Lbbb
Reading File
Finding Sources
Searching the Web
LBBB left bundle branch block ECG criteria diagnosis clinical significance 2024
Reading File
Finding Sources
Searching Images
LBBB left bundle branch block ECG
Reading File
Reading File
Loading Image
Loading Image
Reading File
Here is a comprehensive overview of Left Bundle Branch Block (LBBB):
Left Bundle Branch Block (LBBB)
Pathophysiology
In normal conduction, impulses travel equally down both bundles, with the septum activated left to right. When the left bundle is blocked, the impulse travels down the right bundle first, then spreads through the myocardium to activate the left ventricle from right to left. This reverses septal activation and delays left ventricular depolarization.
The major QRS vector is directed left and posteriorly, generating:
- Wide, predominantly negative (QS) complexes in V1
- Entirely positive (R) complexes in V6
(Harrison's Principles of Internal Medicine 22E, p. 1915)
ECG Criteria (Complete LBBB)
| Feature | Finding |
|---|---|
| QRS duration | ≥ 120 ms (complete block) |
| V1 | Deep, broad S waves (QS or rS pattern) |
| Lateral leads (I, aVL, V5, V6) | Broad, notched or slurred monophasic R waves ("M-shaped" or notched R) |
| Septal Q waves | Absent in lateral leads (reversed septal activation) |
| ST-T changes | Discordant — T wave opposite in polarity to the last QRS deflection (secondary repolarization abnormality) |
Incomplete LBBB: QRS 110–120 ms; less commonly associated with structural disease.
Waveform Diagram
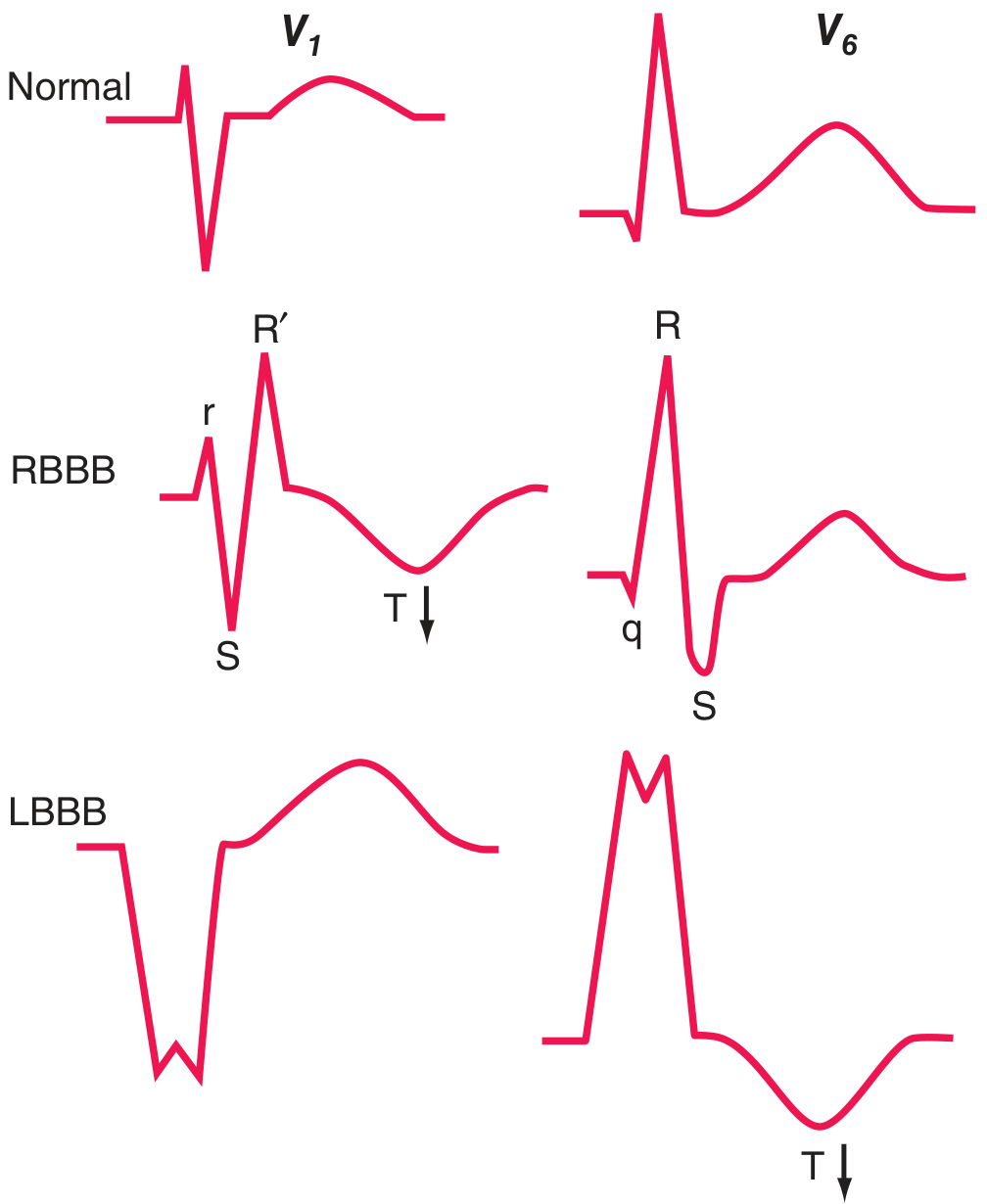
Figure: Comparison of QRS-T patterns — Normal, RBBB, and LBBB in leads V1 and V6. Note the discordant T wave (arrow) in LBBB (V6).
