Anatomy of tracheobronchial tree. Anaesthetic significance. Positions for postural drainage and their significance in pre and post operative care
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Searching Images
tracheobronchial tree anatomy diagram bronchi
Searching Images
postural drainage positions bronchial segments
Loading Image
Loading Image
Searching the Web
postural drainage positions bronchopulmonary segments preoperative postoperative care anaesthesia
I now have comprehensive material to compose a thorough answer. Let me compile everything.
Anatomy of the Tracheobronchial Tree, Anaesthetic Significance, and Postural Drainage
I. ANATOMY OF THE TRACHEOBRONCHIAL TREE
The Trachea
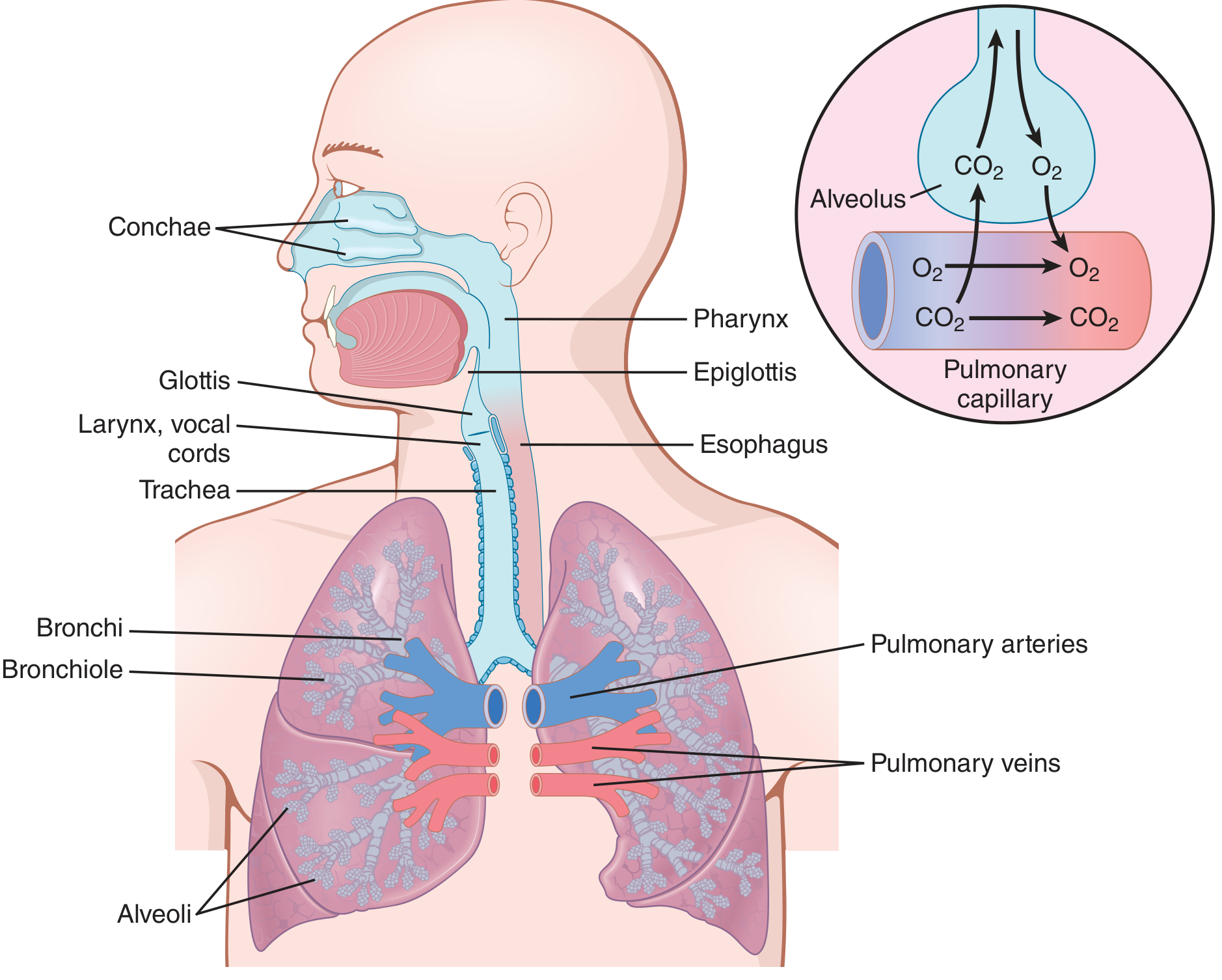
The trachea is a flexible, fibrocartilaginous tube approximately 10–15 cm long in adults. It begins at the lower border of the cricoid cartilage (at the level of C6) and bifurcates at the carina at the level of T4–T5 (behind the sternomanubrial joint).
