Help me understand small incision cataract surgery in short and effective way for a 10 marks answer in exam
Small Incision Cataract Surgery (SICS) / Manual SICS (MSICS)
Definition
Historical Context
| Technique | Incision Size | Notes |
|---|---|---|
| ICCE (older) | Very large | Entire lens + capsule removed with cryoprobe |
| ECCE (conventional) | 8-10 mm limbal | Requires suturing; induces corneal astigmatism |
| MSICS | 5-7 mm scleral tunnel | Self-sealing; no sutures needed |
| Phacoemulsification | 2-3 mm | Expensive equipment; standard in high-income countries |
Steps of MSICS (Surgical Technique)
1. Incision - Scleral Tunnel
- A self-sealing sclero-corneal tunnel is created, approximately 5-7 mm wide
- The tunnel is constructed so the internal opening is wider than the external (valve mechanism) - this prevents leakage without sutures
- The incision is placed about 2 mm posterior to the limbus
2. Anterior Capsulotomy (Capsulorhexis)
- Trypan blue dye (0.1%) is injected to stain the anterior capsule, making it visible (especially useful in mature/hypermature cataracts)
- A continuous curvilinear capsulorhexis (CCC) of ~5-6 mm is created
- Alternatively, a can-opener capsulotomy may be used
3. Hydrodissection
- Balanced salt solution (BSS) is injected under the anterior capsule to separate the cortex from the capsule and free the nucleus
- This allows smooth nucleus prolapse and rotation
4. Nucleus Expression
- The nucleus is manually prolapsed into the anterior chamber using a lens dialer or Sinskey hook
- It is then delivered out through the scleral tunnel in one piece using a wire vectis or irrigating vectis
- This is the defining step - the nucleus comes out intact without ultrasound energy
5. Cortical Aspiration
- Residual cortical material is aspirated using a Simcoe double-lumen cannula (irrigation + aspiration simultaneously)
- The posterior capsule is carefully preserved
6. IOL Implantation
- A posterior chamber IOL (PCIOL) is implanted into the capsular bag
- A rigid PMMA IOL can be used (unlike phaco, where a foldable IOL is needed)
- OVD (viscoelastic) is used to maintain the anterior chamber depth and protect the endothelium
7. Wound Closure
- The self-sealing scleral tunnel usually requires no sutures
- The wound is checked for watertight closure (Seidel test)
Advantages of MSICS
| Feature | Benefit |
|---|---|
| No phaco machine needed | Cost-effective; suitable for developing countries |
| Self-sealing wound | No suture-induced astigmatism |
| Faster surgery | High-volume camps possible |
| Dense cataracts handled well | No ultrasound energy - nucleus removed whole |
| Visual outcomes | Comparable to phacoemulsification |
| Rigid IOL usable | Cheaper than foldable IOLs |
Disadvantages / Limitations
