option | Use |
|---|---|
| ETV (Endoscopic Third Ventriculostomy) | Treatment of choice for aqueductal stenosis (>6 months); shunt-free |
| VP Shunt | Most widely used; lifelong shunt dependency |
| VA Shunt | When peritoneum unsuitable |
| EVD | Temporary emergency drainage |
| Acetazolamide | Temporizing only (reduces CSF production) |
Acute appendicitis summarise
Acute Appendicitis - Summary
Epidemiology
- Most common acute surgical emergency worldwide; accounts for ~17% of ED abdominal pain presentations
- Peak incidence: teens and early twenties; rare in infants
- Lifetime risk: 8.6% males, 6.7% females
- M:F ratio = 3:2 in young adults
Aetiology & Pathology
- Mucosal inflammation (may resolve spontaneously or with antibiotics)
- Venous obstruction → ischaemia of appendix wall
- Bacterial invasion through all layers → acute appendicitis
- Ischaemic necrosis → gangrenous appendicitis
- Perforation → peritonitis or walled-off paracaecal abscess (omentum/bowel loops)
- Rarely: mucus-filled distended appendix = mucocoele
Clinical Features
Classic Presentation
| Feature | Detail |
|---|---|
| Pain | Starts periumbilical/central (visceral) → migrates to right iliac fossa (RIF) within 6-8 hours (somatic, parietal peritoneum) |
| Anorexia | Consistent and early feature |
| Nausea ± vomiting | Usually after pain onset |
| Low-grade fever | ~37.5-38°C; high fever suggests perforation |
| Constipation (or diarrhoea) | Variable |
Key Signs
| Sign | Description |
|---|---|
| McBurney's point tenderness | Maximum tenderness at junction of lateral 1/3 and medial 2/3 of line from ASIS to umbilicus |
| Rovsing's sign | Palpation of LIF causes pain in RIF (peritoneal irritation) |
| Rebound tenderness | Peritoneal irritation at RIF |
| Guarding / rigidity | Voluntary → involuntary as peritonism worsens |
| Psoas sign | RIF pain on passive hip extension (retrocaecal appendix) |
| Obturator sign | RIF pain on internal rotation of flexed right hip (pelvic appendix) |
Atypical Presentations (important to recognise)
- Retrocaecal appendix (~75%): flank/back pain, psoas sign, urinary symptoms
- Pelvic appendix: suprapubic pain, diarrhoea, urinary frequency
- Pregnancy: pain shifts superiorly as uterus enlarges; diagnosis challenging
- Elderly: vague symptoms, less fever/leukocytosis; higher perforation rate at presentation
- Children: rapid progression to perforation; diagnosis often delayed
Investigations
- Leukocytosis with neutrophilia (WBC typically 11,000-18,000); very high WBC suggests perforation
- CRP raised (often >10 mg/L; higher with perforation)
- Urine dipstick: mild pyuria/haematuria can occur (appendix near ureter/bladder) - does not exclude appendicitis
| Feature | Points |
|---|---|
| Migration of pain to RIF | 1 |
| Anorexia | 1 |
| Nausea/vomiting | 1 |
| Tenderness in RIF | 2 |
| Rebound tenderness | 1 |
| Elevated temperature | 1 |
| Leukocytosis | 2 |
| Left shift (neutrophilia) | 1 |
| Total | 10 |
- Score ≤4: appendicitis unlikely (discharge/observe)
- Score 5-6: suggestive - imaging recommended
- Score 7-8: probable - surgical referral
- Score 9-10: highly likely - operate
- Less reliable in women and children
- Ultrasound (USS): First-line (no radiation); shows non-compressible appendix >6mm, periappendiceal fat stranding; operator-dependent
- CT abdomen/pelvis (with IV ± oral contrast): Gold standard - sensitivity ~98%; shows enlarged appendix, appendicolith, fat stranding, perforation, abscess; used when USS inconclusive
- MRI: Preferred in pregnancy (avoids radiation)
Differential Diagnosis
| Condition | Key distinguishing features |
|---|---|
| Mesenteric adenitis | Children; generalised/shifting tenderness; URTI history |
| Ovarian pathology (torsion, ectopic, cyst) | Women; pelvic USS; β-hCG |
| Meckel's diverticulitis | Clinically indistinguishable; found at laparoscopy |
| Right ureteric colic | Severe colicky pain radiating to groin; haematuria; CT KUB |
| Crohn's disease (terminal ileitis) | Longer history; diarrhoea; weight loss |
| Caecal carcinoma | Elderly; mass; anaemia; CT |
| Pelvic inflammatory disease (PID) | Women; bilateral pelvic tenderness; vaginal discharge; cervical excitation |
| Psoas abscess | Chronic; hip flexion deformity; TB risk factors |
Treatment
Conservative (Antibiotics Alone)
- Selected cases of uncomplicated appendicitis (no perforation/abscess, low Alvarado score)
- IV antibiotics (e.g. co-amoxiclav or cefuroxime + metronidazole)
- Up to 30% failure rate requiring surgery within 1 year
- Interval appendicectomy can be offered after resolution
Surgical (Appendicectomy) - Definitive Treatment
- Advantages: less pain, faster recovery, lower wound infection rate, better visualisation (allows diagnosis of alternative pathology in women)
- Open appendicectomy (Lanz/gridiron incision at McBurney's point): still used in resource-limited settings or if laparoscopy unavailable/converted
Complicated Appendicitis
| Complication | Management |
|---|---|
| Appendix mass (phlegmon) | Conservative (IV antibiotics, fluids, NG); appendicectomy at 6-8 weeks (interval) |
| Appendix abscess | Radiological (USS/CT-guided) drainage + antibiotics; interval appendicectomy |
| Generalised peritonitis | Emergency laparoscopy/laparotomy; peritoneal lavage; appendicectomy |
Complications of Appendicitis (if untreated/delayed)
- Perforation → peritonitis (generalized or localised)
- Paracaecal/pelvic abscess
- Pylephlebitis (septic portal vein thrombosis - rare, serious)
- Intestinal obstruction (adhesions)
- Sepsis/multi-organ failure
Complications of Appendicectomy
- Wound infection (most common - ~5%)
- Intraabdominal abscess
- Ileus / adhesion obstruction
- Stump blowout (rare)
- Negative appendicectomy (~15-20% of cases - higher in women)
Pedicle flap and pressure sores summarise
Part 1: Pedicle Flaps
Definition
The Five C's Classification (Bailey & Love)
| C | Category | Details |
|---|---|---|
| Circulation | Blood supply type | Random vs. Axial |
| Composition | Tissue type | Cutaneous, fasciocutaneous, muscle, musculocutaneous, osseous, omentum |
| Contiguity | Proximity to defect | Local, regional, distant |
| Contour | Transfer method | Advancement, transposition, rotation, interpolation, waltzing, free |