Structure of the tracheal wall (three layers):
- Mucosa — respiratory epithelium (pseudostratified ciliated columnar) with mixed tracheal glands; cilia beat outwards to clear particles (mucociliary escalator)
- Fibromusculocartilaginous layer — contains 16–20 C-shaped (horseshoe) hyaline cartilage rings that reinforce the anterior and lateral walls; rings are joined by annular ligaments rich in collagen and elastic fibres; the trachealis muscle (smooth muscle) forms the posterior membranous wall and can alter tracheal diameter
- Adventitia — outer sliding connective tissue layer
The transverse diameter is greater than the sagittal diameter. The posterior membranous wall has no cartilage, allowing the oesophagus to bulge into it during swallowing and permitting coughing-related diameter changes.
Blood supply: Inferior thyroid artery branches (cervical trachea); bronchial branches (thoracic trachea).
Nerve supply: Recurrent laryngeal nerve (motor to trachealis; sensory and secretory innervation).
Lymphatics: Paratracheal nodes, superior and inferior tracheobronchial nodes at the carina.
Nerve supply: Recurrent laryngeal nerve (motor to trachealis; sensory and secretory innervation).
Lymphatics: Paratracheal nodes, superior and inferior tracheobronchial nodes at the carina.
The Carina
The carina is a sagittally oriented cartilaginous ridge at the tracheal bifurcation (T4–T5) that projects into the lumen and divides the inspiratory airstream. It is a highly sensitive reflex zone — stimulation triggers coughing and laryngospasm.
Main Bronchi — Key Differences
| Feature | Right Main Bronchus | Left Main Bronchus |
|---|---|---|
| Length | Short (~2.5 cm) | Long (~5 cm) |
| Diameter | Wider | Narrower |
| Angle from trachea | ~20–25° (nearly vertical) | ~40–45° (more horizontal) |
| Distance from carina to upper lobe orifice | 1–2.5 cm | Not applicable (no middle lobe) |
| Lobes supplied | Upper, Middle, Lower | Upper (+ lingula), Lower |
| Bronchopulmonary segments | 10 (right lung) | 8–10 (left lung) |
Bronchopulmonary Segmental Anatomy
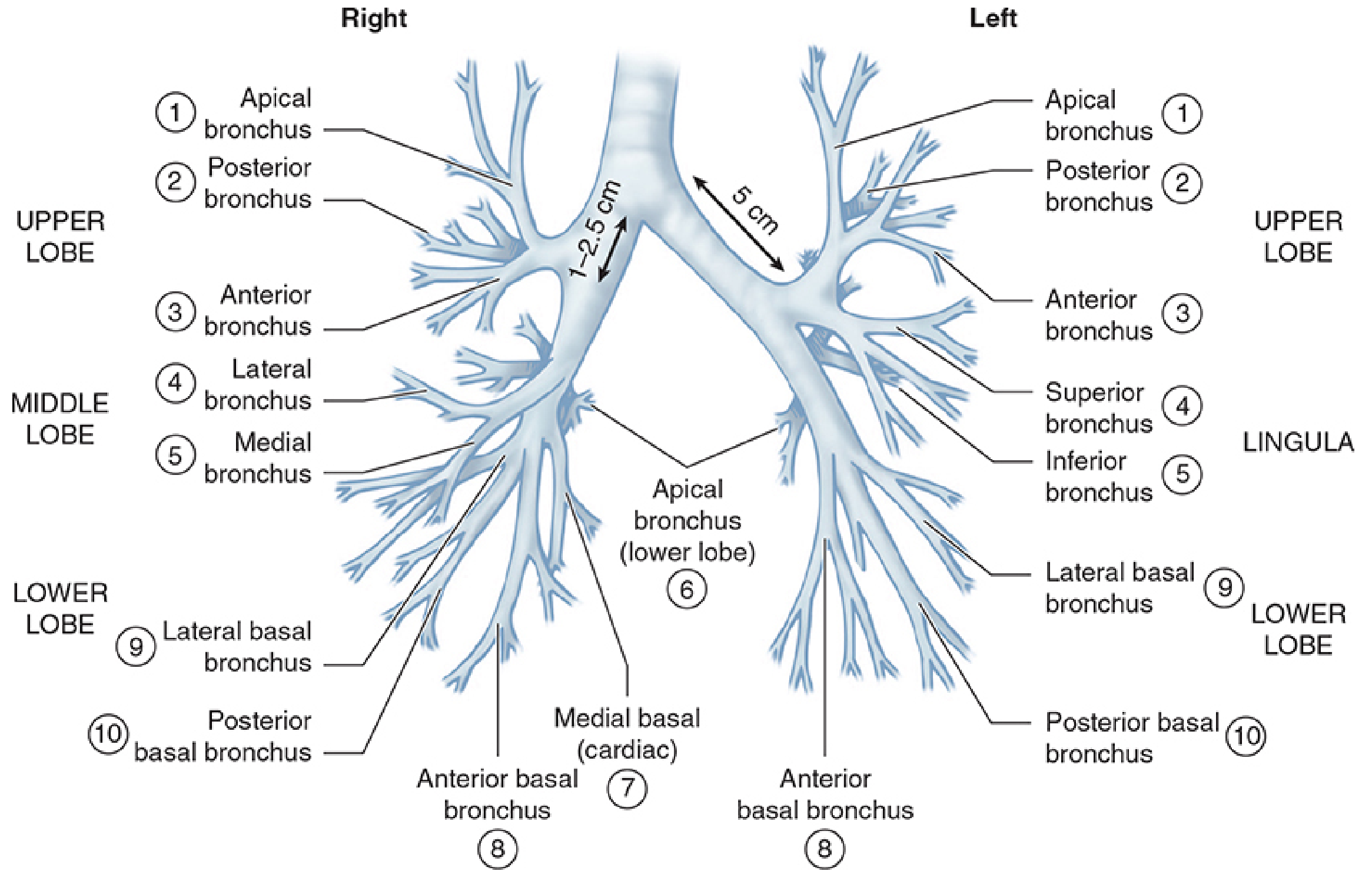
Right lung (10 segments):
- Upper lobe: Apical (1), Posterior (2), Anterior (3)
- Middle lobe: Lateral (4), Medial (5)
- Lower lobe: Apical/Superior (6), Medial basal/Cardiac (7), Anterior basal (8), Lateral basal (9), Posterior basal (10)
Left lung (8–10 segments):
- Upper lobe: Apico-posterior (1+2), Anterior (3)
- Lingula: Superior (4), Inferior (5)
- Lower lobe: Apical/Superior (6), Anteromedial basal (7+8), Lateral basal (9), Posterior basal (10)
Smaller Airways
Beyond the main and lobar bronchi, the tree divides further:
- Segmental bronchi → subsegmental bronchi → terminal bronchioles (no alveoli; conduct air only) → respiratory bronchioles (begin gas exchange) → alveolar ducts → alveolar sacs
- Approximately 65,000 terminal bronchioles in each lung
- Bronchioles (<1.5 mm) lack cartilage; they are kept patent by transpulmonary pressure (tethered open by surrounding alveolar tissue)
Smooth muscle in walls: Sympathetic (β₂-adrenergic) stimulation → bronchodilation; Parasympathetic (vagal, acetylcholine) stimulation → bronchoconstriction
II. ANAESTHETIC SIGNIFICANCE
1. Right Bronchus — Preferential Endobronchial Intubation
