Colorectal Cancer types, etiology, clinical features, investigation & management of it
Reading File
Finding Sources
Finding Sources
Searching PubMed
"colorectal cancer"[MeSH Terms] AND "management"[MeSH Terms]
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive content. Let me compile the complete, detailed answer:
Colorectal Cancer (CRC): A Comprehensive Overview
Epidemiology
Colorectal cancer is the 3rd most common cancer worldwide and a leading cause of cancer-related death. In Europe, North America, and Australasia, it is the greatest cause of cancer mortality in non-smokers. Incidence rises sharply with advancing age, and approximately 10% of cases have a significant hereditary component.
- Pye's Surgical Handicraft, 22nd Ed.
- Sabiston Textbook of Surgery, p. 2121
Types of Colorectal Cancer
By Histology
| Type | Details |
|---|---|
| Adenocarcinoma | ~95% of all CRC; arises from glandular epithelium |
| Mucinous adenocarcinoma | Produces abundant mucin; worse prognosis |
| Signet ring cell carcinoma | Rare; very poor prognosis (5-year survival 9-36%) |
| Squamous cell carcinoma | Rare in colon; more common in anal canal |
| Neuroendocrine tumors | Rare; includes carcinoids |
| Lymphoma/GIST | Very rare secondary types |
By Molecular/Genetic Pathway
Three distinct but overlapping pathways lead to CRC (see diagram below):
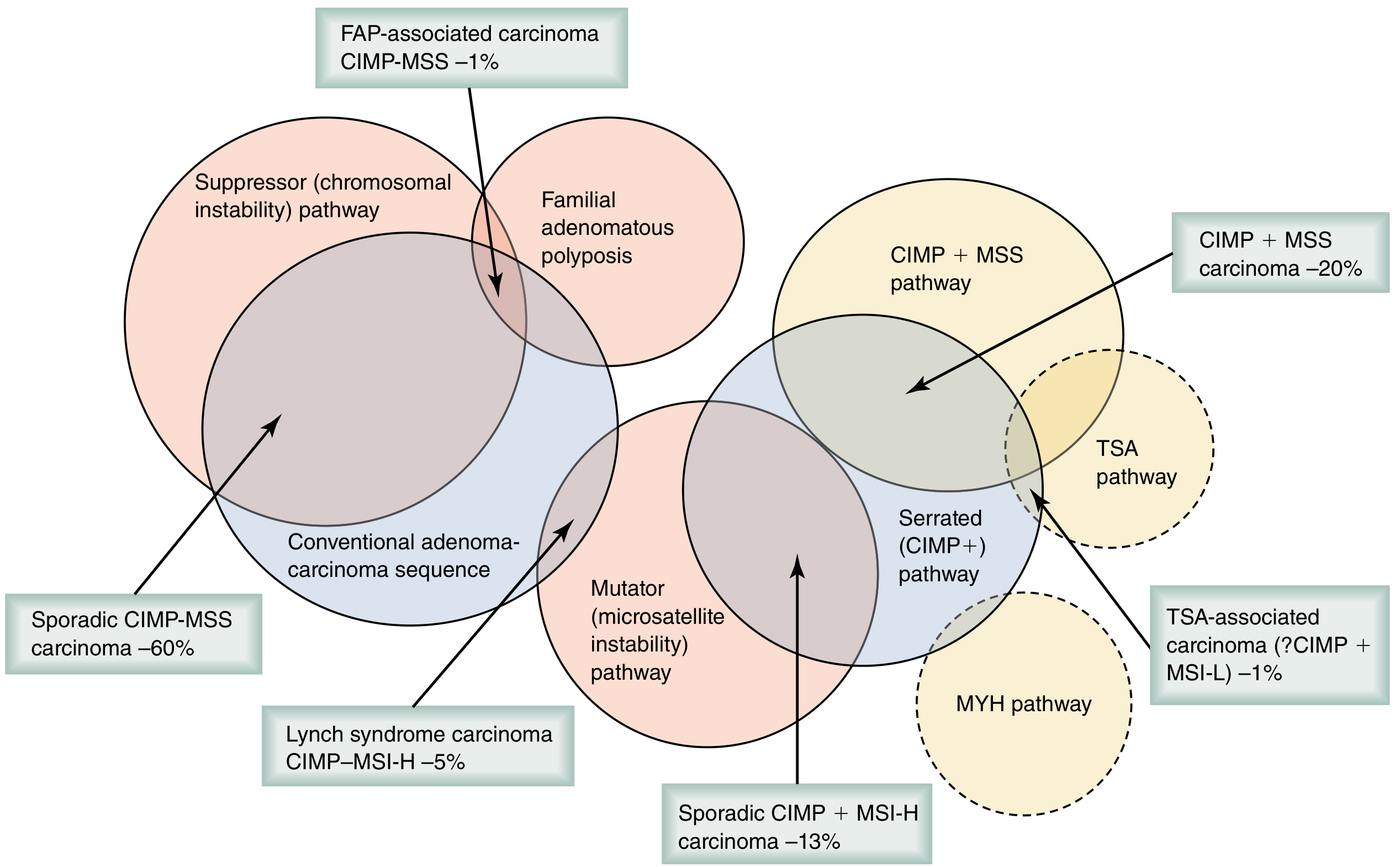
-
Chromosomal Instability (CIN) Pathway - Most common (65-70%). Initiated by APC gene mutation → Wnt/β-catenin activation → tubular adenoma → KRAS mutation → TP53/SMAD4 changes → invasive cancer. The classic adenoma-to-carcinoma sequence. Results in sporadic CIMP-MSS carcinoma (~60%).
