Av malformation after dnc
Reading File
Finding Sources
Searching PubMed
uterine arteriovenous malformation dilation curettage
Reading File
Finding Sources
Searching PubMed
uterine arteriovenous malformation diagnosis management embolization
Loading Image
Finding Sources
Reading Article
PMID: 34130801
Here is a thorough summary of uterine arteriovenous malformation (AVM) after D&C:
Uterine AVM After D&C
What It Is
A uterine AVM is an abnormal direct communication between uterine arteries and veins, bypassing the normal capillary bed. It can be congenital (rare) or acquired - the acquired form is far more common and is closely linked to uterine instrumentation, including:
- Dilation and curettage (D&C)
- Suction evacuation
- Caesarean section
- Endometrial biopsy
- Uterine surgery
The D&C-related form is thought to arise from trophoblastic invasion or traumatic disruption of the myometrium, creating pathological arteriovenous channels. It often occurs after evacuation of products of conception, molar pregnancy, or termination of pregnancy.
Presentation
- Recurrent, sudden, heavy vaginal bleeding - the hallmark symptom - often unprovoked and profuse
- Bleeding typically occurs weeks to months after the D&C
- May follow a period of apparently normal recovery
- Can be life-threatening if a large AVM ruptures
- Importantly, if bleeding persists after D&C and beta-hCG has normalized, AVM should be suspected (rather than retained products of conception)
Diagnosis
First-line: Transvaginal Ultrasound with Color Doppler
The classic finding is a hypoechoic or heterogeneous area within the myometrium adjacent to the endometrium, with:
- Turbulent, high-velocity, low-resistance flow on color Doppler
- Aliasing (color mosaic pattern) - a hallmark sign
- Dilated feeding vessels
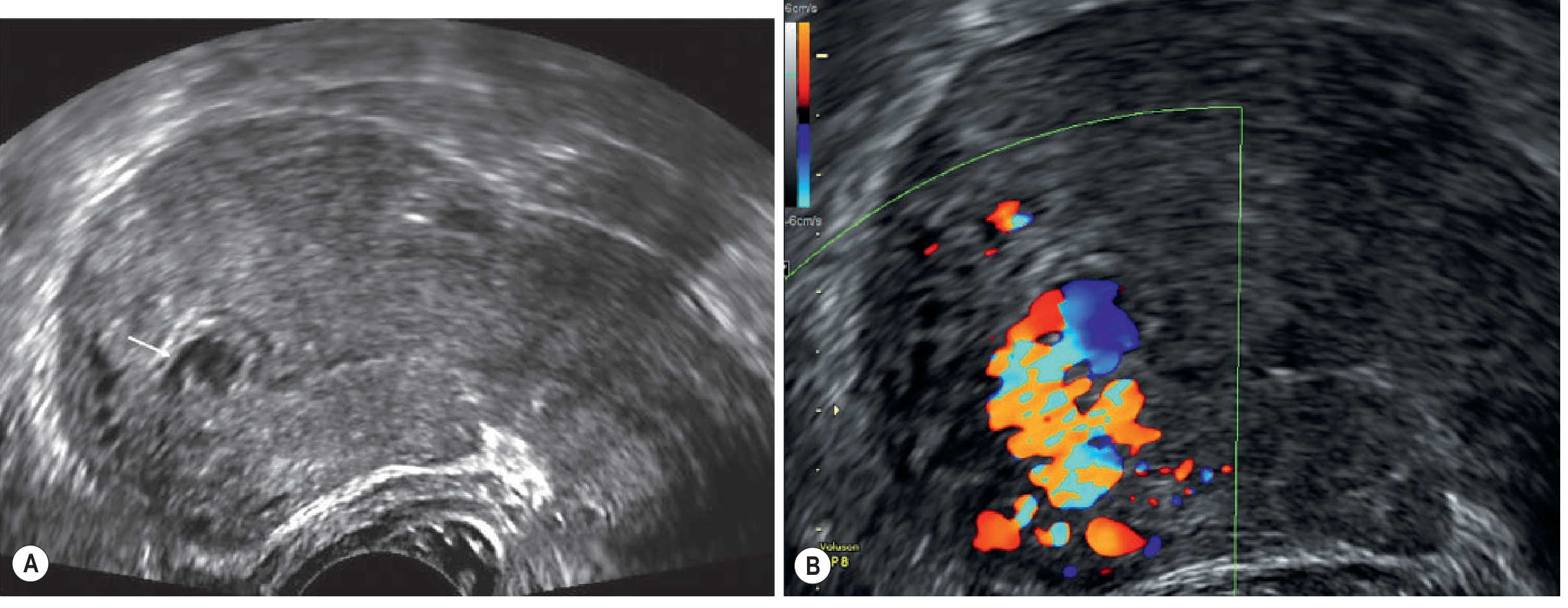
Image: Transvaginal US - (A) focal hypoechoic area; (B) color Doppler aliasing with feeding vessel - classic uterine AVM appearance. Patient had previous surgical removal of retained placenta and presented with recurrent heavy bleeds. (Grainger & Allison's Diagnostic Radiology)
CT Angiography / MRI
- Arterial phase CT shows a hypervascular lesion with early venous opacification
- MRI shows tortuous vessels protruding into the endometrium, with signal voids on T1/T2 weighted sequences and enhancement with contrast
- Selective angiography: shows early venous return (pathognomonic) and can be used therapeutically