12-Lead ECG Example
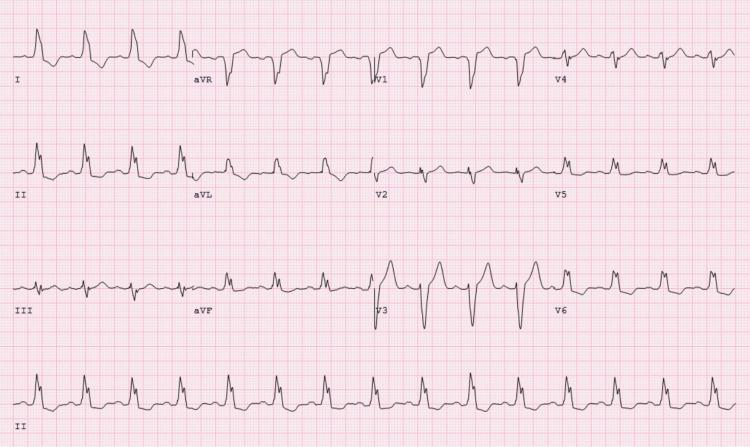
Sinus tachycardia with classic LBBB: wide QRS, deep S waves in V1–V3 with discordant ST elevation, and broad monophasic R waves with notching in lateral leads.
Causes / Associations
LBBB is almost always a marker of structural heart disease. The four major underlying conditions:
- Coronary artery disease (frequently with impaired LV function)
- Hypertensive heart disease
- Aortic valve disease (including post-TAVR)
- Cardiomyopathy (dilated cardiomyopathy especially)
Other causes include severe trauma, fibrosis of the conduction system, and ischemia/infarction.
RBBB is more common in subjects without structural heart disease. LBBB in isolation in a young, asymptomatic patient has weak predictive power, but in an older population it is a significant marker of increased mortality, stroke, and heart failure risk. — Pfenninger & Fowler's Procedures for Primary Care
ST-T Changes: Primary vs. Secondary
- Secondary repolarization abnormality (expected in LBBB): T wave discordant to QRS — this is a normal consequence of altered depolarization sequence.
- Primary repolarization abnormality (ischemia, electrolytes, drugs): T-wave changes independent of QRS. T inversions in right precordial leads (V1–V3) with LBBB may indicate underlying ischemia.
LBBB + Acute MI (Sgarbossa Criteria context)
New or presumed new LBBB in a patient with ischemic chest pain is treated as a STEMI-equivalent:
- ST analysis is obscured by LBBB
- Reperfusion (PCI or thrombolysis) is indicated
- The Sgarbossa criteria help identify MI in the presence of LBBB:
- Concordant ST elevation ≥ 1 mm in leads with positive QRS (most specific)
- Concordant ST depression ≥ 1 mm in V1–V3
- Excessively discordant ST elevation ≥ 5 mm (modified: ST/S ratio ≥ 0.25)
(Goldman-Cecil Medicine, p. 3412)
Rate-Related / Intermittent LBBB
LBBB can be rate-dependent (most often when heart rate exceeds a critical threshold) or intermittent. Waveform patterns identical to LBBB are seen with right ventricular electronic pacing (due to relative delay in LV activation).
Management Implications
| Scenario | Action |
|---|---|
| LBBB + chest pain | Treat as STEMI; urgent reperfusion |
| LBBB + CHF (EF ≤ 35%, QRS ≥ 150 ms) | Cardiac resynchronization therapy (CRT/biventricular pacing) |
| LBBB + syncope with bifascicular block | Pacemaker implantation |
| Asymptomatic LBBB | Stress echo or nuclear perfusion (resting/exercise ECG not interpretable) |
| New LBBB post-TAVR | Monitor for AV block progression |
Fascicular Blocks (Hemiblocks)
Partial left bundle system blocks affect only one fascicle:
- Left anterior fascicular block (LAFB): QRS axis < −45° (marked left axis deviation) — most common cause of marked LAD in adults
- Left posterior fascicular block (LPFB): QRS axis > +110–120° — rare; diagnose only after excluding other causes of right axis deviation
These do not significantly prolong QRS duration and are usually not associated with structural cardiac disease when isolated.
This is a shared conversation. Sign in to Orris to start your own chat.