- Larger incision than phacoemulsification (5-7 mm vs 2-3 mm) - slightly more trauma
- Higher risk of induced astigmatism compared to phaco (though less than conventional ECCE)
- Requires more surgical skill than ECCE for nucleus delivery
- Not ideal for very soft or very hard nuclei equally well (best for grade 2-4 nuclear sclerosis)
Comparison: MSICS vs Phacoemulsification
| Parameter | MSICS | Phacoemulsification |
|---|---|---|
| Incision | 5-7 mm scleral tunnel | 2-3 mm corneal |
| Technology | Manual instruments | Ultrasound machine |
| Cost | Low | High |
| Dense cataracts | Excellent | Risk of complications |
| Visual recovery | Slightly slower | Faster |
| Astigmatism | Minimal | Least |
| IOL type | Rigid PMMA or foldable | Foldable only |
Key Points to Remember for Exam
- MSICS = variant of ECCE, not phaco
- The scleral tunnel is self-sealing - key architectural feature
- Trypan blue stains the capsule for safe capsulorhexis
- Nucleus is removed in one piece - no fragmentation
- Simcoe cannula for cortex removal
- Visual rehabilitation is comparable to phacoemulsification
- Preferred technique for high-volume, low-resource settings (e.g., eye camps in India/Africa)
I need it in 12 steps as per ak khurana
AK Khurana ophthalmology SICS 12 steps small incision cataract surgery
https://dokumen.pub/disorders-of-lens-and-cataract-surgery-f…
https://pmc.ncbi.nlm.nih.gov/articles/PMC12400266
SICS - 12 Steps as per A.K. Khurana
Definition
The 12 Steps
Step 1 - Bridle Suture
- A superior rectus bridle suture (4-0 black silk) is placed to fix and depress the globe
- This brings the superior limbal area into the operative field
- Provides counter-traction during tunnel construction
Step 2 - Conjunctival Peritomy (Flap)
- A fornix-based conjunctival flap is raised from 10 o'clock to 2 o'clock position
- Bare sclera is exposed superiorly
- Bleeding is controlled with bipolar diathermy cautery
Step 3 - Scleral Groove (Partial Thickness Incision)
- A linear groove is made in the sclera, 2 mm posterior to the limbus, ~6-7 mm wide
- Depth: approximately 1/2 to 2/3 scleral thickness
- This marks the external opening of the tunnel
- A crescent knife is used for this step
Step 4 - Sclerocorneal Tunnel Dissection
- Using the crescent knife, a lamellar tunnel is dissected forward into clear cornea (1-1.5 mm beyond the limbus)
- The tunnel is triplanar - scleral plane → limbal plane → corneal plane
- Internal opening is wider than external opening (valvular/trapezoid shape) = self-sealing
- The inner corneal lip (shelf) creates the valve mechanism
Step 5 - Internal Corneal Entry (Keratome Entry)
- A keratome (3.2 mm) or bent needle enters the anterior chamber through the inner tunnel lip
- The anterior chamber (AC) is entered at the level of the posterior limbus