Key distinction from retained products of conception (RPOC):
Both can look hypervascular on Doppler, but:
- RPOC typically resolves after b-hCG normalizes
- AVM persists even after b-hCG normalization
- Clinical context (ongoing bleeding, post-D&C) + imaging together guide the diagnosis
(Grainger & Allison's Diagnostic Radiology, p. 917-918)
Management
1. Uterine Artery Embolization (UAE) - First-line for active/severe bleeding
- Selective angiographic embolization is the standard definitive treatment
- The lesion is identified on angiography by early venous return, then embolized with coils or particles
- Preserves fertility in most cases
- High success rate for stopping acute hemorrhage
2. Medical Management - For stable patients or fertility preservation
A 2021 systematic review and meta-analysis (Rosen et al., Fertility and Sterility) found an overall success rate of 88% with medical treatment in 121 women across 32 studies. Agents used:
| Drug | Success Rate | Complication Rate |
|---|---|---|
| Progestins | 82.5% | 10.0% (lowest) |
| GnRH agonists | 89.3% | 10.7% |
| Methotrexate | 90.0% | - |
| Combined hormonal contraception | Included | - |
- No clinical factors reliably predicted success
- 26 subsequent pregnancies reported with no AVM recurrence
- Medical management is reasonable in hemodynamically stable, well-selected patients
3. Surgical Management
- Reserved for cases failing embolization or medical management
- Options: hysteroscopic resection (small AVMs), uterine artery ligation, or as a last resort - hysterectomy
- Blind curettage of a suspected AVM is contraindicated as it can precipitate catastrophic hemorrhage
Key Points Summary
| Feature | Detail |
|---|---|
| Cause after D&C | Traumatic AV fistula formation in myometrium |
| Symptom | Sudden, recurrent, heavy, unprovoked vaginal bleeding |
| Diagnostic clue | Persists after b-hCG normalizes (unlike RPOC) |
| Best first test | Transvaginal USS + color Doppler |
| Gold standard | Selective angiography |
| Treatment of choice | UAE (embolization) |
| Contraindicated | Blind curettage |
| Fertility outcomes | Generally good after UAE or medical management |
Recent evidence note: The Rosen et al. 2021 systematic review (PMID 34130801) supports medical management as a valid option alongside UAE in stable patients. No contradictions to the textbook approach were found in recent literature.
This is a shared conversation. Sign in to Orris to start your own chat.