-
Serrated/Methylator Pathway (CIMP+) - Initiated by BRAF mutation → CpG island methylator phenotype (CIMP) → silencing of tumor-suppressor genes. Accounts for ~15-20% of CRCs. Tumors tend to be right-sided, in older/female patients. Sporadic CIMP+MSI-H accounts for ~13%, and CIMP+MSS ~20%.
-
Microsatellite Instability (MSI) Pathway - Loss of mismatch repair (MMR) function (MLH1, MSH2, MSH6, PMS2 genes). Three etiologies: Lynch syndrome germline variant, MLH1 hypermethylation, or somatic MMR mutation. Lynch syndrome carcinoma (CIMP-MSI-H) accounts for ~5% of CRC.
- Sabiston Textbook of Surgery, pp. 2121-2122
By Location
- 50% in sigmoid colon and rectum
- Right colon (cecum/ascending): often occult, presents with iron-deficiency anemia
- Left colon/sigmoid: more likely to cause obstruction, change in bowel habits
- Rectal: rectal bleeding, tenesmus
Etiology & Risk Factors
Non-Modifiable Risk Factors
- Age >50 (risk increases sharply)
- Personal history of adenomatous polyps or CRC
- Family history of CRC or adenomas
- Hereditary syndromes (see below)
- Inflammatory bowel disease (UC > Crohn's; risk rises after 8-10 years of disease)
- Male sex (slightly higher risk)
Modifiable/Environmental Risk Factors
- Diet high in red/processed meat; low in fiber
- Obesity and physical inactivity
- Alcohol consumption
- Smoking
- Diabetes mellitus and insulin resistance
Hereditary Syndromes
Polyposis Syndromes
| Syndrome | Gene | Key Features |
|---|---|---|
| FAP (Familial Adenomatous Polyposis) | APC (autosomal dominant) | Hundreds-thousands of polyps; near 100% CRC risk without colectomy; congenital hypertrophy of retinal pigment epithelium (CHRPE) aids early ID of family members |
| MAP (MYH-associated polyposis) | MUTYH (autosomal recessive) | 10-100s of polyps |
| Serrated polyposis syndrome | Unknown | >20 serrated polyps; 15-30% lifetime CRC risk |
| Juvenile polyposis, Peutz-Jeghers, PTEN hamartoma | SMAD4/BMPR1A; STK11; PTEN | Variable CRC risk |
Nonpolyposis Syndromes
-
Lynch Syndrome (HNPCC): Autosomal dominant; MMR gene pathogenic variant (MLH1, MSH2, MSH6, PMS2, EPCAM). Incidence: 1/279 in general population; ~3% of all CRCs. Cumulative CRC risk by age 80: 46-61% (MLH1), 33-52% (MSH2), 10-44% (MSH6), 8.7-20% (PMS2). Also at risk: endometrial, ovarian, gastric, urological, pancreatic, small bowel cancers. Amsterdam II criteria used for clinical diagnosis. Annual colonoscopy from age 20-25.