| Conditioning | Delay procedure | Partial elevation then resetting → improves blood supply → allows larger flap harvest |
By Blood Supply (Most Important Classification)
1. Random Pattern Flap
- No dominant named blood vessel - relies on the subdermal plexus
- Blood supply is unpredictable
- Length:width ratio must not exceed 1:1 to 1.5:1 (or tip becomes ischaemic)
- Examples: rotation flap, advancement flap, transposition flap (Z-plasty, rhomboid)
2. Axial Pattern Flap (Pedicle Flap)
- Has a named dominant artery and vein running along its axis
- More reliable blood supply; can be raised as a much longer flap
- Can be used as:
- Local pedicle flap (stays attached, pivots into defect)
- Island flap (skin bridge divided; flap supplied only by buried vascular pedicle)
- Free flap (pedicle divided, vessels anastomosed at recipient site - microsurgery)
By Transfer Method
| Method | Description | Example |
|---|---|---|
| Advancement | Flap slides directly forward into defect | V-Y flap, bipedicle advancement |
| Rotation | Flap rotates about a pivot point into adjacent defect | Scalp rotation flap |
| Transposition | Flap lifted and moved laterally over intervening skin | Rhomboid (Limberg) flap, Z-plasty |
| Interpolation | Flap passed over/under skin bridge to reach non-adjacent defect | Forehead flap for nasal reconstruction |
| Waltzing | Flap moved in stages, detached and reattached progressively | Tube pedicle (Gillies) |
| Free flap | Pedicle divided; vessels anastomosed microsurgically at remote site | TRAM, ALT, fibula free flap |
By Composition
Fasciocutaneous Flaps (Cormack & Lamberty Classification)
| Type | Blood Supply | Example |
|---|---|---|
| A | Multiple perforators | Pontén flap |
| B | Single perforator along flap axis | Scapular / parascapular flap |
| C | Segmental perforators from one source vessel | Radial forearm flap, lateral arm flap |
| D | Type C + bone | Free fibular osteocutaneous flap |
Muscle/Musculocutaneous Flaps (Mathes & Nahai Classification)
| Type | Vascular Pattern | Examples |
|---|---|---|
| I | Single dominant pedicle | Gastrocnemius, tensor fascia lata |
| II | One dominant + minor pedicle(s) | Gracilis, trapezius, soleus |
| III | Dual dominant pedicles | Gluteus maximus, rectus abdominis, pectoralis minor |
| IV | Segmental pedicles | Sartorius, tibialis anterior |
| V | One dominant + segmental minor pedicles (survives on minor alone) | Latissimus dorsi, pectoralis major |
The Delay Phenomenon
- Flap partially elevated and replaced 1-2 weeks before definitive transfer
- Mechanisms: sympathetic denervation → vasodilatation; choke vessel opening; adrenergic receptor changes
- Result: increased vascular territory → larger flap can be safely raised
Flap Failure
- Arterial insufficiency: pale, cool, no capillary return → immediate re-exploration
- Venous congestion: purple, swollen, brisk dark capillary return → most common; leeches may help
- Risk factors: tension, kinking of pedicle, haematoma, infection, smoking, diabetes
Part 2: Pressure Sores (Decubitus Ulcers / Pressure Ulcers)
Definition & Pathophysiology
- ~95% occur on the lower body: 65% pelvic area, 30% lower limbs
- Ulcer begins as erythema → "punched-out" ulceration → necrosis with grey pseudomembrane
Common Sites (Bony Prominences)
| Position | Site at Risk |
|---|---|
| Supine | Sacrum, occiput, heels, elbows |
| Lateral | Greater trochanter, lateral malleolus, ear |
| Sitting | Ischial tuberosities |
| Prone | Anterior iliac spines, knees, toes |
Risk Factors (>100 identified)
- Immobility - spinal cord injury, stroke, coma, sedation, surgery
- Diabetes mellitus, peripheral vascular disease
- Cerebrovascular disease, sepsis, hypotension
- Malnutrition (low albumin), incontinence (maceration), anaemia
- Extremes of age; cognitive impairment
Staging (NPUAP/EPUAP 4-Stage System)
| Stage | Tissue Involved | Description |
|---|---|---|
| Stage I | Epidermis intact | Non-blanchable erythema; changes in skin temperature, consistency, sensation |
| Stage II | Epidermis ± dermis | Partial thickness loss; shallow open ulcer or intact blister |
| Stage III | Into subcutaneous fat | Full thickness skin loss; may see slough; no bone/tendon/muscle exposed |
| Stage IV | Muscle, bone, tendon, joint capsule | Full thickness tissue loss; exposed bone/tendon/muscle visible |
| Unstageable | Depth unknown | Base obscured by slough/eschar - cannot stage until debrided |
| Deep tissue injury | Suspected deep damage | Purple/maroon intact skin or blood-filled blister from pressure/shear |
Complications
- Sepsis (most serious); local infection; cellulitis
- Osteomyelitis (underlying bone)
- Fistula formation
- Malignant transformation (Marjolin's ulcer - SCC in chronic ulcer)
- Anaerobic colonisation → putrid odour
Prevention (Most Important!)
- Repositioning every 2 hours (minimum) - cornerstone of prevention
- Pressure-redistributing mattresses/cushions: foam, air-filled, gel, water/liquid flotation
- Meticulous skin care; moisture barriers; treat incontinence
- Nutritional optimisation (protein, vitamin C, zinc)
- Risk assessment tools: Braden Scale, Waterlow Score, Norton Scale
- Early mobilisation; heel protectors
Treatment
Conservative (All Stages)
- Pressure relief - remove/redistribute pressure completely
- Positioning - frequent turning, 30° tilt lateral position (not 90°), heel elevation
- Wound debridement:
- Sharp/surgical (fastest)
- Mechanical (wet-to-dry dressings - avoid in granulating wounds)
- Enzymatic (collagenase)
- Autolytic (occlusive dressings)
- Frequency: at least weekly
- Exception: Stable dry heel eschar - do NOT debride (risk of opening vascular wound)
- Wound cleaning: Normal saline - not hydrogen peroxide or povidone-iodine (cytotoxic to healing tissue)
- Dressing selection (keep wound moist, surrounding skin dry):
| Dressing | Use |
|---|---|
| Transparent film | Stage II only (light drainage) |
| Hydrocolloid | Stage II-III; mild exudate |
| Alginate | Heavy exudate; haemostatic |
| Foam | Moderate exudate |
| Hydrofiber | Stage III-IV full thickness only |
| Hydrogel | Dry/necrotic wounds; promotes autolysis |
