Korokoffs sounds and how to measure bp
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Finding Sources
Loading Image
Finding Sources
Reading File
I now have comprehensive information from multiple authoritative textbooks. Let me compile the full answer.
Korotkoff Sounds and Blood Pressure Measurement
What are Korotkoff Sounds?
Korotkoff sounds are the sounds heard through a stethoscope over the brachial artery during auscultatory blood pressure measurement. They are named after Nikolai Korotkoff, a Russian physician who first described them in 1905.
Mechanism: When a BP cuff is inflated above systolic pressure, the brachial artery is completely collapsed and no sound is heard. As the cuff is slowly deflated, blood begins to jet through the partially occluded vessel at peak systole, creating turbulent flow. This turbulence causes vibration of the arterial wall, producing the characteristic sounds. Under normal open-flow conditions, blood moves in laminar flow, which produces no sound. - Guyton and Hall Textbook of Medical Physiology, p. 191
The 5 Phases of Korotkoff Sounds
| Phase | Character | Clinical Significance |
|---|---|---|
| Phase I | First appearance of clear, repetitive tapping sounds | = Systolic BP |
| Phase II | Sounds become softer and longer (swishing quality) | Cuff slightly below systolic; reduced turbulence |
| Phase III | Sounds become louder and crisper again | Blood passing more freely |
| Phase IV | Sounds suddenly become muffled (low-pitched, blowing) | Approaches diastolic; still some vessel compression |
| Phase V | Complete disappearance of all sounds | = Diastolic BP (standard clinical reading) |
- SBP = Phase I (first tapping sound heard)
- DBP = Phase V (sounds completely disappear) - Washington Manual of Medical Therapeutics; Fuster & Hurst's The Heart, 15th Ed.
Exception: When sounds do not disappear but persist down to 0 mmHg (e.g., aortic regurgitation, hyperdynamic states), Phase IV (muffling) is used as the diastolic pressure. - Washington Manual of Medical Therapeutics