-
Sabiston Textbook of Surgery, pp. 2122-2124
Clinical Features
Right-Sided Colon Cancer
- Iron-deficiency anemia (occult bleeding from cecal/ascending lesions)
- Fatigue, pallor
- Palpable right iliac fossa mass
- Vague abdominal discomfort
- Late obstruction (large lumen)
Left-Sided Colon / Sigmoid Cancer
- Change in bowel habit (most common symptom overall) - alternating constipation/diarrhea
- Bright red rectal bleeding or blood mixed with stool
- "Pencil-thin" stools
- Colicky abdominal pain
- Acute intestinal obstruction (narrower lumen)
Rectal Cancer
- Rectal bleeding (most common symptom)
- Tenesmus (feeling of incomplete evacuation)
- Mucous per rectum
- Pelvic/perineal pain (advanced)
- Palpable mass on digital rectal examination
Advanced/Systemic Features
-
Weight loss
-
Anorexia
-
Hepatomegaly (liver metastases)
-
Jaundice
-
Malignant ascites
-
Features of distant metastases (lung, bone, brain)
-
Acute presentations: intestinal obstruction (~8-29% of cases), perforation, fistula
-
Pye's Surgical Handicraft, 22nd Ed., p. 275
Investigations
Blood Tests
- FBC: Microcytic hypochromic anemia (iron deficiency from chronic blood loss)
- LFTs: May be deranged with liver metastases
- CEA (Carcinoembryonic antigen): Tumor marker; preoperative level >5 ng/mL predicts worse disease-free survival (DFS). Used primarily for post-treatment surveillance - not diagnostic
- CA 19-9: May be elevated
- LDH, ALP: Non-specific markers of metastatic disease
Stool Tests
- Fecal Occult Blood Test (FOBT) / Fecal Immunochemical Test (FIT): Screening tools
- Multi-targeted stool DNA test: Every 1-3 years as screening option
Endoscopy
- Colonoscopy: Gold standard - allows visualization, biopsy, and polypectomy of the entire colon. Preferred screening modality
- Flexible sigmoidoscopy: Visualizes distal colon only; combined with FOBT for screening
- CT colonography (virtual colonoscopy): Every 5 years as screening option; non-invasive
Imaging
- CT chest/abdomen/pelvis (staging): Primary modality for staging; detects liver, lung, lymph node metastases
- MRI pelvis: Critical for rectal cancer - assesses relationship to mesorectal fascia, circumferential resection margin (CRM), sphincter involvement, and depth of invasion (T staging)
- Endorectal ultrasound (ERUS): Accurate T and N staging for rectal cancer
- PET-CT: For equivocal metastatic lesions, recurrence assessment, or evaluating response to treatment
Histopathology & Molecular Testing
-
Biopsy: Confirms diagnosis, histological grade
-
MSI/MMR testing: All newly diagnosed CRC should be tested for Lynch syndrome screening
-
KRAS/NRAS/BRAF mutation testing: Required before initiating anti-EGFR therapy (cetuximab, panitumumab)
-
HER2 amplification, NTRK fusions: For targeted therapy eligibility in metastatic CRC
-
Sabiston Textbook of Surgery, pp. 2128-2135
-
Goldman-Cecil Medicine, p. 3962
Staging
TNM Staging (AJCC - 8th Edition)
| Stage | Description | 5-year Survival |
|---|---|---|
| I | T1-2, N0, M0 (mucosa/submucosa/muscularis) | ~90% |
| IIA | T3, N0, M0 (through muscularis propria) | ~70-80% |
| IIB/C | T4a/b, N0, M0 (peritoneum/adjacent organs) | ~55-65% |
| IIIA/B/C | Any T, N1-2, M0 (regional lymph nodes) | ~40-70% |
| IV | Any T, Any N, M1 (distant metastases) | <15% |
Dukes' Classification (Historical, Still Referenced)
| Stage | Description | 5-year Survival |
|---|---|---|
| A | Tumor confined to mucosa | 95% |
| B | Tumor invading muscle | 68% |
| C | Lymph node metastases | 34% |
| D | Distant metastases | <10% |
Poor Prognostic Factors
-
High CEA (>5 ng/mL) pre- and post-op
-
Lymphovascular invasion (LVI)
-
Perineural invasion (PNI)
-
High tumor budding
-
Mucinous histology / signet ring cells
-
BRAF and KRAS mutations (worse prognosis)
-
MSI-H predicts better survival (~15% better than MSS)
-
Sabiston Textbook of Surgery, pp. 2133-2135
-
Pye's Surgical Handicraft, Table 18.3
Management
Screening (Asymptomatic Average-Risk Adults ≥45 years)
- Annual high-sensitivity FOBT or FIT
- Multi-targeted stool DNA test every 1-3 years
- CT colonography every 5 years
- Flexible sigmoidoscopy every 5 years (or every 10 years + annual FOBT)
- Colonoscopy every 10 years (preferred - combines detection and treatment)
USPSTF recommends routine screening ages 45-75; selective 75-85.
Surgical Management
Colon Cancer
- Right hemicolectomy: Cecal, ascending, hepatic flexure cancers
- Transverse colectomy: Transverse colon tumors
- Left hemicolectomy: Descending colon tumors
- Sigmoid colectomy: Sigmoid tumors
- High anterior resection: Upper rectum/sigmoid junction
Principles include: oncologic margins, en bloc removal of draining lymphatics, high vascular ligation. Laparoscopic approach is standard when feasible.