- Infection management: topical antibiotics if infected; systemic if cellulitis/sepsis; topical metronidazole eliminates odour from anaerobic colonisation within 36 hours
- Nutrition: high-protein diet; supplements (vitamin C, zinc); dietitian input
- Pain management
Surgical (Stage III/IV)
- Debridement ± wound VAC (negative pressure wound therapy)
- Flap reconstruction - muscle or musculocutaneous flaps are preferred (bring vascularised tissue to fill dead space over bone):
- Ischial ulcers: gracilis, biceps femoris, posterior thigh, gluteus maximus flaps
- Sacral ulcers: gluteus maximus advancement/rotation flap
- Trochanteric ulcers: tensor fascia lata, vastus lateralis flaps
- Prerequisites before surgery: nutritional optimisation, infection control, complete pressure relief
- High recurrence rate if precipitating factors not addressed
Lucid interval and haemopneumothorax summarise
Part 1: Lucid Interval
Definition
- Patient is knocked unconscious at the time of impact
- Regains consciousness for a period (minutes to hours)
- Becomes unconscious again - this second deterioration signals expanding intracranial haematoma
"Lucid interval is the short period of consciousness between initial unconsciousness which occurs immediately after accident and unconsciousness at later stage after the lucid interval." - S Das
Pathophysiology
- Trauma (often minor blow to temporal region) → fracture of temporal squama → rupture of the middle meningeal artery (or anterior branch)
- Arterial bleeding accumulates between skull and dura (extradural space)
- Initial concussive LOC resolves as brain recovers
- As haematoma expands → progressive brain compression → tentorial herniation → ipsilateral 3rd nerve palsy → contralateral hemiparesis → coma → death (if untreated)
Key Points: EDH vs SDH
| Feature | Extradural Haematoma (EDH) | Subdural Haematoma (SDH) |
|---|---|---|
| Source of bleed | Middle meningeal artery (arterial) | Bridging veins (venous) |
| Location | Between skull and dura | Between dura and arachnoid |
| Lucid interval | Classic - ~50% present this way | Less classic - ~12-36% have lucid period |
| CT appearance | Biconvex (lens-shaped) hyperdense; cannot cross suture lines | Crescent-shaped (concave); crosses suture lines |
| Skull fracture | Temporal fracture often coexists | May occur without fracture |
| Progression | Rapid (arterial) - hours | Slower (venous); acute within 24h, chronic >2 weeks |
| Prognosis | Excellent if promptly evacuated | Worse - 40-60% mortality if surgical intervention needed |
| Mechanism | Temporal blow (sports, assault) | Acceleration-deceleration; shaken baby |
Clinical Features of EDH
- History of blow to head (often apparently minor)
- Initial brief LOC → lucid interval (patient may complain of headache, appear well)
- Progressive drowsiness, severe headache, vomiting
- Ipsilateral fixed dilated pupil (CN III compression from uncal herniation)
- Contralateral hemiparesis (ipsilateral cerebral peduncle compression)
- Rapid deterioration to coma and death if untreated
- Cushing's triad (late): hypertension + bradycardia + irregular respirations
Post-Traumatic Amnesia (PTA) - Severity Guide (S Das)
| PTA Duration | Severity of Head Injury |
|---|---|
| <1 hour | Slight |
| 1-24 hours | Moderate |
| 1-7 days | Severe |
| >1 week | Almost fatal |
Investigations
- Urgent CT head (non-contrast): biconvex hyperdense collection for EDH
- Skull X-ray: temporal fracture (but CT supersedes)
- GCS scoring: deteriorating GCS is the red flag
Treatment of EDH
- Emergency craniotomy / burr hole + evacuation of haematoma
- If EDH rapidly detected and evacuated → excellent functional outcome
- Arterial EDHs detected within hours; venous sinus EDHs may be delayed
- Any deteriorating GCS after head injury = urgent CT + neurosurgical referral
Part 2: Haemopneumothorax
Definition
Pneumothorax
Types
| Type | Mechanism | Features | Treatment |
|---|---|---|---|
| Simple (closed) | Air in pleural space; no continued entry | Ipsilateral reduced breath sounds; hyperresonance | Small: observe; Large: chest drain |
| Open (sucking chest wound) | Chest wall defect allowing air entry with respiration | "Sucking" wound; paradoxical breathing | Seal wound with 3-sided occlusive dressing; then chest drain elsewhere |
| Tension | One-way valve effect - air enters but cannot escape | Life-threatening emergency (see below) | Immediate needle decompression |
Tension Pneumothorax - Emergency
- Respiratory distress, hypoxia
- Tracheal deviation away from affected side (late sign)
- Absent breath sounds on affected side
- Hyperresonance to percussion
- Jugular venous distension (JVD)
- Hypotension → cardiovascular collapse
- Needle decompression - 2nd intercostal space, midclavicular line (temporary)
- Followed immediately by chest drain (tube thoracostomy) - 5th ICS, anterior axillary line
Haemothorax
Definition & Sources
- Intercostal vessels (rib fractures)
- Lung laceration
- Major vessels (aorta, subclavian, internal mammary)
- Diaphragmatic/abdominal organ injuries
Classification by Volume
| Type | Blood Volume | Features | Management |
|---|---|---|---|
| Small haemothorax | <300 mL | Often asymptomatic; seen on CT only | Observe; may resolve spontaneously |
| Moderate haemothorax | 300-1500 mL | Dull percussion; decreased breath sounds | Chest drain (ICS 5, AAL) |
| Massive haemothorax | >1500 mL (adult) | Haemodynamic instability; dullness | Chest drain + immediate resuscitation ± surgery |
Massive Haemothorax
- Defined as >1500 mL on initial chest drain output
- Adult surgical thoracotomy indications:
- Initial drain output >1500 mL
- Ongoing output >150-200 mL/hr for 4+ hours
- Paediatric equivalent: ~20% of estimated blood volume initially, or ongoing 2-3 mL/kg/hr
- However: patient physiology (haemodynamic instability) should drive surgical decision more than absolute volumes
Haemopneumothorax
Combined Presentation
- Features of both: dullness (blood) + hyperresonance (air) may be present simultaneously
- More commonly: decreased air entry throughout with dullness at base
- Common in penetrating chest trauma (stab/gunshot) and severe blunt trauma
- CXR: fluid level (blood) with air above
Management
| Step | Action |
|---|---|