The near-vertical angle (~20°) and wider lumen of the right main bronchus means any over-advanced endotracheal tube (ETT) preferentially enters the right main bronchus, resulting in:
- Left lung collapse/atelectasis
- Desaturation, unilateral breath sounds
- Unilateral pulmonary oedema (on reperfusion)
Rule: After intubation, confirm bilateral breath sounds. The cuff should ideally sit just below the vocal cords; in the average adult female the 22 cm mark at the teeth; adult male, ~23 cm. In infants/neonates, the tube should pass only 1–2 cm beyond the glottis to avoid endobronchial intubation.
2. Foreign Body Aspiration
The more vertical orientation of the right main bronchus makes inhaled foreign bodies (and aspirated gastric contents) preferentially enter the right lung — particularly the right lower lobe. This is especially relevant in children.
3. Double-Lumen Tube (DLT) Placement — One-Lung Ventilation
Because of differences in bronchial anatomy between the two sides, DLTs are designed specifically for right or left bronchi:
- Left-sided DLT preferred for most cases (left main bronchus is longer, ~5 cm from carina; greater margin for correct placement)
- Right-sided DLT required for: left pneumonectomy, left sleeve resection, descending thoracic aortic aneurysm compressing left bronchus, left lung transplantation
- The right upper lobe orifice is only 1–2.5 cm from the carina, so right-sided DLTs incorporate a modified side port/cuff slot to ensure right upper lobe ventilation
Confirmation is by fiberoptic bronchoscopy after positioning.
4. Carinal Reflex and Airway Reactivity
- The carina is the most sensitive zone in the tracheobronchial tree; stimulation during light anaesthesia causes coughing, laryngospasm, bronchospasm
- ETT tip resting on the carina → persistent coughing, high airway pressures, inability to ventilate
- Adequate depth of anaesthesia required before endotracheal manipulation
5. The Trachealis Muscle and Airway Dynamics
The posterior membranous trachealis muscle contracts (narrows) during cough (increasing linear velocity to expel secretions). Under anaesthesia:
- Muscle relaxants abolish this mechanism → impaired mucociliary clearance and inability to cough
- This is a key reason for retained secretions postoperatively
6. Mucociliary Clearance
Respiratory epithelial cilia beat at ~1000 beats/min, propelling mucus toward the pharynx. Anaesthesia impairs this by:
- Inhalational agents reduce ciliary beat frequency in a dose-dependent manner
- Dry inspired gases (from ETT breathing circuits without humidification) → ciliary damage → retained secretions
- Smoking → squamous metaplasia + ciliary immobilisation
7. Bronchospasm Under Anaesthesia
The smooth muscle throughout the bronchial tree can go into spasm. Risk factors under anaesthesia:
- Asthma/COPD
- Light anaesthesia with ETT stimulation
- Irritant inhalational agents (e.g., desflurane) vs bronchodilating agents (isoflurane, sevoflurane, halothane)
- Anticholinesterase reversal (neostigmine) → bronchoconstriction; blunted by co-administration of glycopyrrolate/atropine
Treatment: Deepen anaesthesia, β₂-agonists (salbutamol/albuterol), IV ketamine (bronchodilator), IV aminophylline, IV magnesium, IV hydrocortisone.
