Mitral clips
Reading File
Finding Sources
Finding Sources
Searching PubMed
"MitraClip" AND "mitral regurgitation"
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive information to provide a thorough answer. Let me compile everything.
Mitral Clips (Transcatheter Edge-to-Edge Repair / TEER)
What is a Mitral Clip?
The MitraClip (Abbott Vascular) is a percutaneous device that mimics the Alfieri edge-to-edge surgical repair - it clips the free edges of the anterior and posterior mitral leaflets together to create a double-orifice mitral valve, reducing mitral regurgitation (MR) without open-heart surgery.
- Delivered via a transfemoral transseptal approach under general anesthesia with TEE guidance
- The clip grasps both leaflets on the ventricular side to create leaflet apposition
- The effect on MR is evaluated in real time by echocardiography (unlike open surgery, which is assessed after cardiopulmonary bypass is discontinued)
- Multiple clips can be placed if the initial result is suboptimal
- Classic clip position: between the A2 and P2 scallops, creating a double orifice
- Barash Clinical Anesthesia 9e, p. 2687; Braunwald's Heart Disease, p. 809
3D Echo View After MitraClip Placement
Here is an intraoperative 3D TEE "surgeon's view" showing the MitraClip in position between the A2/P2 scallops, with the double orifice visible on either side:
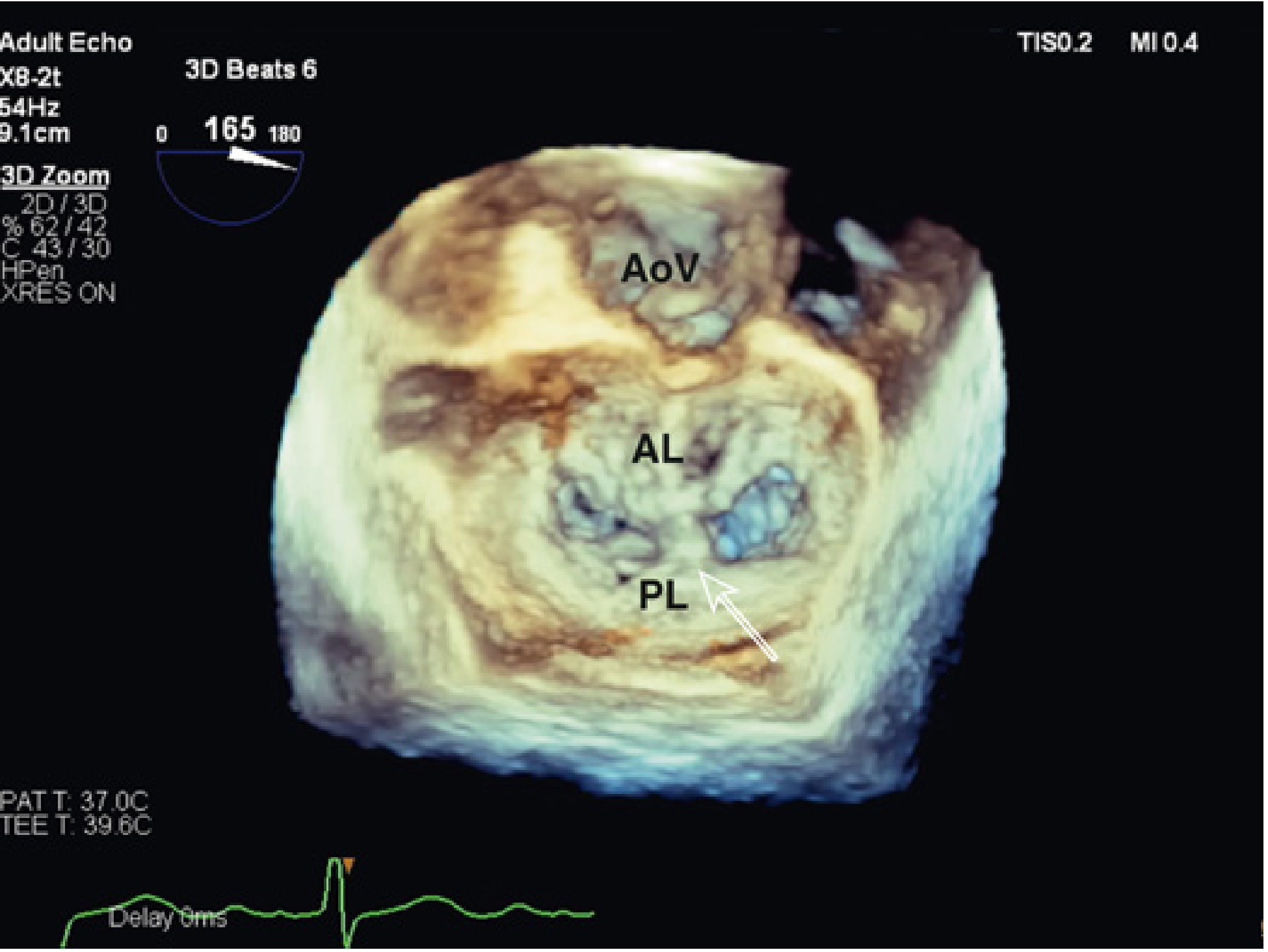
3D en face (surgeon's view) TEE showing MitraClip between anterior leaflet (AL) and posterior leaflet (PL), with the aortic valve (AoV) visible superiorly. - Miller's Anesthesia 10e, Fig. 33.30
Indications
| Type of MR | Indication |
|---|---|
| Primary (degenerative) MR | High surgical risk patients with symptomatic moderately-severe to severe MR (e.g., flail leaflet, prolapse) |
| Secondary (functional) MR | Heart failure patients with secondary MR who remain symptomatic despite optimal guideline-directed medical therapy (GDMT) |
Contraindications/unfavorable features (per Fuster & Hurst):
- LVEF <30%
- Extreme NT-proBNP >10,000 pg/mL
- Significant RV dysfunction (TAPSE <15 mm)
- Severe pulmonary hypertension or severe TR
- Major comorbidities (significant renal dysfunction)
- Excessive LV dilatation (LVESD >70 mm per COAPT)
- Fuster & Hurst's The Heart 15e, p. 969
Key Clinical Trials
Primary MR - EVEREST II
- 184 MitraClip vs. 95 surgical repair/replacement
- 30-day major adverse events: 9.6% vs. 57% (surgery) - largely driven by transfusion requirement
- Freedom from death/MV surgery/MR >2+ at 12 months: 55% (clip) vs. 73% (surgery) - surgery superior for durability
- BUT: MitraClip showed greater benefit than surgery in higher-risk patients
- Durable results at follow-up in patients with acute procedural success
Secondary MR - COAPT Trial (US/Canada, n=614)
- Symptomatic HF + moderate-severe secondary MR; all on optimal GDMT
- LVEF 20-50%, LVESD ≤69 mm, MR grade 3-4+
- Primary endpoint (HF hospitalization at 24 months): 35.8 vs 67.9 per 100 patient-years (NNT = 3.1) - P<0.001
- All-cause mortality at 24 months: 29.1% vs 46.1% (NNT = 5.9) - P<0.001
- Benefits even more pronounced at 3 years
Secondary MR - MITRA-FR Trial (France, n=304)
