Apporach to a case of carcinoma ano rectum
Reading File
Finding Sources
Finding Sources
Searching PubMed
"rectal cancer" AND "management"
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the information needed for a comprehensive answer. Here is the full clinical approach to carcinoma of the ano-rectum:
Approach to Carcinoma of the Ano-Rectum
This topic covers two distinct entities that require different approaches: carcinoma of the rectum (predominantly adenocarcinoma) and carcinoma of the anal canal/margin (predominantly squamous cell carcinoma). Both are discussed below.
PART A: CARCINOMA OF THE RECTUM
Anatomy & Definition
The rectum extends 12-15 cm from the anorectal ring to the rectosigmoid junction. Rectal cancer specifically refers to tumors at or below the peritoneal reflection. From a surgical perspective, the unique challenge is the bony confines of the pelvis and proximity to vital structures (bladder, prostate/vagina, sacral plexus, ureters). - Current Surgical Therapy 14e
Histological Types
- Adenocarcinoma - >95% of rectal tumors
- Mucinous adenocarcinoma (~17% of CRCs - note: no FDG uptake on PET)
- Signet ring cell carcinoma (rare, poor prognosis)
Clinical Presentation
| Symptom | Notes |
|---|---|
| Change in bowel habits | Most common presentation |
| Rectal bleeding (PR bleed) | Often mixed with stool, differentiates from hemorrhoids |
| Tenesmus | Sensation of incomplete evacuation; late finding |
| Change in stool caliber | "Pencil thin" stools |
| Rectal pain | Late finding - indicates locally invasive disease |
| Colicky abdominal pain | With rectosigmoid obstruction |
| Weight loss | Almost always indicates metastatic disease |
| Symptoms of anterior invasion | Pneumaturia, fecaluria (bladder), vaginal discharge/fistula |
| Severe intractable back pain | Posterior sacral plexus infiltration |
- Bailey & Love's Short Practice of Surgery 28th Edition
Modes of Spread
1. Local Spread
Occurs circumferentially rather than longitudinally. After penetrating the muscularis, it spreads into the mesorectum (limited initially by mesorectal fascia), then into:
- Anteriorly: prostate, seminal vesicles, bladder (male); vagina, uterus (female)
- Laterally: ureter
- Posteriorly: sacrum and sacral plexus
2. Lymphatic Spread
- Above the peritoneal reflection: upward along superior rectal vessels
- Below the peritoneal reflection: predominantly upward, but ~20% lateral spread to pelvic wall nodes
- Downward spread (to inguinal nodes) is rare and limited to the distal 1-2 cm of anal canal
3. Haematogenous Spread
Via portal vein -> liver (most common). Rectal cancer also has increased lung metastases via systemic veins compared to colon cancer.
4. Transperitoneal Spread - peritoneal seedlings/carcinomatosis
- Bailey & Love's Short Practice of Surgery 28th Edition
Investigations
Diagnostic Workup
-
Digital Rectal Examination (DRE)
- Irregular, hard, elevated/ulcerated endoluminal mass
- Assess mobility (mobile vs. tethered vs. fixed)
- Measure distance of lower margin from top of anal sphincter complex