Auscultatory Gap
In some patients (especially older hypertensives), Korotkoff sounds may disappear and then reappear at lower pressures - this is the "auscultatory gap." It can span up to 25 mmHg and cause underestimation of true systolic BP. To avoid this, palpate the radial pulse while inflating the cuff to confirm the true obliteration pressure. - Fuster & Hurst's The Heart, 15th Ed.
How to Measure Blood Pressure (Step-by-Step)
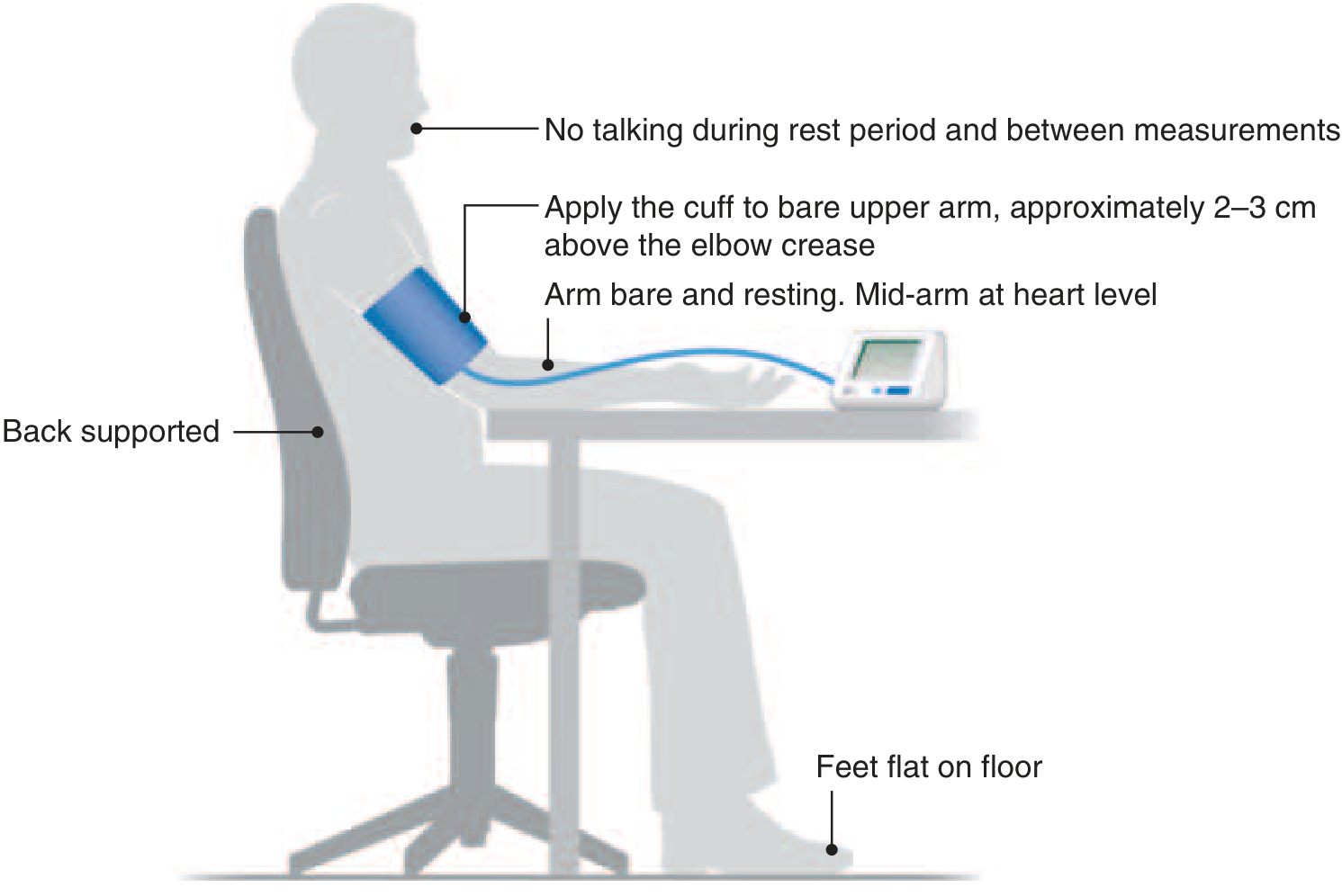
Patient Preparation
- Patient should rest quietly for 3-5 minutes before measurement
- Avoid caffeine, smoking, alcohol, or exercise for at least 30 minutes prior
- Empty the bladder; avoid a full bladder
- No talking during the rest period or measurements
- Seat with back supported, feet flat on the floor - Harrison's Principles of Internal Medicine, 22nd Ed.
Equipment
- Use a clinically validated sphygmomanometer
- Cuff size: The inflatable bladder width should be ~40% of arm circumference; the bladder should encircle at least 80% of the arm. A cuff that is too small gives a falsely high reading.
- Place the cuff on the bare upper arm, approximately 2-3 cm above the antecubital fossa (elbow crease)
- Mid-arm (cuff center) should be at heart level
Technique
- Palpate the radial pulse; inflate the cuff until the pulse disappears, then add 20-30 mmHg more (this sets the inflation target and helps avoid missing the auscultatory gap)
- Place the stethoscope diaphragm lightly over the brachial artery at the antecubital fossa
- Deflate the cuff slowly at ~2 mmHg/second
- Note the pressure at the first appearance of tapping sounds (Phase I) = Systolic BP
- Continue deflating - note the pressure at complete disappearance of sounds (Phase V) = Diastolic BP
- Deflate completely and remove cuff
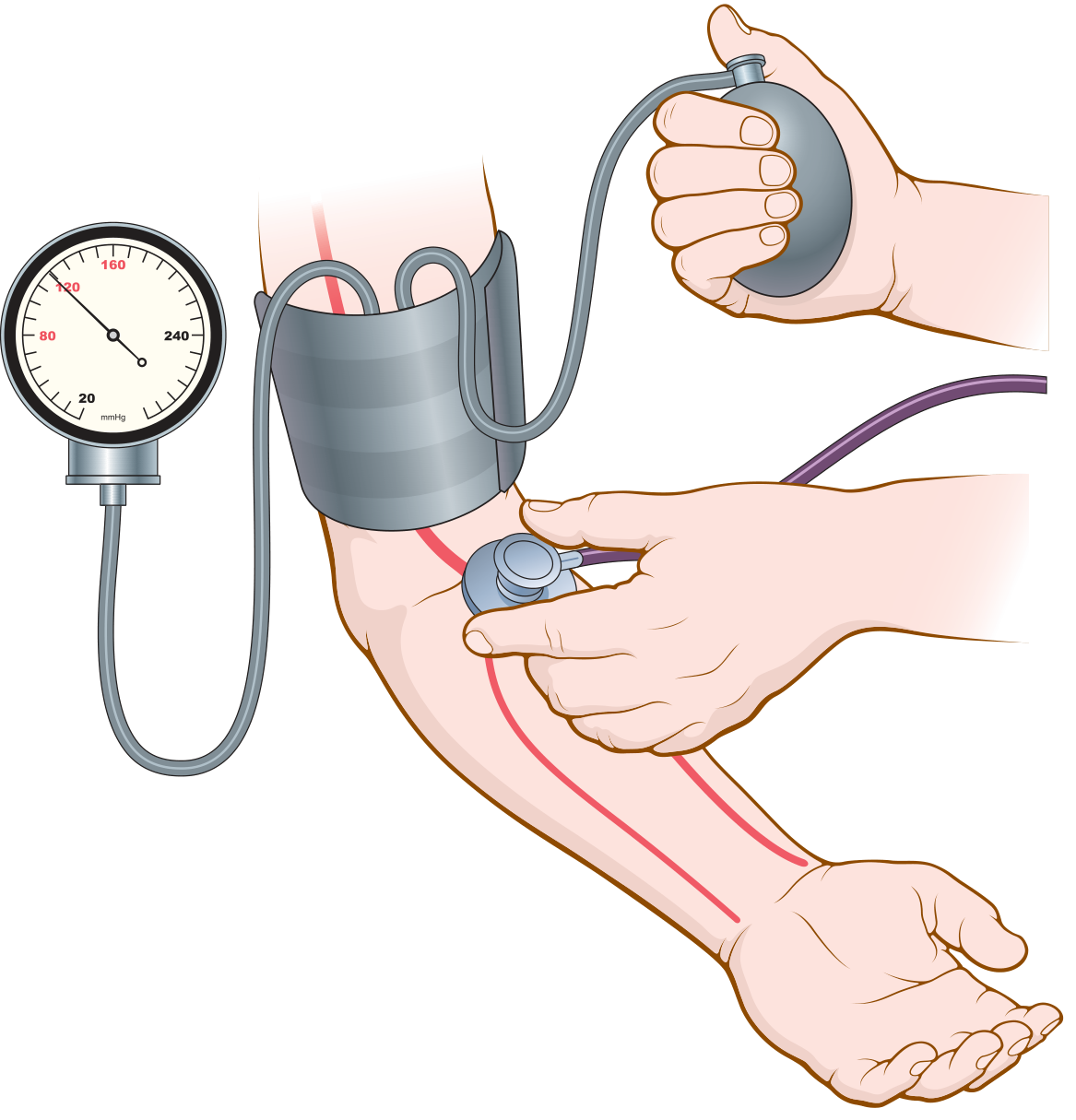
Figure: Auscultatory method for measuring systolic and diastolic pressures - Guyton & Hall Medical Physiology
Repeat and Record
- Take two readings separated by 2 minutes; average them