8. Bronchial Anatomy and Airway Resistance
- The greatest resistance normally resides in medium-sized bronchi near the trachea (few in number), not the terminal bronchioles
- In disease (asthma, COPD), small airway resistance dominates due to smooth muscle contraction, oedema, and mucus — reflected as reduced FEV₁ and increased RV/FRC
III. POSTURAL DRAINAGE — POSITIONS AND SIGNIFICANCE
Definition
Postural drainage is the positioning of a patient so that the target bronchopulmonary segment is placed superior to the carina (and the bronchial orifice), allowing gravity to facilitate drainage of secretions from the peripheral airways to the central airways, where they can be cleared by coughing or suctioning. Positions are held for 3–15 minutes per segment. Chest percussion/vibration is typically combined.
Positions for Each Segment
| Segment | Position |
|---|---|
| Upper lobes — Apical (bilateral) | Sitting upright, leaning slightly back |
| Upper lobe — Posterior (Right) | Lying on left side, rotated 45° face down, pillow support |
| Upper lobe — Posterior (Left) | Lying on right side, rotated 45° face down, shoulders raised ~30 cm |
| Upper lobe — Anterior (bilateral) | Supine (lying flat on back), knees flexed |
| Middle lobe — Lateral & Medial | Right side down, bed tilted head-down 15° |
| Lingula — Superior & Inferior | Left side down, bed tilted head-down 15° |
| Lower lobe — Apical (Superior) | Prone with pillow under abdomen (flat) |
| Lower lobe — Medial basal (Cardiac) | Right side with bed head-down 20° |
| Lower lobe — Anterior basal | Supine, knees flexed, bed head-down 20° |
| Lower lobe — Lateral basal (Right) | Left lateral, head-down 20° |
| Lower lobe — Lateral basal (Left) | Right lateral, head-down 20° |
| Lower lobe — Posterior basal (bilateral) | Prone, pillow under lower abdomen, bed head-down 20° |
Key principle: Upper lobe segments drain in upright/semi-upright positions (gravity already assists); middle and lower lobes require a head-down tilt of 15–20° since they do not benefit from gravity in standard upright or recumbent postures.
Significance in PREOPERATIVE Care
-
Reduction of secretion load — Patients with chronic lung disease (COPD, bronchiectasis, cystic fibrosis, lung abscess, pneumonia) often have retained secretions that increase perioperative complication risk. Preoperative postural drainage reduces this load.
-
Improving pulmonary function — Clearing secretions restores lung compliance, reduces atelectasis, and improves FEV₁/FVC, thereby increasing the physiological reserve before anaesthesia.
-
Antibiotic efficacy — Postural drainage augments the effect of antibiotics by clearing infective material from airways (lung abscess treatment depends critically on postural drainage + antibiotics).
-
Prevention of aspiration pneumonia — In patients with copious secretions, reducing the secretion burden preoperatively lowers the risk of soiling unaffected lung segments during induction or intubation.
-
Combined with chest physiotherapy — Humidification, mucolytics (acetylcysteine), bronchodilators, incentive spirometry, and postural drainage together constitute preoperative respiratory optimisation, which has been shown to reduce postoperative mortality in patients with COPD (from ~17% to ~9%) — Barash, Clinical Anesthesia, 9e.
-
Teaching — Patients are instructed in and practised in postural drainage positions preoperatively so cooperation postoperatively is maximised.
Significance in POSTOPERATIVE Care
-
Prevention of retention collapse (atelectasis) — After general anaesthesia, ciliary activity is depressed, cough reflexes are blunted by residual anaesthetic and muscle relaxant effects, and secretions pool in dependent segments → lobar atelectasis (commonest postoperative pulmonary complication). Postural drainage clears this.
-
Prevention and treatment of postoperative pneumonia — Retained secretions infected by oropharyngeal flora → postoperative pneumonia. Postural drainage, incentive spirometry, and early mobilisation are the cornerstones of prevention.
-
Restoration of FRC — Anaesthesia + supine position reduces FRC; atelectasis and secretion retention worsen this. Postural drainage restores ventilation-perfusion matching and FRC.
-
After thoracic surgery — Especially after lobectomy, pneumonectomy, and bronchiectasis surgery, the residual bronchial tree is at high risk for secretion retention; postural drainage of specific remaining segments prevents empyema and collapse.