| Airway | Secure and maintain |
| Breathing | High-flow O₂; assess and treat immediately life-threatening chest injuries |
| Circulation | Two large-bore IV access; fluid resuscitation; blood products |
| Chest drain | 5th ICS, anterior axillary line (safe triangle) - drains both blood AND air simultaneously |
| CXR | Post-procedure to confirm expansion |
- Borders: anterior border of latissimus dorsi, lateral border of pectoralis major, base of axilla, above 5th ICS
- Insert above the rib to avoid neurovascular bundle (runs below each rib)
- Use large bore drain (28-32F) for haemothorax (allows clot drainage)
- Massive haemothorax with ongoing haemodynamic instability
- Persistent air leak
- Clotted haemothorax (retained haemothorax - best managed with VATS)
- Aortic or great vessel injury
- Cardiac injury / tamponade
- Risk of empyema and fibrothorax
- Managed with video-assisted thoracoscopic surgery (VATS) - increasingly preferred over open approach
Life-Threatening Chest Injuries - "Deadly Dozen" Summary
- Airway obstruction
- Tension pneumothorax → needle decompression
- Open pneumothorax → 3-sided occlusive dressing
- Massive haemothorax → chest drain + fluids
- Flail chest with pulmonary contusion → ventilatory support
- Cardiac tamponade → pericardiocentesis / thoracotomy
Post op pulmonary complication and treatment of perforation peritonitis summarise
Part 1: Postoperative Pulmonary Complications (PPCs)
Definition & Significance
Pathophysiology
- Reducing functional residual capacity (FRC) - lung volumes fall, particularly after thoracic/upper abdominal surgery
- Diaphragmatic dysfunction - stimulation of GI viscera during surgery alters diaphragmatic movement for days
- Impaired mucociliary clearance - from anaesthesia, pain, opioids → secretion retention
- Reduced cough effort - pain limits deep breathing and coughing
- Net result: V/Q mismatch, shunting, atelectasis, secretion pooling → infection risk
Risk Factors (Bailey & Love / Sabiston)
| Patient Factors | Procedure Factors | Lab Markers |
|---|---|---|
| Non-modifiable: Age, male sex, ASA >II, frailty, malignancy, acute URTI within 1 month, impaired cognition, stroke, long-term steroids, weight loss >10% | Non-modifiable: Thoracic/upper abdominal surgery, vascular surgery, emergency surgery, duration >2 hours, reoperation | Raised urea/creatinine |
| Modifiable: Smoking, COPD/asthma, OSA, obesity (BMI <18.5 or >40), hypertension, CCF, chronic liver failure, renal failure, DM, alcohol, GORD, preoperative sepsis | Modifiable: General vs. regional anaesthesia, NMB agents, open vs. laparoscopic, mechanical ventilation strategy, intraoperative transfusion | Low albumin, SpO₂ <96%, abnormal CXR preop, anaemia <10 g/dL, FEV₁/FVC <0.7, FEV₁ <80% |
Individual Complications
1. Atelectasis (Most Common PPC)
- Partial or complete collapse of alveoli; most common cause of postoperative fever in early period (POD 1-2)
- Features: Fever, tachypnoea, reduced SpO₂, absent/reduced breath sounds; CXR - loss of hemidiaphragm, air bronchograms, volume loss with tracheal deviation toward collapse
- Treatment:
- Early mobilisation (out of bed 3x/day)
- Deep breathing exercises (5 breaths held 5-6 seconds)
- Incentive spirometry (ICOUGH protocol)
- Coughing and chest physiotherapy
- Bronchodilators; hydration; tracheal suctioning if needed
- Optimal analgesia - multimodal (paracetamol + NSAIDs + opioids PRN + regional blocks) to enable deep breathing
- Reversible within 24-48 hours with above measures
2. Pneumonia
- Develops from retained secretions ± aspiration
- Features: fever (typically POD 3-5), productive cough, consolidation on CXR, leukocytosis
- Treatment: antibiotics guided by sputum culture; physiotherapy; adequate analgesia
3. Aspiration
- Aspiration pneumonitis (Mendelson syndrome): Chemical injury from sterile acidic gastric contents (pH <2.5); treat supportively (O₂, CPAP/ventilation)
- Aspiration pneumonia: Infective; from colonised oropharyngeal secretions; requires antibiotics
- Risk factors: emergency surgery, bowel obstruction, impaired consciousness, GLP-1 receptor agonists (delayed gastric emptying), oropharyngeal instrumentation
4. Postoperative Respiratory Failure
- Defined as ventilator dependency >48 hours after surgery
- Causes: ARDS, severe pneumonia, PE, severe atelectasis, bronchospasm, worsening COPD
- Management: escalating respiratory support (NIV → invasive ventilation), ICU admission
5. Bronchospasm
- Especially in asthmatics/COPD patients; triggered by airway manipulation, aspiration, pain
- Treatment: nebulised bronchodilators (salbutamol, ipratropium), IV steroids, correct trigger
6. Pleural Effusion
- Post-thoracic/cardiac/upper abdominal surgery or from hypoalbuminaemia
- Significant effusions: thoracocentesis or chest drain
Prevention (ICOUGH Protocol - Sabiston)
- I - Incentive spirometry
- C - Coughing and deep breathing
- O - Oral care (brushing teeth + mouthwash - reduces VAP risk)
- U - Understanding (patient education)
- G - Getting out of bed (early mobilisation 3x/day)
- H - Head of bed elevation (>30°)
Part 2: Treatment of Perforation Peritonitis
Classification of Peritonitis
| Type | Description | Example |
|---|---|---|
| Primary | No GI source; haematogenous spread | SBP in cirrhosis; TB peritonitis |
| Secondary | GI perforation/transmural infection | Perforated appendix, peptic ulcer, colon; most common surgical peritonitis |
| Tertiary | Persistent/recurrent despite treatment; nosocomial organisms | ICU patients; antibiotic-resistant organisms; mortality up to 50% |
Pathophysiology
Diagnosis
- Sudden onset severe abdominal pain; board-like (generalised) rigidity
- Generalised rebound tenderness, guarding
- Absent bowel sounds
- Signs of systemic sepsis: fever, tachycardia, hypotension
- Note: Not all peritonitis requires surgery (e.g. localised diverticular peritonitis may respond to antibiotics)
- FBC (leukocytosis), CRP, LFTs, U&E, lactate, blood cultures
- Erect CXR: Free air under diaphragm (pneumoperitoneum) - limited sensitivity; absence does NOT exclude perforation
- CT abdomen/pelvis (with IV ± oral contrast): Gold standard; much more sensitive than plain films; can identify site of perforation, free air, free fluid, abscesses