- No significant difference in all-cause death + HF hospitalization at 12 months (54.6% vs 51.3%, P=NS)
- No change at 24-month follow-up either
Why did COAPT and MITRA-FR conflict?
| Feature | MITRA-FR | COAPT |
|---|---|---|
| MR severity criteria | ERO >20 mm² | MR grade 3-4+ (AHA) |
| LV size exclusion | None | LVESD >70 mm |
| RV dysfunction exclusion | None | Moderate/severe excluded |
| Follow-up endpoint | 1 year | 2 years (recurrent events) |
| GDMT intensity | Less strict | More intensive |
Post-hoc analysis: COAPT enrolled patients with proportionally more severe MR relative to LV size (more "valve-driven" rather than "ventricle-driven" disease), hence more potential for benefit. Patients most likely to benefit: ERO ≥0.30 cm² + no excessive LV dilatation + after intensive GDMT has failed.
- Fuster & Hurst's The Heart 15e, p. 972; Braunwald's Heart Disease, p. 810
Procedure - Anesthetic Considerations
- General anesthesia with invasive monitoring is standard
- TEE is mandatory - guides transseptal puncture, clip positioning, and real-time MR assessment
- Transseptal puncture target: superior and posterior in the fossa ovalis (to allow adequate working height above the mitral valve)
- Mortality is lower with MitraClip vs. surgery using standard surgical risk prediction models
- Barash Clinical Anesthesia 9e, p. 2687; Miller's Anesthesia 10e, p. 5057
Next-Generation Devices
| Device | Key Feature |
|---|---|
| MitraClip NTR/XTR (Abbott) | Newer iterations with better grasping; EXPAND registry showed improved outcomes with experience |
| PASCAL (Edwards Lifesciences) | Wider paddles + central spacer to fill regurgitant orifice; independent leaflet capture; 98% success in early series |
| DRAGONFLY (Hangzhou Valgen, China) | Early clinical development |
Tricuspid Extension
Both MitraClip and PASCAL are also being used in the tricuspid position (anterior + septal leaflet clipping):
- Trivalve Registry (n=249): 96% technical success; TR ≥3+ reduced from 97% to 23% at discharge; 1-year mortality 20.3%
- TRILUMINATE trial: Prospective multicenter study ongoing
- Braunwald's Heart Disease, p. 811
Recent Evidence (2023-2026)
- TEER for MR in cardiogenic shock (2025 meta-analysis) - PMID 40055145: Systematic review confirming procedural feasibility in this very high-risk setting
- MitraClip vs. PASCAL meta-analysis (2025) - PMID 39754135: Both devices show comparable clinical outcomes; PASCAL may achieve better MR reduction
- MitraClip vs. surgery for secondary MR (2025) - PMID 40851316: Updated meta-analysis ongoing
Summary Points
- MitraClip = percutaneous edge-to-edge repair; mimics Alfieri technique; creates double-orifice MV
- Main indications: high-surgical-risk primary MR; secondary MR with HF after adequate GDMT
- EVEREST II: less durable than surgery overall, but better for high-risk patients
- COAPT: landmark benefit for secondary MR (NNT 3.1 for HF hospitalization, NNT 5.9 for mortality)
- MITRA-FR: negative trial - key lesson is patient selection (proportionate vs. disproportionate MR)
- TEE guidance is essential throughout the procedure
- Expanding to tricuspid valve repair and newer devices (PASCAL)
This is a shared conversation. Sign in to Orris to start your own chat.