Obstructing colon cancer (8-29% of cases):
- Right-sided: segmental resection ± primary anastomosis
- Left-sided: options include Hartmann's procedure (resection + end colostomy) or primary anastomosis in stable patients. Endoscopic stenting as bridge to elective surgery is an option - reduces wound infection, increases laparoscopic completion, higher rates of primary anastomosis.
Rectal Cancer
Key principle: Total Mesorectal Excision (TME) - removal of rectum en bloc with its mesorectum, blood vessels, and lymphatics, just outside the fascia propria ("holy plane" - Heald). TME reduced local recurrence from 25% to 6% (Norwegian cohort study of 3319 patients).
Surgical options based on tumor location:
- Low anterior resection (LAR): For upper and mid-rectal tumors with adequate distal margin; anastomosis with/without defunctioning stoma
- Abdominoperineal resection (APR): For very low rectal tumors where sphincter preservation is not possible; results in permanent colostomy
- Transanal endoscopic microsurgery (TEM)/Transanal minimally invasive surgery (TAMIS): For selected early T1-T2 rectal tumors
Neoadjuvant Therapy (Rectal Cancer)
- Neoadjuvant chemoradiotherapy (CRT) with 5-fluorouracil (5-FU) or capecitabine + radiation: Standard for locally advanced rectal cancer (T3/T4 or N+). Downsizes tumor, increases R0 resection rates, reduces local recurrence.
- Short-course radiotherapy (SCRT): 25 Gy in 5 fractions, followed by surgery within 1 week.
- Total Neoadjuvant Therapy (TNT): Full chemotherapy + radiation delivered before surgery (increasingly used).
Adjuvant Chemotherapy
Per NCCN guidelines:
- Stage III (lymph node positive): FOLFOX (oxaliplatin + 5-FU + leucovorin) or CAPOX (capecitabine + oxaliplatin) for 6 months - standard of care
- Stage II high-risk (T4, LVI, PNI, <12 nodes examined, obstruction/perforation, poor differentiation): adjuvant chemotherapy considered
- Stage II standard-risk: Generally surveillance alone; MSI-H tumors have less benefit from 5-FU monotherapy
- Stage IV: Systemic chemotherapy is the primary modality (FOLFOX, FOLFIRI ± bevacizumab/cetuximab/panitumumab based on RAS/BRAF status)
Targeted & Biologic Therapy (Metastatic CRC)
| Drug | Target | Indication |
|---|---|---|
| Bevacizumab | VEGF | All mCRC (regardless of RAS status) |
| Cetuximab / Panitumumab | EGFR | RAS wild-type tumors only |
| Pembrolizumab | PD-1 | MSI-H/dMMR mCRC (1st line) |
| Encorafenib + cetuximab | BRAF V600E + EGFR | BRAF V600E mutant mCRC |
| Larotrectinib / Entrectinib | NTRK | NTRK fusion-positive |
| Trastuzumab-based | HER2 | HER2-amplified mCRC |
Management of Liver Metastases
- ~15-25% of patients have synchronous liver metastases
- Surgical resection is the only potentially curative option; 5-year survival ~40% after R0 resection
- Neoadjuvant chemotherapy to downsize before surgery ("conversion chemotherapy")
- Ablation (radiofrequency or microwave) for non-resectable small lesions
- Hepatic arterial infusion pump for liver-predominant disease
Surveillance After Curative Resection
-
CEA every 3-6 months for 2 years, then every 6 months for 3 years
-
CT chest/abdomen/pelvis annually for 5 years
-
Colonoscopy at 1 year post-resection, then every 3-5 years
-
Regular history and physical examination
-
Sabiston Textbook of Surgery, pp. 2133-2150
Key Summary Points
| Aspect | Key Facts |
|---|---|
| Most common type | Adenocarcinoma (95%) |
| Most common pathway | CIN (adenoma-carcinoma sequence, 65-70%) |
| Most common symptom | Change in bowel habit |
| Gold standard investigation | Colonoscopy with biopsy |
| Staging system | AJCC TNM (8th ed.) |
| Curative treatment | Surgical resection (hemicolectomy/LAR/APR + TME) |
| Key surgical principle for rectal Ca | Total Mesorectal Excision (TME) |
| Adjuvant therapy (Stage III) | FOLFOX or CAPOX x 6 months |
| Tumor marker for follow-up | CEA |
| Hereditary syndrome screening | MSI/MMR testing on all new CRC |
Sources: Sabiston Textbook of Surgery (Biological Basis of Modern Surgical Practice); Pye's Surgical Handicraft, 22nd Ed.; Goldman-Cecil Medicine; Sleisenger & Fordtran's Gastrointestinal and Liver Disease
This is a shared conversation. Sign in to Orris to start your own chat.