- Peritoneal lavage: If CT unavailable or patient too unstable; >500 WBC/mm³, elevated amylase/bilirubin, or +Gram stain = ~90% likelihood of surgical peritonitis
- Diagnostic laparoscopy: Highly accurate; many causes can be dealt with laparoscopically
Treatment - The Three Pillars
1. Resuscitation
- IV access (2 large-bore); aggressive fluid resuscitation (30 mL/kg bolus)
- Guided by: BP (arterial line if shocked), HR, CVP, mixed venous O₂ sat, urine output (target >0.5 mL/kg/hr)
- Monitor: FBC, U&E, glucose, creatinine, blood gases, serum lactate (Surviving Sepsis guidelines)
- Vasopressors only after adequate volume resuscitation fails
- Glucocorticoids only for septic shock refractory to fluids + vasopressors
- O₂ therapy; urinary catheter; NGT (bowel decompression)
- Blood products if anaemic/coagulopathic
2. Antibiotics
| Setting | Organisms | Antibiotic Choice |
|---|---|---|
| Community-acquired | Gram-negative bacilli, anaerobes, enterococci | Broad-spectrum beta-lactam (e.g. piperacillin-tazobactam) OR cephalosporin + metronidazole |
| Hospital-acquired / healthcare-associated | Resistant organisms (MRSA, ESBL, Candida) | Broader cover; discuss with microbiology |
| Colonic source | Gram-negative aerobes + anaerobes | Must cover both; metronidazole essential |
| Candida | Treat only if: septic shock, immunocompromised, or hospital-acquired | Antifungal (fluconazole/echinocandin) |
- Monotherapy: broad-spectrum beta-lactam (e.g. piperacillin-tazobactam) = as effective as beta-lactam + aminoglycoside
- Fluoroquinolone + metronidazole
- Aminoglycosides avoided if possible (nephrotoxicity)
3. Surgical Intervention (Source Control) - Mainstay
- Source control - close/resect/exteriorise the perforation
- Peritoneal decontamination - copious washout (lavage) with warm saline
- Prevention of recurrence - drainage of abscesses, fascial closure
- Laparotomy - gold standard for definitive management
- Laparoscopy - increasingly successful for selected cases (perforated peptic ulcer, appendix, selected colonic perforations)
| Cause | Procedure |
|---|---|
| Perforated peptic ulcer | Graham patch (omental patch) ± H. pylori eradication |
| Perforated appendix | Appendicectomy ± lavage |
| Perforated diverticulum | Hartmann's procedure (resection + end colostomy) or primary anastomosis ± defunctioning stoma |
| Free colonic perforation | Resection ± stoma |
| Anastomotic leak | Re-explore; takedown + stoma vs. washout + drain |
- Used when source control not possible at first operation
- Reasons for planned re-exploration: tenuous source control, bowel viability assessment, inadequate drainage, haemodynamic instability, fecal peritonitis, reassessment of anastomosis, abdominal compartment syndrome
Nutrition
- Peritonitis = hypermetabolic state comparable to 50% TBSA burn
- 3000-4000 kcal/day may still not achieve positive nitrogen balance
- Enteral preferred over parenteral (maintains gut barrier)
- Feeding jejunostomy tube placed at initial operation in critically ill patients
Prognosis
| Cause | Mortality |
|---|---|
| Perforated appendix | ~10% |
| Perforated duodenal ulcer | ~10% |
| General secondary peritonitis | Up to 30% |
| Tertiary peritonitis (nosocomial) | Up to 50% |
Ewings sarcoma
"Ewing sarcoma"[MeSH Terms] AND treatment
Ewing's Sarcoma
Definition & Overview
- The 2nd most common primary malignant bone tumor in patients under 30 years
- The most common primary bone malignancy in patients under 10 years
- The 3rd most common overall nonhematologic primary bone malignancy
- Incidence: <1 per million per year; ~200 cases/year in the USA
Molecular Biology / Pathogenesis
- >90% of cases carry a balanced translocation t(11;22)(q24;q12)
- Fuses the EWSR1 gene (chromosome 22) with the FLI1 gene (chromosome 11)
- Produces a chimeric EWS/FLI1 fusion protein - an aberrant transcription factor
- Binds to chromatin and dysregulates transcription → uncontrolled proliferation, abnormal differentiation
- Other less common translocations involve EWS with other ETS family transcription factors
- Cell of origin: Uncertain - mesenchymal stem cells or primitive neuroectodermal cells most likely
- No known predisposing factors
- Exceedingly rare in individuals of African descent; predominantly affects Whites of European origin
Epidemiology
| Feature | Detail |
|---|---|
| Age | 5-25 years; peak in 2nd decade |
| Sex | Slight male predominance |
| Race | Predominantly White/European; very rare in Black African populations |
| Incidence | ~200 cases/year USA; <1/million/year globally |
Location
- Diaphysis of long bones (most characteristic) with frequent extension into the metaphysis
- Flat bones of shoulder girdle and pelvic girdle (common)
- Pelvis and ribs frequently involved
- Femur, tibia, fibula, humerus, pelvis most common sites
- Spine: 3.5-15% of cases; sacrum and lumbar spine predominate; sacral involvement up to 50%
- Rarely: small bones of hands/feet
- 20% are extraskeletal (extraosseous Ewing's sarcoma) - arising in soft tissue
Clinical Features
Symptoms
- Pain - nearly universal; onset often insidious, initially mild/intermittent
- May mimic musculoskeletal injury; responds temporarily to conservative treatment → diagnosis delayed
- Average delay from symptom onset to diagnosis: 34 weeks (15 weeks patient delay + 19 weeks physician delay)
- Swelling at the affected site - often large soft-tissue mass
- Fever - low-grade, intermittent; mimics osteomyelitis
- Erythema overlying the lesion
Signs
- Tender, warm, swollen mass
- May have palpable soft-tissue component
- Neurological deficits if spinal involvement
Systemic Features (simulating infection/malignancy)
- Intermittent low-grade fever
- Leukocytosis
- Anaemia
- Elevated ESR and CRP
- Can clinically and radiologically mimic osteomyelitis - one of the most important differentials
Pathology
Macroscopic
- Soft, tan-white tumor arising in the medullary cavity
- Invades cortex, periosteum, and soft tissue
- Frequently shows areas of haemorrhage and necrosis
Microscopic
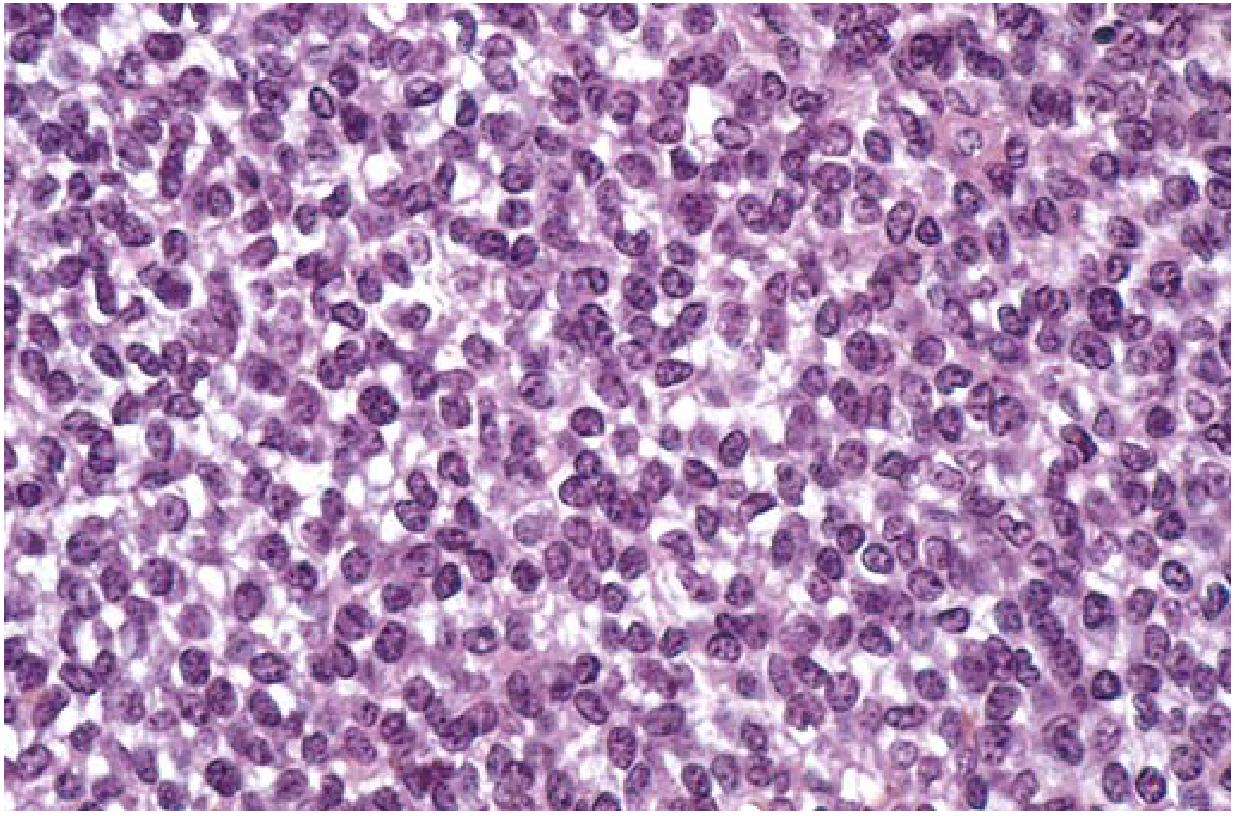
- Sheets of uniform small round cells - slightly larger than lymphocytes
- Scant cytoplasm - clear/pale due to glycogen content (PAS positive)
