Septic arthritis in CKD patient
Reading File
Finding Sources
Finding Sources
Searching PubMed
"septic arthritis" AND "chronic kidney disease"
Reading File
Reading File
Reading File
Reading Article
PMID: 40800124
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
I now have comprehensive content from multiple authoritative sources. Let me compile the full, detailed answer.
Septic Arthritis in CKD Patients
Why CKD Changes Everything
CKD is a recognised independent risk factor and prognostic determinant for septic arthritis. The mechanisms are multiple:
- Uremia-induced immune dysfunction - uremia impairs polymorphonuclear (PMN) cell chemotaxis, phagocytosis, and oxidative burst, producing a functional immunocompromised state even without immunosuppressive drugs. Goldman-Cecil explicitly lists uremia among the metabolic conditions contributing to the "net state of immunosuppression."
- Repeated vascular access - patients on hemodialysis have percutaneous vascular access established several times weekly, creating a portal of entry for S. aureus bacteremia and subsequent hematogenous seeding of joints. The frequency of septic arthritis in hemodialysis patients is "much increased compared with the general population." (Rheumatology, 2-Volume Set, Elsevier 2022)
- Comorbidity burden - CKD frequently coexists with diabetes, vascular disease, and immunosuppression, each of which independently elevates risk.
- Atypical presentation - the uremic immunocompromised state blunts the febrile response and inflammatory markers. The synovial WBC count may be below the usual 50,000/µL threshold despite true infection.
A 2025 review in Frontiers in Medicine (PMID: 40800124) highlights CKD as one of the three key prognostic comorbidities in septic arthritis (alongside diabetes and RA), concluding that "CKD causes uremia-induced immune dysfunction...as well as repeated vascular access increasing infection susceptibility, leading to increased mortality."
Epidemiology & Organisms
| Clinical Setting | Most Likely Organism |
|---|---|
| Native joint (CKD/HD) | S. aureus (incl. MRSA - HD is a major MRSA risk factor) |
| Hemodialysis access | S. aureus, coagulase-negative staphylococci |
| Immunocompromised/CKD | Gram-negative bacilli (Pseudomonas, Enterobacteriaceae) |
| CKD + diabetes | S. aureus, gram-negatives, atypical organisms |
| IV drug use + CKD | Pseudomonas aeruginosa, S. aureus |
Hemodialysis is listed as a specific risk factor for MRSA in septic arthritis alongside recent hospitalisation, nursing home admission, and recent antibiotic exposure. (Campbell's Operative Orthopaedics, 15th Ed 2026)
Diagnostic Challenges in CKD
Attenuated Inflammatory Response
- CKD patients may lack fever (>80% of immunocompetent adults have fever; this proportion is lower in the immunocompromised/CKD population)
- ESR and CRP are chronically elevated at baseline in CKD, reducing their diagnostic specificity
- A synovial WBC count < 50,000/µL does NOT exclude septic arthritis in immunocompromised patients - this is a critical pitfall
Diagnostic Mimics in CKD (especially relevant)
CKD creates several arthritis mimics that must be distinguished from septic arthritis:
- β2-microglobulin amyloid arthropathy - occurs with long-term HD; amyloid deposits cause joint swelling, carpal tunnel, destructive arthropathy. Synovial fluid cell count may be inflammatory.
- Crystal arthropathy - CKD predisposes to gout (urate retention) and pseudogout (calcium pyrophosphate). In CKD, however, crystal presence does NOT exclude septic arthritis - both can coexist when synovial WBC > 50,000/µL.