- Measure in both arms at the initial visit; use the arm with the higher reading
- In orthostatic hypotension workup: measure supine, sitting, and standing (normally systolic BP should not fall >20 mmHg on standing)
- In coarctation of the aorta: lower extremity BP is normally 10-20 mmHg higher than upper extremity; a lower reading suggests coarctation - Fuster & Hurst's The Heart, 15th Ed.
Automated (Oscillometric) Method
Modern digital cuffs use an electronic pressure sensor to detect oscillations in cuff pressure rather than sound. As the cuff deflates:
- Maximum oscillation amplitude corresponds to mean arterial pressure (MAP)
- Algorithms calculate systolic and diastolic values from the oscillation pattern
Advantages: requires less skill, usable at home, avoids "white-coat effect."
Limitations: can be inaccurate with inappropriate cuff size, severe atherosclerosis, or very irregular rhythms. They cannot detect pulsus paradoxus or pulsus alternans - manual auscultation is still needed for these. - Guyton & Hall, p. 191-192; Fuster & Hurst's The Heart, 15th Ed.
ACC/AHA BP Classification (Adults)
| Category | Systolic (mmHg) | Diastolic (mmHg) | |
|---|---|---|---|
| Normal | < 120 | and | < 80 |
| Elevated | 120-129 | and | < 80 |
| Stage 1 HTN | 130-139 | or | 80-89 |
| Stage 2 HTN | ≥ 140 | or | ≥ 90 |
- Harrison's Principles of Internal Medicine, 22nd Ed.
Common Errors and How to Avoid Them
| Error | Effect | Prevention |
|---|---|---|
| Cuff too small | Falsely high BP | Use correct cuff size |
| Arm below/above heart level | Falsely high/low BP | Position arm at heart level |
| Missing auscultatory gap | Underestimation of SBP | Palpate radial pulse first |
| Deflating cuff too fast | Missed readings | Deflate at 2 mmHg/sec |
| Patient talking or tense | Falsely elevated BP | Rest 3-5 min; no talking |
| Stiff vessels (atherosclerosis) | Altered Korotkoff sounds | Consider intra-arterial measurement if needed |
This is a shared conversation. Sign in to Orris to start your own chat.