- Homer-Wright rosettes may be present (circular groupings around fibrillary core)
- No bone or cartilage production (distinguishes from osteosarcoma)
- One of the "small round blue cell tumors" of childhood
Small Round Blue Cell Tumors - Differential (mnemonic: "LEMON")
- Lymphoma
- Ewing's sarcoma / PNET
- Medulloblastoma / rhabdoMyosarcoma
- Oat cell (small cell lung)
- Neuroblastoma
Immunohistochemistry
- CD99 (MIC2) strongly positive - characteristic marker
- Vimentin positive
- NSE and S100 variable (neural differentiation)
Radiological Features
Plain X-Ray
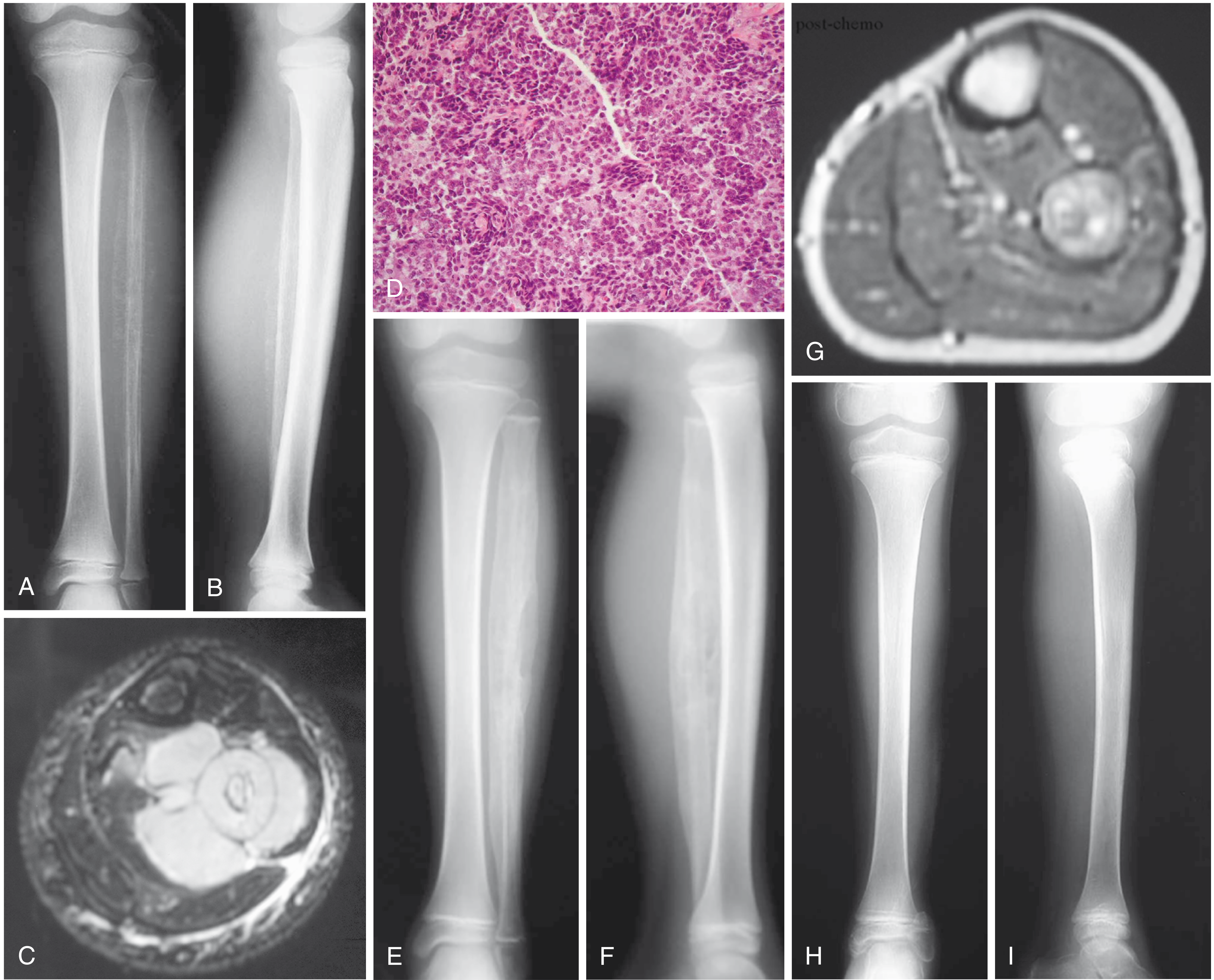
- Permeative ("moth-eaten") lytic destruction with ill-defined margins
- "Onion-skin" periosteal reaction - most characteristic; layers of reactive bone from periosteal elevation
- Often involves a large portion or the entire bone (more so than osteosarcoma)
- Codman's triangle may be seen (reactive bone at tumor margins)
- Large associated soft-tissue mass often visible
- Diaphyseal location (vs. osteosarcoma which is metaphyseal)
MRI (Investigation of Choice for Local Staging)
- T1: isointense to muscle
- T2: hyperintense; highlights extent of bone marrow and soft-tissue involvement
- Gadolinium: intense enhancement due to hypercellularity
- Delineates intraosseous and extraosseous extent; relationship to neurovascular structures
- "Curtain sign" - invasion of spinal canal in vertebral disease
CT
- Greater sensitivity than X-ray for cortical destruction, permeative pattern, soft-tissue mass
- Used for staging (chest CT for lung metastases)
Bone Scan (Tc-99m)
- Identifies skip lesions and distant bone metastases
FDG-PET/CT
- New standard for initial staging and detection of recurrence/new metastases
- Initial SUV of primary tumor correlates with tumor aggressiveness
Investigations
| Investigation | Purpose |
|---|---|
| Plain X-ray of affected bone | Initial imaging; characteristic onion-skin pattern |
| MRI of affected region | Local staging; extent; surgical planning |
| CT chest/abdomen/pelvis | Pulmonary metastases; lymph node assessment |
| Bone scan | Skeletal metastases |
| FDG-PET/CT | Full body staging; new standard |
| FBC, ESR, CRP, LDH | Elevated; LDH is a prognostic marker |
| Biopsy (open or CT-guided) | Definitive diagnosis; must be done at treating centre |
| Bone marrow biopsy (posterior iliac crest) | Marrow involvement staging |
| Molecular studies / FISH | Confirm EWS-FLI1 translocation |
Staging
- Local disease - size, compartmentalization
- Metastatic disease - lung (most common), bone, bone marrow
| Stage | Description | Prognosis |
|---|---|---|
| Localized, non-metastatic | No clinically detectable metastases | Better |
| Metastatic | Lung, bone, or bone marrow metastases | Poor |
| Pelvis primary | Worse than extremity primaries regardless of metastases | Intermediate-poor |
- Metastatic disease at presentation
- Pelvic / axial location (vs. distal extremity)
- Large tumor volume (>200 mL)
- Poor histological response to neoadjuvant chemotherapy (<90% necrosis = poor; 100% necrosis = good response)
- Age >14-20 years (paradoxically worse than younger or older)
- Elevated LDH
- FLI1 type 2 fusion transcript
Treatment
1. Neoadjuvant Chemotherapy (First)
- Vincristine + Doxorubicin (adriamycin) + Cyclophosphamide (VDC)
- Alternating with Ifosfamide + Etoposide (IE)
- Dose-intensive regimen; dose intensification improves outcomes
- Duration: ~12-18 weeks before local treatment
- Treat micrometastatic disease (present even in "localised" cases)
- Reduce tumor size and soft-tissue mass → facilitates limb-salvage surgery
- Assess histological response (% necrosis at surgery) - important prognostic marker
- Good response: ≥90% necrosis (some protocols require 100%)
- Poor response: <90% necrosis → consideration of alternative regimens
2. Local Control (Surgery ± Radiotherapy)
- Wide local excision (limb-salvage) is preferred when achievable with adequate margins
- Avoids complications of radiation in growing children (growth disturbance, radiation sarcoma)
- Reconstruction: endoprosthesis, allograft, allograft-prosthesis composite, vascularised fibula graft depending on site/age
- Amputation reserved for cases where adequate margins cannot be achieved with limb-salvage
- Pelvic tumors: internal hemipelvectomy or hindquarter amputation for large tumors
- Ewing's sarcoma is radiosensitive - used when surgical resection not feasible or margins inadequate
- Doses: 45-55 Gy (definitive); 45-50 Gy (adjuvant post-surgery with close margins)
- Primary radiation (without surgery) for inoperable sites (pelvis, spine, sacrum)
- Spinal Ewing's: chemotherapy + radiotherapy primary; surgery for neurological compromise or instability
- Long-term complications: radiation-induced sarcoma, growth disturbance, fibrosis
- Surgery preferred when wide margins achievable (better local control; avoids late radiation effects)
- Radiation when surgical morbidity unacceptable or adequate resection not possible
3. Adjuvant Chemotherapy
- Continuation of VDC/IE regimen post local treatment
- Total treatment duration: ~10-12 months
Salvage Chemotherapy (Relapsed/Refractory Disease)
- Cyclophosphamide + topotecan
- Irinotecan + temozolomide
- Gemcitabine + docetaxel
Prognosis
| Group | 5-Year Survival |
|---|---|
| Localized disease (all sites) | ~70% event-free survival; 75% 5-year survival |
| Long-term cure (localized) | ~50% |
| Metastatic disease at diagnosis | Poor (<30% 5-year survival) |
| Spinal Ewing's (surgical series) | 82% at 1 yr, 75% at 2 yr, 57% at 5 yr |
Key Differentials
| Condition | Distinguishing Features |
|---|---|
| Osteomyelitis | Most important; identical clinical/imaging features; biopsy essential |
| Osteosarcoma | Metaphyseal; osteoid production; older age (15-25); sunburst periosteal reaction |
| Lymphoma of bone | Older patients; systemically unwell; CD20+ |
| Eosinophilic granuloma | Vertebra plana; less systemic features; CD1a+ |
| Neuroblastoma | <5 years; urine catecholamines; adrenal primary |
| Rhabdomyosarcoma | Soft tissue origin; desmin+, myogenin+ |
| Metastatic neuroblastoma | Young children; skeletal metastases; primary abdominal |
One page summary for ewings sarcoma