-
Modified positions postoperatively — The classic head-down tilt is relatively contraindicated immediately postoperatively because it can:
- Increase intracranial pressure (neurosurgical patients)
- Worsen cardiovascular compromise
- Risk aspiration in patients with unprotected airways
- Cause decreased arterial oxygenation
Therefore, modified (horizontal) postural drainage — achieving the closest approximation of the classical position without head-down tilt — is recommended first in the postoperative period. The head-down position is used with caution only if horizontal positions prove inadequate. -
Postoperative respiratory therapy package — Morgan & Mikhail (Clinical Anesthesiology, 7e) states: "The outcome is favourably influenced by preoperative and postoperative respiratory therapy that includes bronchodilators, incentive spirometry, postural drainage, and pathogen-specific antibiotic therapy."
Contraindications to Postural Drainage
| Absolute/Relative | Condition |
|---|---|
| Relative | Raised intracranial pressure |
| Relative | Active haemoptysis |
| Relative | Uncontrolled hypertension |
| Relative | Recent spinal/thoracic surgery or injury |
| Relative | Oesophageal surgery |
| Relative | Haemodynamic instability |
| Absolute | Patient refusal |
Summary Table: Anaesthetic Significance at a Glance
| Anatomical Feature | Anaesthetic Implication |
|---|---|
| Right bronchus nearly vertical, wider | ETTs and foreign bodies enter right preferentially; endobronchial intubation |
| Carina at T4–T5 | Reference for ETT depth; highly reflexogenic zone |
| Right upper lobe orifice 1–2.5 cm from carina | Right-sided DLT needs special cuff slot; higher malposition risk |
| Left bronchus ~5 cm from carina | Left DLT: safer to position, preferred for most cases |
| Trachealis muscle | Abolition by relaxants → impaired cough + secretion clearance |
| No cartilage in bronchioles | Closure/collapse with smooth muscle spasm (asthma, bronchospasm) |
| Ciliated respiratory epithelium | Impaired by anaesthetic agents → retained secretions → postural drainage essential |
| Innervation: vagus/RLN | Bronchoconstriction risk (parasympathetic stimulation); RLN injury risk during neck/thoracic surgery |
Sources:
- Morgan & Mikhail's Clinical Anesthesiology, 7e (Anatomic Considerations, DLT selection, tracheal intubation)
- Barash, Cullen, Stoelting's Clinical Anesthesia, 9e (Postural drainage, bronchial secretion management)
- Miller's Anesthesia, 10e (Trachea and bronchi; ETT insertion; DLT positioning)
- Guyton & Hall Textbook of Medical Physiology (Trachea, bronchi, bronchioles; airway resistance; autonomic control)
- Color Atlas of Human Anatomy, Vol. 2: Internal Organs (Structural and microscopic anatomy of trachea)
- Fishman's Pulmonary Diseases (Bronchial hygiene, chest physiotherapy)
- AARC Clinical Practice Guideline: Postural Drainage Therapy (Respir Care 1991)
Anatomy of tracheobronchial tree. Anaesthetic significance. Positions for postural drainage and their significance in pre and post operative care
I already covered this topic comprehensively in my previous response. Here is the complete answer again for reference:
Anatomy of the Tracheobronchial Tree, Anaesthetic Significance, and Postural Drainage
I. ANATOMY OF THE TRACHEOBRONCHIAL TREE
The Trachea
The trachea is a flexible fibrocartilaginous tube approximately 10–15 cm long in adults. It begins at the lower border of the cricoid cartilage (C6) and bifurcates at the carina at the level of T4–T5 (behind the sternomanubrial joint).
Structure of the tracheal wall (three concentric layers):
- Mucosa — pseudostratified ciliated columnar (respiratory) epithelium with mixed tracheal glands; cilia beat outward to clear particles (mucociliary escalator)
- Fibromusculocartilaginous layer — 16–20 C-shaped (horseshoe) hyaline cartilage rings reinforcing the anterior and lateral walls; rings joined by elastic annular ligaments; the trachealis muscle (smooth muscle) closes the rings posteriorly, forming the membranous wall
- Adventitia — outer connective tissue sliding layer
The transverse diameter exceeds the sagittal diameter. The posterior membranous wall lacks cartilage, allowing oesophageal bulging during swallowing and tracheal narrowing during coughing (to increase linear velocity of expelled air).
| Feature | Detail |
|---|---|
| Length | 10–15 cm (adult) |
| Cartilage rings | 16–20, C-shaped hyaline |
| Vertebral levels | C6 → T4/T5 |
| Blood supply | Inferior thyroid artery (cervical); bronchial arteries (thoracic) |
| Nerve supply | Recurrent laryngeal nerve (motor + sensory + secretory) |
| Lymphatics | Paratracheal nodes; superior and inferior tracheobronchial nodes at carina |
The Carina
The carina is a sagittally oriented cartilaginous ridge at the tracheal bifurcation (T4–T5) that projects into the lumen and divides the inspiratory airstream. It is the most reflexogenic zone in the tracheobronchial tree — stimulation triggers violent coughing, laryngospasm, and bronchospasm.