- A side-port paracentesis (1 mm) is also made at 2-3 o'clock for a second instrument
Step 6 - Anterior Capsulotomy
- Trypan blue 0.1% is injected to stain the anterior capsule (especially in mature cataracts)
- OVD (viscoelastic) is injected to maintain AC depth
- A Continuous Curvilinear Capsulorhexis (CCC) of 5-6 mm is made using a cystotome or Utrata forceps
- Alternatively, a can-opener capsulotomy using a 26G needle is performed
Step 7 - Hydrodissection and Hydrodelineation
- Hydrodissection: BSS injected under the anterior capsular rim to separate cortex from capsule - creates a fluid wave behind the nucleus
- Hydrodelineation: BSS injected into the nucleus to separate the epinucleus from the endonucleus (creates a "golden ring")
- This loosens and mobilizes the nucleus, allowing free rotation
Step 8 - Nuclear Prolapse into Anterior Chamber
- The nucleus is rotated and prolapsed into the anterior chamber using a Sinskey hook or nucleus rotator
- Gentle pressure at the inferior limbus with a second instrument helps prolapse the nucleus through the capsulorhexis opening
- OVD is placed above and below the nucleus to protect the corneal endothelium
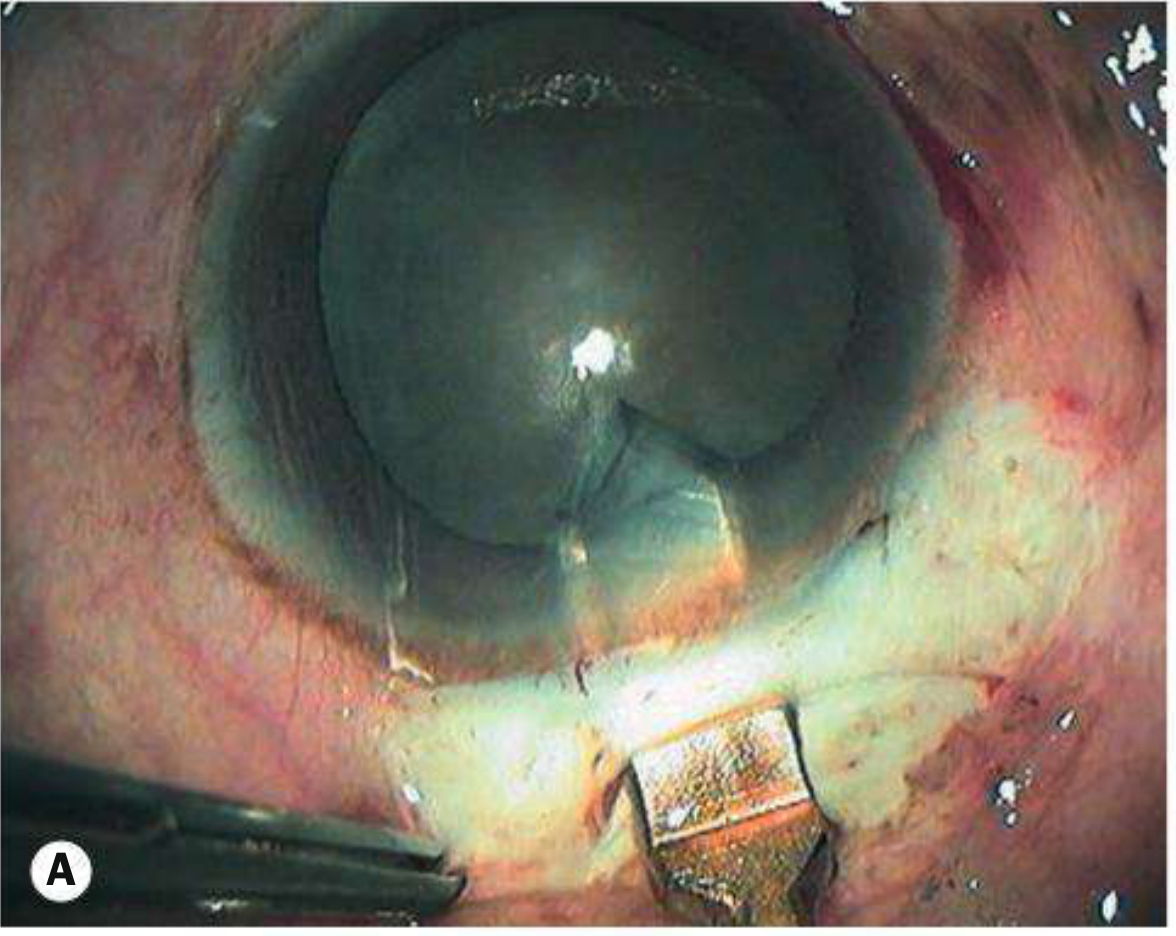
Step 9 - Nuclear Delivery (Expression)
- The nucleus is delivered out through the sclerocorneal tunnel in one piece
- Two main methods:
- Vectis method: Irrigating vectis is passed under the nucleus and lifts it out
- Viscoexpression: OVD injected behind the nucleus to push it out (Blumenthal technique)
- Phaco-sandwich / wire loop: for harder nuclei
- No ultrasound energy is used
Step 10 - Cortical Aspiration
- Residual cortical matter is aspirated using a Simcoe double-lumen cannula (irrigation + aspiration in one instrument)
- 360° cortex is removed systematically
- The posterior capsule is polished to remove any residual lens epithelial cells (reduces PCO)
- AC is maintained throughout with irrigation
Step 11 - IOL Implantation
- AC is refilled with OVD to maintain depth and protect the endothelium
- A rigid PMMA posterior chamber IOL (PCIOL) (5.5-6 mm optic) is implanted into the capsular bag
- The leading haptic is placed first, then the optic is dialed in, followed by the trailing haptic
- If capsulorhexis is intact - bag fixation; if not - sulcus fixation
- OVD is thoroughly removed after IOL placement to prevent IOP spike
Step 12 - Wound Closure
- The sclerocorneal tunnel is self-sealing - no sutures required (the valvular architecture closes on hydration)
- Stromal hydration of side port with BSS to ensure watertight closure
- Conjunctival flap is reposited and secured with bipolar cautery or absorbable suture (8-0 Vicryl)
- AC is checked for formed depth and no wound leak (Seidel test)