Ewing's Sarcoma - One Page Summary
Key Facts
- 2nd most common malignant bone tumor in <30 yrs (after osteosarcoma); most common in <10 yrs
- Age: 5-25 yrs (peak 2nd decade); slight male predominance; very rare in Black African populations
- Genetics: t(11;22) → EWS-FLI1 fusion protein (>90% of cases) → aberrant transcription → uncontrolled growth
- No known predisposing factors
Sites
- Diaphysis of long bones (femur, tibia, fibula, humerus) - with metaphyseal extension
- Flat bones - pelvis, ribs, scapula (pelvic = worse prognosis)
- 20% extraskeletal (soft tissue); spine 3.5-15%
Clinical Features
| Feature | Detail |
|---|---|
| Pain | Universal; insidious onset; average 34-week delay to diagnosis |
| Swelling | Often large soft-tissue mass |
| Fever + erythema | Mimics osteomyelitis (most important differential) |
| Systemic | Leukocytosis, raised ESR/CRP, anaemia |
Radiology
| Modality | Findings |
|---|---|
| X-ray | Permeative lytic lesion; "onion-skin" periosteal reaction; large soft-tissue mass; involves large portion of bone |
| MRI | Gold standard for local staging; T2 hyperintense; gadolinium enhancement |
| CT | Cortical destruction; lung metastases staging |
| FDG-PET/CT | New standard for full staging and recurrence |
Pathology
- Gross: Soft, tan-white; haemorrhage and necrosis
- Micro: Sheets of uniform small round blue cells; scant glycogen-rich (clear) cytoplasm; Homer-Wright rosettes; no bone/cartilage
- IHC: CD99 (MIC2) strongly +; vimentin +
Small Round Blue Cell Tumors DDx: LEMON
Investigations
- X-ray → MRI → CT chest/abdomen → FDG-PET/CT
- Bloods: FBC, ESR, CRP, LDH (prognostic)
- Biopsy (at treating sarcoma centre - tract must be excisable)
- Bone marrow biopsy; molecular FISH for EWS-FLI1
Treatment (Multimodal)
Neoadjuvant chemo (12-18 wks)
↓
Local control (surgery ± RT)
↓
Adjuvant chemo (total ~10-12 months)
- VDC: Vincristine + Doxorubicin + Cyclophosphamide
- IE: Ifosfamide + Etoposide
- Surgery (preferred): Wide local excision + reconstruction (limb-salvage); avoids radiation late effects in children
- Radiotherapy: Radiosensitive tumor; used when surgery not feasible (pelvis, spine); 45-55 Gy
- Amputation if adequate margins unachievable
- ≥90% necrosis = good response → better prognosis
- <90% necrosis = poor response → consider regimen change
Prognosis
| Group | 5-Year Survival |
|---|---|
| Localised disease | ~70% EFS; 50% long-term cure |
| Metastatic disease | <30% |
Key Differentials
Claw toes
Claw Toes
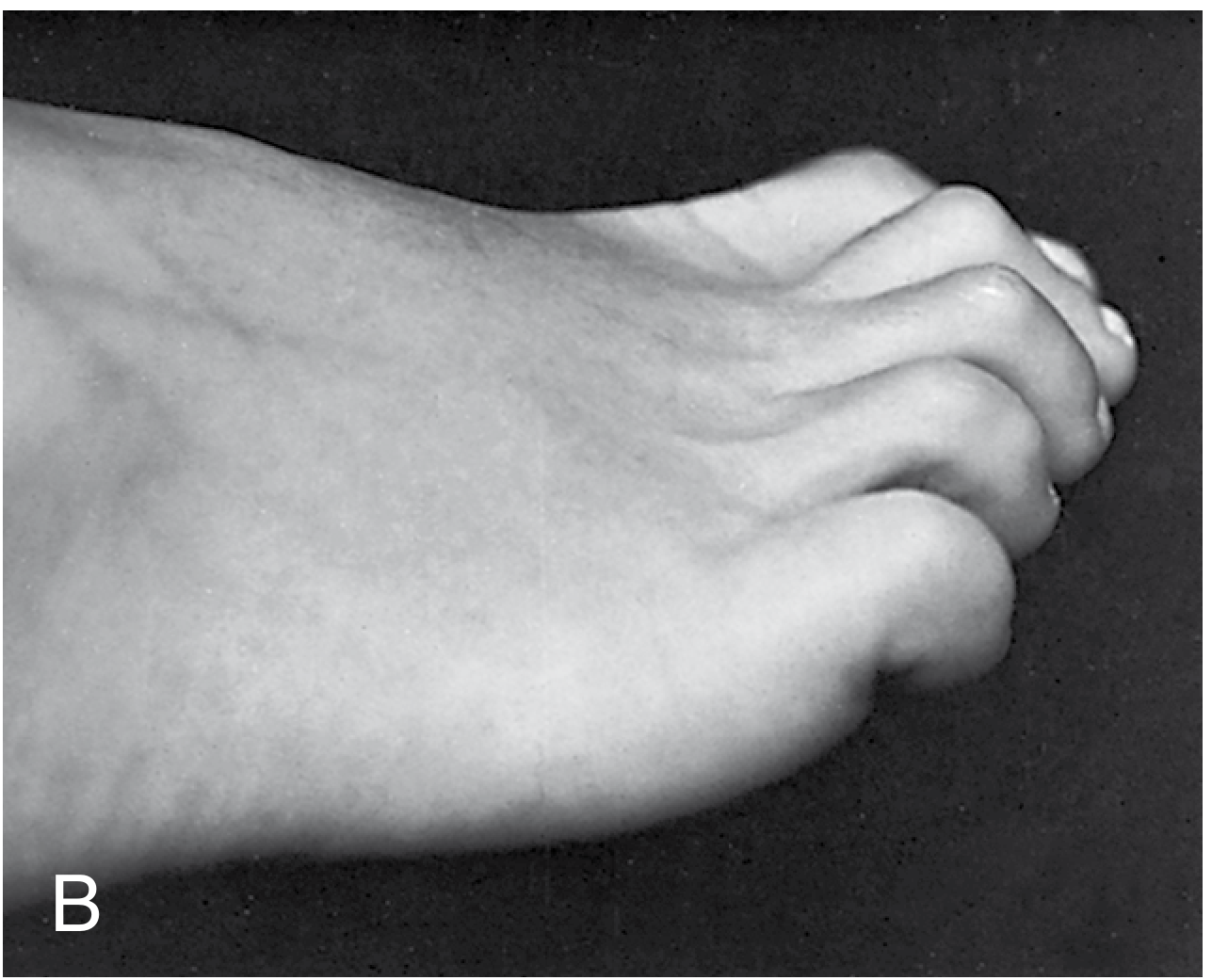
Definition
- Hyperextension at the metatarsophalangeal (MTP) joint
- Flexion at both the proximal interphalangeal (PIP) joint
- Flexion at the distal interphalangeal (DIP) joint
Distinguishing Claw Toe, Hammer Toe, and Mallet Toe
| Feature | Claw Toe | Hammer Toe | Mallet Toe |
|---|---|---|---|
| MTP joint | Hyperextended (always) | May or may not be extended | Normal |
| PIP joint | Flexed | Flexed (primary deformity) | Normal |
| DIP joint | Flexed | Usually normal | Flexed (only joint) |
| Toes involved | All lesser toes (bilateral) | 1-2 toes (usually 2nd) | Usually 2nd toe only |
| Cause | Usually neuromuscular | Footwear/biomechanical | Footwear/FDL contracture |
| Intrinsic imbalance | Always present | Usually absent | Absent |
"Complex hammer toe refers to concomitant dorsiflexion of the MTP joint that does not correct - more appropriately termed and treated as a claw toe" - Miller's Review
Pathomechanics (Intrinsic Minus Deformity)
- Interossei and lumbricals pass plantar to the MTP axis → flex MTP joint
- Simultaneously extend IP joints via the extensor hood
- EDL (extensor digitorum longus) - unopposed → hyperextends MTP joint
- With MTP in hyperextension, EDL loses excursion → can no longer extend the IP joints
- FDL (flexor digitorum longus) - unopposed at IP joints → flexes PIP and DIP joints
- The deformity becomes self-perpetuating: MTP hyperextension further neutralises the antagonist effects of the flexors at the MTP level and of the extensors at the IP level
- Increased plantar pressure under metatarsal heads (fat pad migrates distally)
- Dorsal prominence at PIP → pressure from shoe upper → hard corn (heloma durum)
- Distal pulp pressure → end corn
- Plantar callosity under metatarsal heads
Aetiology
Neurological / Neuromuscular (Classic cause of claw toes affecting all toes)
| Condition | Mechanism |
|---|---|
| Charcot-Marie-Tooth disease (hereditary motor-sensory neuropathy) | Most classic neurological association; pes cavus + claw toes |
| Pes cavus (any cause) | High arch → intrinsic imbalance |
| Poliomyelitis | Intrinsic paralysis |
| Spinal cord lesions | Intrinsic denervation |
| Diabetic peripheral neuropathy | Intrinsic atrophy |
| Alcoholic neuropathy | Intrinsic atrophy |
| Medial/lateral plantar nerve injury | Direct intrinsic loss |
| Compartment syndrome (foot) | Ischaemic intrinsic contracture |
Non-Neurological
- Ill-fitting footwear (narrow toe box; high heels) - most common cause of isolated hammer/claw toes; F:M ratio up to 5:1
- Rheumatoid arthritis - MTP joint synovitis → plantar plate destruction → dorsal subluxation of proximal phalanx
- Hallux valgus - 2nd toe crowded, buckled
- Connective tissue disorders
- Trauma
- Long second ray ("Morton's foot")
Clinical Features
Symptoms
- Pain - most commonly over the dorsum of PIP joint (pressure from shoe)
- Pain under metatarsal heads (metatarsalgia) - shifted loading
- Difficulty with footwear
Signs
- Hyperextension MTP + flexion PIP + flexion DIP (all lesser toes)
- Hard corn (heloma durum) - dorsum of PIP joint from shoe pressure
- End corn - plantar surface of toe tip from DIP flexion
- Plantar callosities under metatarsal heads from depressed MT heads
- Flexible vs. fixed deformity - test by holding MTP in neutral and assessing IP joint mobility
- In diabetics/sensory neuropathy: ulceration and deep infection at pressure points
- Assess for underlying neurological cause (sensory loss, wasting, reflexes, pes cavus)
Flexibility Assessment (Key Examination)
- Flexible: Passively correctable to neutral position at rest → better prognosis; soft tissue procedures
- Fixed (rigid): Not passively correctable → bony procedures required