Main Bronchi — Key Differences
| Feature | Right Main Bronchus | Left Main Bronchus |
|---|---|---|
| Length | Short (~2.5 cm) | Long (~5 cm) |
| Diameter | Wider | Narrower |
| Angle from trachea | ~20–25° (nearly vertical) | ~40–45° (more horizontal) |
| Distance carina → upper lobe orifice | 1–2.5 cm | ~5 cm (no middle lobe) |
| Lobes supplied | Upper, Middle, Lower | Upper (+ lingula), Lower |
| Bronchopulmonary segments | 10 | 8–10 |
Bronchopulmonary Segmental Anatomy
Right lung (10 segments):
- Upper lobe: Apical (1), Posterior (2), Anterior (3)
- Middle lobe: Lateral (4), Medial (5)
- Lower lobe: Apical/Superior (6), Medial basal/Cardiac (7), Anterior basal (8), Lateral basal (9), Posterior basal (10)
Left lung (8–10 segments):
- Upper lobe: Apico-posterior (1+2), Anterior (3)
- Lingula: Superior (4), Inferior (5)
- Lower lobe: Apical/Superior (6), Anteromedial basal (7+8), Lateral basal (9), Posterior basal (10)
Smaller Airways
The bronchial tree divides progressively:
Main bronchi → Lobar bronchi → Segmental bronchi → Subsegmental bronchi → Terminal bronchioles → Respiratory bronchioles → Alveolar ducts → Alveolar sacs
Key physiological points:
- Bronchi (>1.5 mm): contain cartilage plates; kept open by structural rigidity
- Bronchioles (<1.5 mm): no cartilage; kept open by transpulmonary tethering forces from surrounding alveoli
- ~65,000 terminal bronchioles per lung
- Smooth muscle present throughout; absent only in terminal respiratory bronchioles and alveolar walls
- Greatest normal airway resistance: medium bronchi near the trachea (few in number); in disease (asthma, COPD) small airway resistance dominates
Autonomic control of bronchial smooth muscle:
- Sympathetic (β₂-adrenergic): bronchodilation — epinephrine, salbutamol
- Parasympathetic (vagal, acetylcholine): bronchoconstriction — mild normally, exaggerated in disease and by anaesthetic stimulation
II. ANAESTHETIC SIGNIFICANCE
1. Endobronchial Intubation — Right Bronchus Preference
The near-vertical angle and wider lumen of the right main bronchus means any over-advanced ETT preferentially enters the right main bronchus, causing:
- Left lung collapse/atelectasis → falling SpO₂
- Absent breath sounds on left
- Unilateral pulmonary oedema (reperfusion injury on extubation)
Clinical rule: After intubation, confirm equal bilateral breath sounds. Standard depth: ~21 cm at teeth in adult females, ~23 cm in males. In infants/neonates, the ETT tip should pass only 1–2 cm beyond the glottis.
2. Foreign Body Aspiration
The more vertical right bronchus directs aspirated foreign bodies preferentially into the right lung (especially right lower lobe). Equally relevant to aspiration of gastric contents during induction — risk of right lower lobe aspiration pneumonia. This underscores the importance of:
- Rapid sequence induction (RSI) with cricoid pressure in at-risk patients
- Head-up position during induction
3. Double-Lumen Tube (DLT) and One-Lung Ventilation
Critical knowledge for thoracic anaesthesia:
| Feature | Left-sided DLT | Right-sided DLT |
|---|---|---|
| Preference | Most cases (longer left bronchus = safer margin) | Specific indications only |
| Indication for right-sided | Left pneumonectomy, left sleeve resection, left lung transplant, left bronchial mass, descending thoracic aortic aneurysm compressing left bronchus | — |
| Special design needed | No | Yes — side port/slot in endobronchial cuff for right upper lobe ventilation |
| Challenge | — | Right upper lobe orifice only 1–2.5 cm from carina → easy malposition → right upper lobe collapse |
Confirmation: Fiberoptic bronchoscopy after placement is gold standard.
4. Carinal Reflex and Stimulation
- The carina is the most sensitive trigger zone; under light anaesthesia, contact with the ETT tip or suction catheter causes coughing, laryngospasm, bronchospasm, and arrhythmias (including bradycardia via vagal reflex)
- ETT tip resting on carina → high airway pressures, bilateral inadequate ventilation, persistent bucking
- Adequate anaesthetic depth must be established before any endotracheal manipulation
5. Trachealis Muscle and Impaired Cough
The posterior trachealis muscle contracts during coughing, dramatically narrowing the trachea and increasing linear air velocity to expel secretions. Under general anaesthesia:
- Neuromuscular blockade abolishes the cough mechanism entirely
- Residual neuromuscular block postoperatively → weak cough → secretion retention
- This is a primary driver of postoperative atelectasis and pneumonia
6. Mucociliary Clearance — Anaesthetic Impairment
| Insult | Effect |
|---|---|
| Inhalational anaesthetic agents | Dose-dependent reduction in ciliary beat frequency |
| Dry, unhumidified gases via ETT | Ciliary desiccation and damage |
| High FiO₂ (oxygen toxicity) | Mucosal damage |
| Opioids | Suppress cough reflex |
| Smoking history | Squamous metaplasia + ciliary immobilisation |
All these factors together mean that mucociliary clearance is severely impaired perioperatively, making postural drainage, chest physiotherapy, and early mobilisation essential in postoperative care.