- Assess sphincter integrity (critical for anastomosis planning)
- In females: vaginal exam to assess posterior vaginal wall
-
Rigid Proctoscopy
- Preferred method for accurate distance measurement from anal verge
- Tumors within 12-15 cm of anal verge = rectal cancer
- On flexible endoscopy: at or below the third fold
-
Colonoscopy + Biopsy
- Full colorectal visualization is preferred
- Rules out synchronous tumors (risk 3-5%)
- Biopsy for tissue diagnosis
-
CEA (Carcinoembryonic Antigen)
- Not diagnostic, but useful for prognosis and post-treatment surveillance baseline
Staging Investigations
Local/Regional Staging:
- MRI Pelvis (preferred) - High-resolution T2-weighted images assess:
- Depth of tumor invasion (T stage)
- Circumferential resection margin (CRM) - critical for surgical planning
- Mesorectal fascia involvement
- Locoregional lymph nodes
- Extramural vascular invasion (EMVI)
- Endorectal Ultrasound (EUS) - alternative if MRI contraindicated; limited by bulky disease, posterior tumors, and operator dependence
Systemic Staging:
- CT chest, abdomen and pelvis - standard for distant metastasis workup
- PET-CT - not routine initial staging, but useful in equivocal CT/MRI findings, detecting nodal disease (improves N-staging accuracy from 48% to 66%)
All patients require: DRE + colonoscopy with biopsy + CT CAP + pelvic MRI. - Bailey & Love's, Current Surgical Therapy 14e
Staging Systems
TNM Staging (AJCC 8th Edition - Current Standard)
| T Stage | Description |
|---|---|
| T1 | Submucosa |
| T2 | Muscularis propria |
| T3 | Through muscularis propria into perirectal tissue |
| T4a | Penetrates visceral peritoneum |
| T4b | Invades adjacent organs |
| N Stage | Description |
|---|---|
| N0 | No regional nodes |
| N1 | 1-3 regional nodes |
| N2 | ≥4 regional nodes |
Dukes Classification (Historical but widely used)
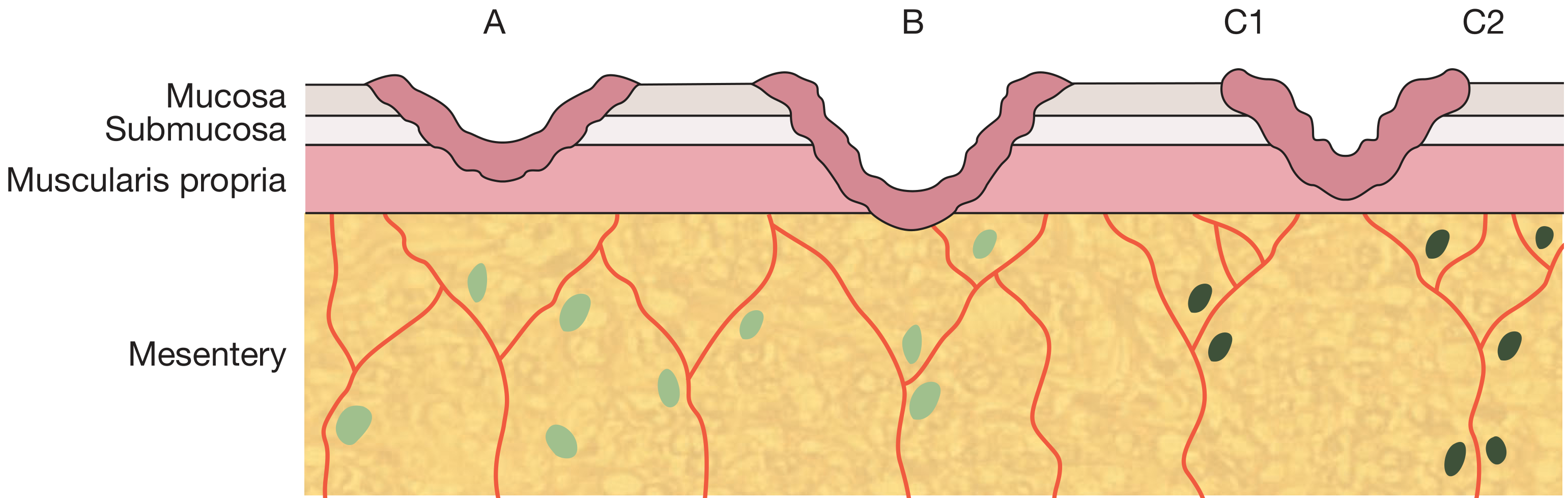
| Stage | Description |
|---|---|
| A | Confined to bowel wall |
| B | Penetrates muscularis propria |
| C1 | Pararectal lymph nodes involved |
| C2 | Apical nodes involved |
- Bailey & Love's Short Practice of Surgery 28th Edition
Multidisciplinary Team (MDT)
Management must be discussed in an MDT setting involving:
- Colorectal surgeons
- Radiologists
- Medical and radiation oncologists
- Pathologists
- Stoma care nurses
- The treatment decision is made jointly with the patient
Treatment
Neoadjuvant Therapy (Before Surgery)
| Approach | Indication |
|---|---|
| Long-course chemoradiotherapy (CRT) | Locally advanced disease (T3/T4 or threatened CRM); 5 fractions over 6 weeks + 5-FU/capecitabine |
| Short-course radiotherapy (SCRT) | High-risk for local recurrence (e.g., perirectal node involvement) but margins not threatened; 5 Gy x 5 days |
| Total Neoadjuvant Therapy (TNT) | Combines chemotherapy (FOLFOX) + CRT before surgery - increasingly preferred for LARC |
~20% achieve complete clinical response (cCR) to neoadjuvant CRT - these patients may be candidates for "Watch and Wait" (Habr-Gama protocol).