Investigations
- X-rays (weight-bearing): Assess joint subluxation/dislocation at MTP, degree of deformity, arthritic changes
- Neurological workup if bilateral/all toes involved: nerve conduction studies, EMG, spine MRI
- Consider: blood glucose (DM), rheumatoid factor, anti-CCP
Treatment
Conservative (First Line)
- Footwear modification: Wide toe box, low heel, extra depth shoes; most important initial measure
- Toe splints/buddy strapping for flexible deformities - maintain correction
- Metatarsal pads/orthotics - offload metatarsal heads, redistribute pressure
- Chiropody: Regular debridement of corns and callosities
- Physiotherapy: Intrinsic strengthening exercises (towel scrunching, marble picking) for flexible deformities
- Patient education: avoid tight/high-heeled footwear
Surgical (When Conservative Fails)
Flexible Claw Toe
- Girdlestone-Taylor FDL flexor-to-extensor transfer: FDL tendon divided at DIP, rerouted dorsally and sutured to extensor hood - corrects both IP flexion and MTP hyperextension simultaneously; procedure of choice for flexible claw toe
- EDB (extensor digitorum brevis) tenotomy + EDL lengthening to correct MTP hyperextension
- K-wire fixation of MTP in neutral for 4-6 weeks post-operatively
Fixed Claw Toe
- PIP joint arthrodesis (most common) - resection of condyles of proximal phalanx + fusion with K-wire; reliably corrects PIP flexion
- PIP excisional arthroplasty (Fowler/DuVries) - resection of condyles without formal fusion; less rigid but quicker recovery
- EDL lengthening / EDB tenotomy - to correct MTP hyperextension
- MTP dorsal capsulotomy + collateral ligament release - for fixed MTP extension/subluxation
- Weil osteotomy (metatarsal shortening) - for MTP subluxation/dislocation; allows anatomical reduction of MTP joint
- Plantar plate repair after Weil osteotomy for MTP subluxation
Claw Toe of the Hallux (Great Toe)
- IP joint arthrodesis + transfer of extensor hallucis longus (EHL) into neck of 1st metatarsal (Jones transfer) + dorsal MTP capsulotomy
- Simple IP arthrodesis alone is insufficient - does not correct MTP hyperextension
Associated Procedures
- Correct hallux valgus if present (50% reduction in recurrence of lesser toe deformity)
- Address underlying pes cavus if causative
Surgical Options Summary Table
| Deformity | Procedure |
|---|---|
| Flexible claw toe | FDL flexor-to-extensor transfer + EDB tenotomy + EDL lengthening |
| Fixed claw toe | PIP arthrodesis + EDL lengthening + MTP capsulotomy |
| Flexible hammer toe | Girdlestone-Taylor FDL transfer or PIP arthroplasty |
| Fixed hammer toe + MTP subluxation | PIP condyle resection + EDL lengthening + MTP capsulotomy ± Weil osteotomy |
| Mallet toe (flexible) | FDL tenotomy |
| Mallet toe (fixed) | Excisional arthroplasty or DIP arthrodesis |
| Hallux claw toe | IP arthrodesis + EHL transfer to 1st MT neck + MTP capsulotomy |
Complications of Surgery
- Recurrence (most common; higher in 2nd toe; reduced by concomitant 1st ray correction)
- Persistent swelling ("sausage toe") - can last months
- Infection (higher with multiple comorbidities)
- Mal-union / non-union of arthrodesis
- Transfer metatarsalgia
- Vascular compromise / avascular necrosis
One page summary on claw toes for university exams mbbs
Claw Toes — One Page MBBS Summary
Definition
- MTP joint → hyperextension
- PIP joint → flexion
- DIP joint → flexion
- Affects all lesser toes (bilateral); always has MTP hyperextension
Distinguish the Three Toe Deformities
| MTP | PIP | DIP | Toes | Cause | |
|---|---|---|---|---|---|
| Claw toe | Extended | Flexed | Flexed | All 4 | Neuromuscular |
| Hammer toe | ±Extended | Flexed | Normal | 1-2 (2nd) | Footwear |
| Mallet toe | Normal | Normal | Flexed | 2nd | FDL contracture |
Pathomechanics — Intrinsic Minus Deformity
↓ Intrinsics → EDL unopposed → MTP hyperextension
→ FDL unopposed → PIP + DIP flexion
Causes
- Charcot-Marie-Tooth disease (+ pes cavus) ← classic
- Diabetic / alcoholic neuropathy
- Poliomyelitis, spinal cord lesions
- Plantar nerve injury, compartment syndrome
- Ill-fitting footwear (narrow toe box, high heels) - F:M 5:1
- Rheumatoid arthritis (plantar plate destruction)
- Hallux valgus (crowding of 2nd toe)
- Trauma, connective tissue disorders
Clinical Features
- MTP hyperextended + PIP flexed + DIP flexed (all lesser toes)
- Hard corn (heloma durum) — dorsum of PIP
- End corn — plantar tip of toe (DIP flexion)
- Plantar callosities under metatarsal heads
- Diabetics/neuropathy → ulceration at pressure points
- Flexible = passively correctable → better prognosis
- Fixed (rigid) = not correctable → bony surgery needed
Investigations
- X-ray (weight-bearing): Joint subluxation, severity, arthritis
- NCS/EMG if neurological cause suspected
- Blood glucose; RF/anti-CCP if inflammatory cause
Treatment
Conservative (First Line — All Stages)
- Wide toe box, low-heeled shoes
- Metatarsal pads (offload MT heads)
- Buddy strapping / toe splints (flexible only)
- Chiropody (corn/callosity debridement)
- Physiotherapy (intrinsic strengthening)
Surgical (Failed Conservative)
- Girdlestone-Taylor procedure — FDL flexor-to-extensor transfer (corrects both IP flexion AND MTP hyperextension) ← procedure of choice
- EDB tenotomy + EDL lengthening
- PIP joint arthrodesis — resect condyles of proximal phalanx + K-wire fusion ← most common
- EDL lengthening + MTP dorsal capsulotomy + collateral ligament release
- Weil osteotomy (metatarsal shortening) for MTP subluxation/dislocation
- IP arthrodesis + Jones transfer (EHL → neck of 1st metatarsal) + MTP capsulotomy
- (Simple IP arthrodesis alone fails — does not correct MTP hyperextension)
Key Points for Exams
- Claw toe = intrinsic minus deformity
- Always MTP hyperextension — this distinguishes it from hammer toe
- Most common neurological cause = Charcot-Marie-Tooth + pes cavus
- Most common non-neurological cause = tight footwear
- Flexible → soft tissue (Girdlestone-Taylor); Fixed → bony (PIP arthrodesis)
- In diabetics: risk of ulceration and osteomyelitis at pressure points
Abductor lurch in one page mbbs
Intracerebral hemorrhage and acute ischemic stroke and leptospirosis
CIDP and multiple sclerosis and brainstorm stroke syndromes