7. Bronchospasm Under Anaesthesia
The bronchial smooth muscle can respond with spasm under anaesthesia, especially in susceptible patients.
Triggers: Endotracheal intubation under light anaesthesia; aspiration; secretions; certain drugs (neostigmine, β-blockers, morphine, NSAIDs in aspirin-sensitive asthma).
Anaesthetic agents and bronchomotor tone:
- Bronchodilating: isoflurane, sevoflurane, halothane, ketamine
- Neutral/mildly irritant: propofol (actually blunts airway reflexes)
- Irritant (avoid in asthmatics): desflurane (increases airway resistance by 30–40%)
Management of intraoperative bronchospasm:
- Deepen anaesthesia (sevoflurane, propofol, ketamine)
- Inhaled β₂-agonist (salbutamol via ETT)
- IV aminophylline (5–7 mg/kg loading dose over 20 min)
- IV hydrocortisone
- IV magnesium sulphate
- Rule out mechanical causes (ETT tip at carina, endobronchial intubation, secretions)
8. Preoperative Respiratory Optimisation — Summary
Barash (Clinical Anesthesia, 9e) notes that adequate hydration decreases viscosity of secretions and facilitates removal. The perioperative respiratory therapy package includes:
- Bronchodilators
- Mucolytics (acetylcysteine/Mucomyst)
- Humidification
- Postural drainage
- Incentive spirometry
- Pathogen-specific antibiotics
- Smoking cessation (≥8 weeks before elective surgery for maximal benefit)
This package reduces postoperative pulmonary complication rates in COPD patients significantly.
III. POSTURAL DRAINAGE — POSITIONS AND SIGNIFICANCE
Definition and Principle
Postural drainage (gravity-assisted drainage) is the positioning of a patient such that the target bronchopulmonary segment is placed superior to the carina, allowing gravity to drain secretions from peripheral airways toward central airways for removal by coughing or suctioning.
Each position is held for 3–15 minutes. Chest percussion (cupping), vibration, and active coughing are performed concurrently to maximise effect.
Key principle: Upper lobes drain in upright/semi-upright postures (gravity already assists in routine positions). Middle lobe and lingula require a 15° head-down tilt. Lower lobes require a 20° head-down tilt because they lie below the carina in standard postures.
Positions for Each Bronchopulmonary Segment
| Lobe | Segment | Drainage Position |
|---|---|---|
| Upper Lobe | Apical (bilateral) | Sitting upright, leaning slightly back against pillow |
| Upper Lobe | Posterior — Right | Lying on left side, rotated 45° face-down, pillow support |
| Upper Lobe | Posterior — Left | Lying on right side, rotated 45° face-down, shoulders raised ~30 cm |
| Upper Lobe | Anterior (bilateral) | Supine (flat), knees flexed |
| Middle Lobe | Lateral & Medial | Right side down, bed tilted head-down 15° |
| Lingula | Superior & Inferior | Left side down, bed tilted head-down 15° |
| Lower Lobe | Apical/Superior (bilateral) | Prone with pillow under abdomen, bed flat |
| Lower Lobe | Medial basal (Cardiac) — Right | Right lateral, bed tilted head-down 20° |
| Lower Lobe | Anterior basal (bilateral) | Supine, knees flexed, bed tilted head-down 20° |
| Lower Lobe | Lateral basal — Right | Left lateral, bed tilted head-down 20° |
| Lower Lobe | Lateral basal — Left | Right lateral, bed tilted head-down 20° |
| Lower Lobe | Posterior basal (bilateral) | Prone, pillow under lower abdomen, bed tilted head-down 20° |
Significance in PREOPERATIVE Care
1. Secretion clearance and reduction of infective load
Patients with chronic bronchitis, bronchiectasis, cystic fibrosis, lung abscess, or recurrent pneumonia carry a heavy secretion burden. Preoperative postural drainage reduces this significantly, decreasing the risk of intraoperative aspiration of purulent material into healthy segments and postoperative infection.
2. Improvement of pulmonary function
Clearing retained secretions restores ventilation-perfusion matching, improves lung compliance, and optimises preoperative spirometry values (FEV₁, FVC). This directly expands the margin of physiological reserve.
3. Synergy with antibiotics
In lung abscess, postural drainage is a cornerstone of treatment — antibiotics alone are often inadequate without mechanical drainage of the cavity. Preoperatively, this reduces cavity size and controls sepsis.