Surgical Options
1. Total Mesorectal Excision (TME) - Gold standard
- En-bloc removal of the rectum with its surrounding mesorectal envelope
- Critical for oncologic clearance; reduces local recurrence from ~30% to <10%
2. Anterior Resection (AR)
- For tumors of upper and middle rectum
- Colorectal or coloanal anastomosis with circular stapler (double-stapling technique)
- Defunctioning loop ileostomy usually fashioned
3. Low Anterior Resection (LAR)
- For low rectal tumors with adequate distal margin
- May require coloanal anastomosis (CAA)
- J-pouch or transverse coloplasty pouch for reservoir function
4. Abdominoperineal Resection (APR)
- Required for tumors involving the sphincter complex or very low locally advanced tumors
- Results in permanent colostomy
- Also indicated in patients with poor preoperative bowel function/incontinence
5. Local Excision (TEM/TAMIS)
- Reserved for cT1N0 tumors without high-risk features
- High-risk features precluding local excision alone: deep T1 (>1 mm submucosa / Kikuchi SM3), poor differentiation, LVI, PNI, tumor budding, positive margins
- If high-risk features found on final pathology: formal TME recommended
6. Minimally Invasive TME
-
Laparoscopic, robotic, or transanal TME (taTME)
-
Improves short-term outcomes; should be performed by experienced surgeons
-
Oncologic non-inferiority vs. open surgery not fully established by RCTs for laparoscopic approach
-
Sabiston Textbook of Surgery, Bailey & Love's, Current Surgical Therapy 14e
Preoperative Preparation
- Mechanical bowel preparation (diet, purgatives, enemas)
- Perioperative IV antibiotics at induction (broad-spectrum)
- In USA: oral neomycin + metronidazole preoperatively in addition to IV antibiotics
- Stoma care nurse counseling and stoma siting preoperatively
Adjuvant Therapy
| Scenario | Recommendation |
|---|---|
| Received TNT with path stage II/III | No adjuvant chemotherapy needed |
| Stage II/III, did not receive full neoadjuvant chemo | Adjuvant FOLFOX x 8 cycles preferred |
| Stage II/III, no prior radiotherapy, high local recurrence risk | Adjuvant radiotherapy (selective) |
| cT3N0 | Oxaliplatin can be omitted |
Early initiation of adjuvant chemotherapy after resection is associated with improved outcomes.