- Subconjunctival antibiotic + steroid injection given at the end
Summary Table
| Step | Action | Key Instrument |
|---|---|---|
| 1 | Bridle suture | 4-0 black silk |
| 2 | Conjunctival peritomy | Scissors + cautery |
| 3 | Scleral groove | Crescent knife |
| 4 | Tunnel dissection | Crescent knife |
| 5 | Keratome entry | Keratome/bent 26G |
| 6 | Anterior capsulotomy (CCC) | Cystotome/Utrata + trypan blue |
| 7 | Hydrodissection | Cannula + BSS |
| 8 | Nuclear prolapse into AC | Sinskey hook |
| 9 | Nuclear delivery | Vectis / viscoexpression |
| 10 | Cortical aspiration | Simcoe cannula |
| 11 | IOL implantation | Lens folder/inserter |
| 12 | Wound closure | Cautery / self-sealing |
Key Points for Exam
- The triplanar tunnel is the basis of self-sealing (no sutures needed)
- Trypan blue - stains capsule in mature cataract
- Simcoe cannula - used for cortex aspiration (irrigation + aspiration combined)
- Vectis - instrument for nucleus delivery
- Incision size: 5-7 mm external, wider internally
- Visual outcomes comparable to phacoemulsification - but no expensive machine needed
- Best suited for dense/mature cataracts and high-volume settings
Can you create a poster of this with diagrams for easy and quick revision fir exam
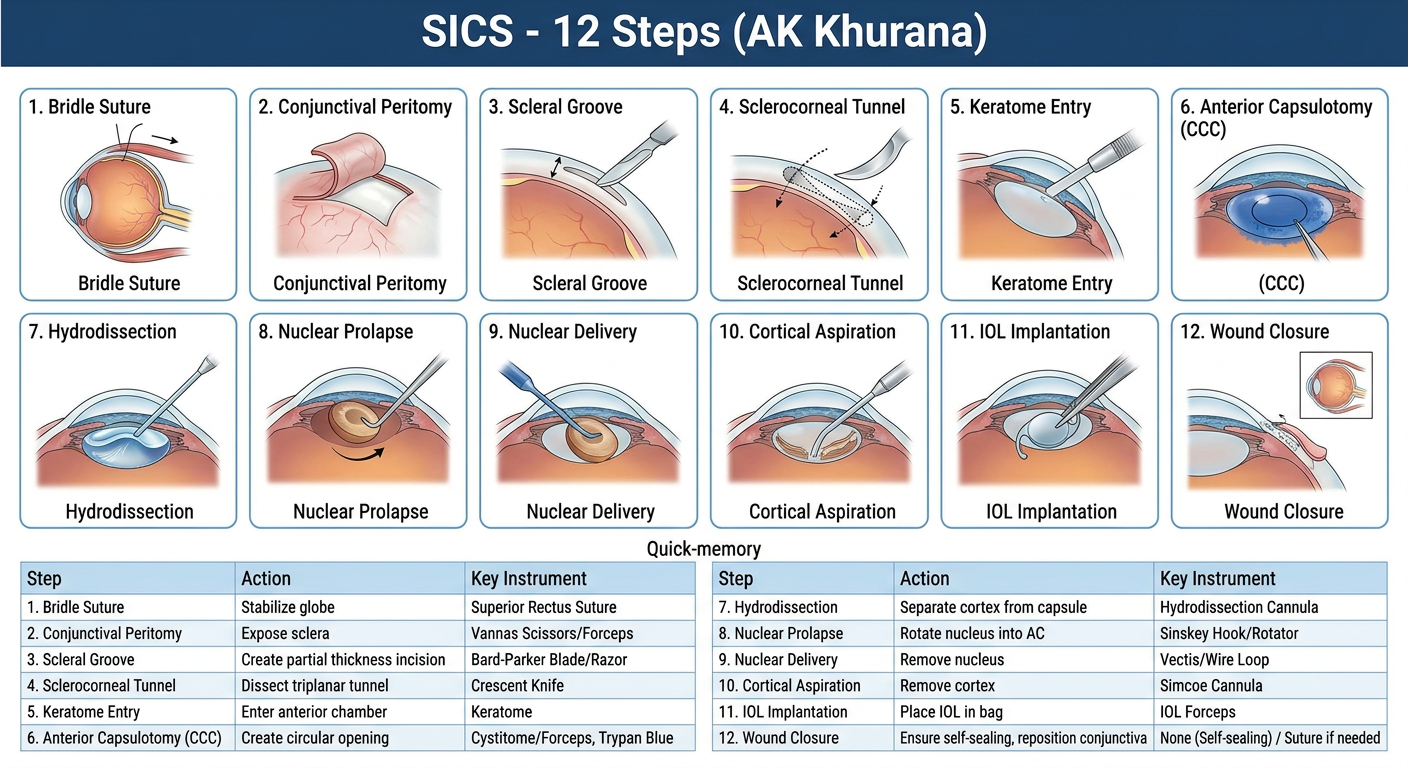
A detailed medical revision poster titled "SICS - 12 Steps (AK Khurana)" for ophthalmology exam preparation. The poster shows all 12 surgical steps of Small Incision Cataract Surgery in a clean grid layout with numbered boxes. Each step has a small anatomical diagram/illustration and a brief label: 1. Bridle Suture - diagram of superior rectus suture holding globe 2. Conjunctival Peritomy - fornix-based flap exposing bare sclera 3. Scleral Groove - partial thickness groove 2mm from limbus 4. Sclerocorneal Tunnel - triplanar dissection with crescent knife 5. Keratome Entry - keratome entering anterior chamber 6. Anterior Capsulotomy (CCC) - circular capsulorhexis with trypan blue staining 7. Hydrodissection - fluid wave separating cortex from capsule 8. Nuclear Prolapse - nucleus being rotated into anterior chamber 9. Nuclear Delivery - vectis delivering nucleus through tunnel 10. Cortical Aspiration - Simcoe cannula removing cortex 11. IOL Implantation - PMMA lens being placed in capsular bag 12. Wound Closure - self-sealing tunnel, conjunctival repositioning At the bottom include a quick-memory table with columns: Step, Action, Key Instrument. Color scheme: dark blue header, white background, each step in a light blue bordered box with diagrams. Clean medical textbook illustration style.
- Steps 1-5 = Getting IN (access to the eye)
- Steps 6-8 = Preparing the lens (capsule + nucleus)
- Steps 9-10 = Removing the lens (nucleus + cortex)
- Steps 11-12 = Finishing (IOL + closure)