4. Risk stratification and anaesthetic planning
The volume and character of sputum assessed during postural drainage sessions helps quantify the degree of airway disease, guide anaesthetic technique selection (e.g., DLT use for one-lung isolation to protect the healthy lung), and plan postoperative ICU requirements.
5. Patient education and compliance
Practising positions and deep breathing exercises preoperatively significantly improves postoperative compliance, as the patient is already familiar and coordinated with the technique.
6. Outcome evidence
Morgan & Mikhail (Clinical Anesthesiology, 7e) states the outcome in patients with chronic lung disease is "favourably influenced by preoperative and postoperative respiratory therapy that includes bronchodilators, incentive spirometry, postural drainage, and pathogen-specific antibiotic therapy." Studies show reduced postoperative mortality in COPD patients from ~17% (untreated) to ~9% (treated with preoperative respiratory optimisation).
Significance in POSTOPERATIVE Care
1. Prevention and reversal of atelectasis (retention collapse)
The commonest postoperative pulmonary complication is lobar or segmental atelectasis from retained secretions. Causes include:
- Depressed cough (opioids, residual muscle relaxant, pain splinting)
- Reduced mucociliary clearance (inhalational agents, dry gases)
- Reduced FRC (supine position, upper abdominal/thoracic incision)
- Increased secretion viscosity (dehydration)
Postural drainage + percussion + incentive spirometry reverses this.
2. Prevention of postoperative pneumonia
Retained secretions become colonised → pneumonia. Postural drainage, early mobilisation, and chest physiotherapy are the primary preventive strategies.
3. Restoration of FRC and V/Q matching
Atelectasis and secretion pooling reduce FRC and create intrapulmonary shunting (V/Q = 0). Postural drainage of dependent segments restores alveolar ventilation and improves PaO₂.
4. After thoracic surgery
After lobectomy, pneumonectomy, or bronchiectasis surgery, the residual bronchial tree must be drained aggressively to prevent empyema, bronchopleural fistula, and stump breakdown.
5. Modified positions — postoperative adaptation
Classical head-down tilt positions are relatively contraindicated immediately postoperatively because they can:
- Increase intracranial pressure (especially after neurosurgery, head injury)
- Cause cardiovascular compromise (reduced venous return in hypovolaemic patients)
- Risk regurgitation and aspiration in patients with unprotected airways
- Cause respiratory distress and hypoxaemia
Therefore, modified (horizontal) postural drainage is used first — achieving the closest approximation to the classical position without head-down tilt, using lateral decubitus and prone positions with the bed flat. Head-down tilt is introduced gradually and with caution only when horizontal positions prove insufficient.
6. Timing and frequency
Typically performed 2–4 times daily postoperatively. Each session should include: positioning → percussion/vibration (3–5 minutes per segment) → encouraged coughing or suctioning → rest. Combined with early ambulation, which independently improves secretion clearance.
Contraindications to Postural Drainage
| Category | Condition |
|---|---|
| Absolute | Patient refusal; untreated tension pneumothorax |
| Relative | Raised intracranial pressure (avoid head-down) |
| Relative | Active massive haemoptysis |
| Relative | Uncontrolled hypertension or haemodynamic instability |
| Relative | Recent spinal injury or surgery |
| Relative | Recent oesophageal anastomosis |
| Relative | Acute pulmonary oedema |
| Relative | Pulmonary embolism (acute phase) |
Summary — Anaesthetic Significance at a Glance
| Anatomical Feature | Anaesthetic Implication |
|---|---|
| Right bronchus nearly vertical, wider | ETT and foreign bodies preferentially enter right; risk of endobronchial intubation |
| Carina at T4–T5 | Reference for ETT depth; highly reflexogenic (laryngospasm, bronchospasm, bradycardia) |
| Right upper lobe orifice 1–2.5 cm from carina | Right-sided DLT requires side port; higher malposition risk |
| Left main bronchus ~5 cm from carina | Left-sided DLT preferred; safer positioning margin |
| Trachealis muscle | Neuromuscular blockade abolishes cough; retained secretions; postural drainage essential |
| No cartilage in bronchioles | Collapse with smooth muscle spasm; bronchospasm in asthma/COPD |
| Ciliated respiratory epithelium | Impaired by anaesthetic agents, dry gases, opioids → retained secretions |
| Vagal innervation | Bronchoconstriction risk; neostigmine → bronchospasm; use glycopyrrolate |
| Recurrent laryngeal nerve supply | RLN injury risk in thyroid, neck, thoracic aortic surgery → vocal cord palsy |
Sources:
- Morgan & Mikhail's Clinical Anesthesiology, 7e
- Barash, Cullen, Stoelting's Clinical Anesthesia, 9e
- Miller's Anesthesia, 10e
- Guyton & Hall Textbook of Medical Physiology
- Color Atlas of Human Anatomy, Vol. 2: Internal Organs
- Fishman's Pulmonary Diseases and Disorders
- AARC Clinical Practice Guideline: Postural Drainage Therapy
This is a shared conversation. Sign in to Orris to start your own chat.