Management of Synchronous Metastases (~20% at presentation)
- Liver is most common metastatic site (~50% stage IV have liver-only disease)
- Long-term survival achievable in >1/3 of patients selected for hepatic resection
- Lung metastases more common in rectal vs. colon cancer
"Watch and Wait" Strategy
For patients with cCR after neoadjuvant CRT:
- Clinical, endoscopic, and radiologic complete response
- Intensive surveillance with DRE, endoscopy, and MRI
- ~20% of CRT-treated patients eligible
- Surgical salvage if local regrowth occurs
PART B: CARCINOMA OF THE ANAL CANAL / ANAL MARGIN
Anatomy
- Anal canal: from anorectal ring to anal verge (4 cm)
- Anal margin: from anal verge extending 5 cm radially onto perianal skin
- Dentate line: divides squamous (below) from columnar (above) epithelium
Histological Types
- Squamous cell carcinoma (SCC) - most common anal canal cancer
- Adenocarcinoma (near anorectal junction)
- Melanoma (rare)
Staging (AJCC for Anal SCC)
| Stage | Primary Tumor | Lymph Nodes | Metastases |
|---|---|---|---|
| 1 | <2 cm (T1) | - | - |
| 2 | 2-5 cm (T2) or >5 cm (T3) | - | - |
| 3A | Any T | Perirectal (N1) or T4 + N0 | - |
| 3B | T4 + N1 or any T + N2/N3 | Bilateral or inguinal nodes | - |
| 4 | Any T | Any N | + |
Clinical Evaluation & Staging
- History: symptoms + risk factors (HIV, HPV, immunosuppression, anoreceptive intercourse)
- Physical exam: tumor size, location, relationship to dentate line and sphincters
- Anoscopy/proctosigmoidoscopy + biopsy
- Full colonoscopy (rule out synchronous CRC, up to 15% of cases)
- Gynecologic exam + cervical cancer screening in females
- HIV testing for all patients
- CT chest/abdomen/pelvis
- Pelvic MRI (optional, for primary tumor detail)
- Inguinal node biopsy if clinically suspicious
Treatment
Anal Margin SCC
- Small tumors: Wide local excision with 1-cm margins (if adequate margins without encroaching on canal/musculature)
- Larger tumors or high-risk features: CRT as first line
Anal Canal SCC - Standard: Nigro Protocol (CRT)
- Radiation: 45 Gy to the pelvis + 15-20 Gy boost
- Chemotherapy: 5-FU (infusional) + Mitomycin-C
- Cisplatin may substitute for Mitomycin-C without detriment to outcomes
- Results: 80% complete response rate, 72% colostomy-free rate
- Clinically/histologically positive inguinal nodes included in radiation fields
Response Assessment
- Assess at 12 weeks after completing CRT (DRE + anoscopy/proctoscopy)
- If complete response: enter surveillance
- If good but incomplete response: reassess at 6 more weeks
- At 11 weeks: 64% cCR; by 26 weeks: 85% cCR
- Patients failing to achieve cCR at 26 weeks: significantly inferior 5-year OS (48% vs 87%)
- If lesion persists/progresses: biopsy to confirm SCC, then salvage APR
Salvage APR
- For residual/recurrent anal SCC after CRT
- Soft tissue flaps often needed for wound closure in radiated field
Surveillance After CRT (NCCN guidelines)
-
DRE + inguinal node palpation every 3-6 months x 5 years
-
Anoscopy every 6-12 months x 3 years
-
CT CAP (or pelvic MRI) annually x 3 years (stage II/III)
-
Local recurrence without metastases: APR
-
Sabiston Textbook of Surgery, Current Surgical Therapy 14e
Summary
| Feature | Rectal Adenocarcinoma | Anal Canal SCC |
|---|---|---|
| Histology | Adenocarcinoma | Squamous cell carcinoma |
| Main treatment | TME surgery ± neoadjuvant CRT | Nigro Protocol (CRT) - organ preserving |
| Surgery type | AR, LAR, or APR | APR only for salvage |
| Staging | TNM (AJCC 8th), Dukes | TNM (AJCC) |
| Key imaging | MRI pelvis + CT CAP | CT CAP ± pelvic MRI |
| Colostomy | Avoided if sphincter preserved | Avoided unless salvage APR |
Recent evidence note: The 2024 ASCO Guideline on Locally Advanced Rectal Cancer (PMID 39116386, J Clin Oncol 2024) and a 2025 meta-analysis on neoadjuvant PD-1/PD-L1 inhibitors combined with CRT (PMID 40453663) may update some neoadjuvant protocols - immunotherapy combinations are an emerging area particularly for MMR-deficient rectal cancers.
This is a shared conversation. Sign in to Orris to start your own chat.