- Calcium hydroxyapatite deposition - especially peri-articular in HD patients
- Calcium oxalate arthropathy - in dialysis patients (excess oxalate from vitamin C metabolism)
- Erosive enthesopathy from secondary hyperparathyroidism
- Reactive arthritis from recurrent UTIs/bacteremic episodes common in CKD
Diagnostic Algorithm (Goldman-Cecil, 2024)
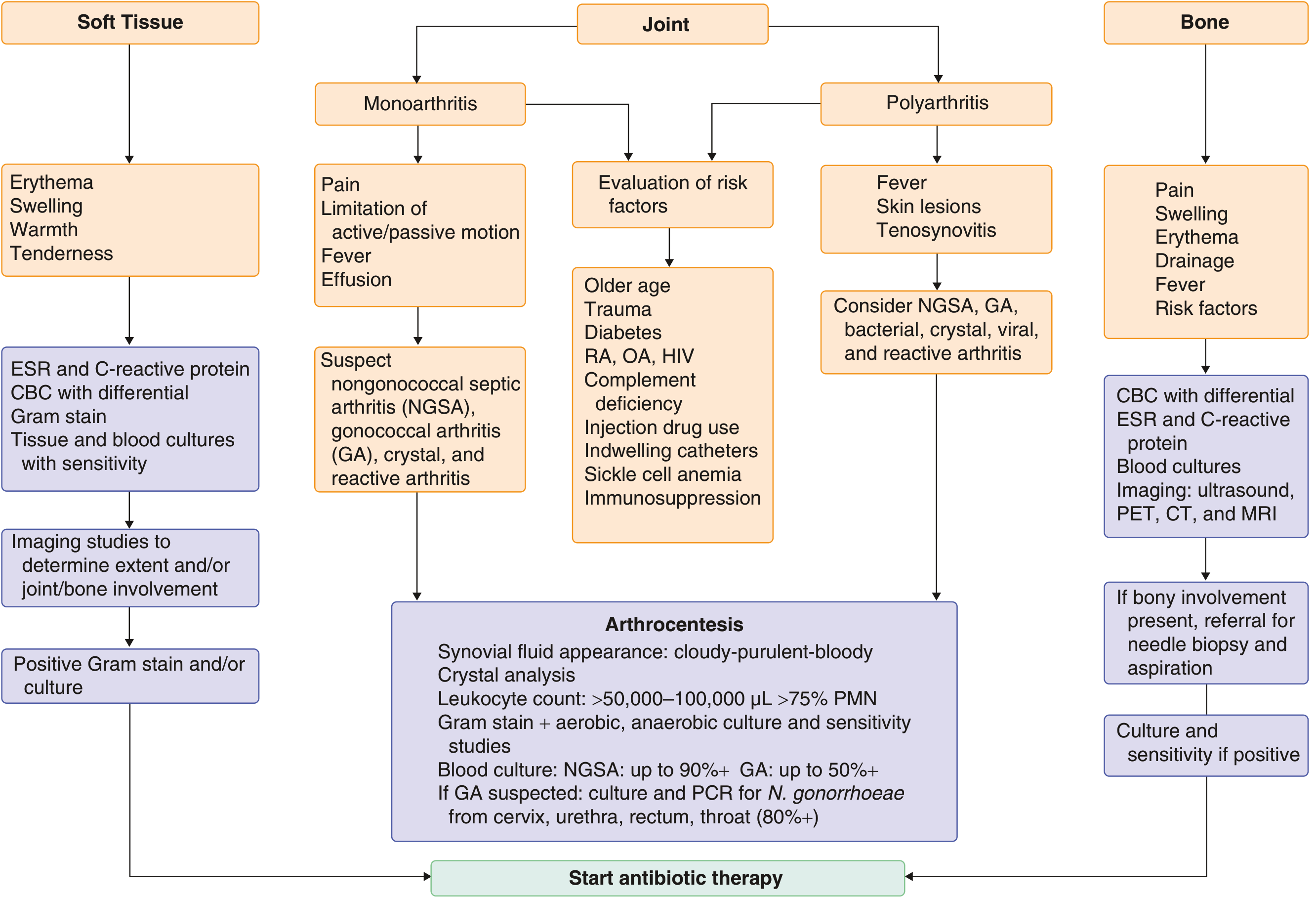
Arthrocentesis is Mandatory
- Synovial fluid: appearance (cloudy/purulent), leukocyte count + differential, crystal analysis, Gram stain, aerobic + anaerobic + fungal + mycobacterial culture
- Blood cultures: positive in up to 90% of nongonococcal septic arthritis
- In CKD with HD and line-associated bacteremia: also culture the access site
- Ultrasound or CT-guided aspiration for deep joints (hip, sacroiliac)
- The Gram stain is positive in fewer than 50% - a negative result does not rule out infection
- PCR of synovial fluid is increasingly useful, especially when prior antibiotics have been given
Treatment
General Principle
Septic arthritis is an orthopedic emergency. Even with prompt treatment, 25-50% of patients have lasting functional loss. In CKD patients, outcomes are worse due to delayed diagnosis, MRSA prevalence, and immunocompromise.
Antibiotic Selection
Empirical therapy is based on Gram stain result:
| Gram Stain | Empirical Choice | Rationale in CKD |
|---|---|---|
| Gram-positive cocci | Vancomycin 15 mg/kg IV q12h | MRSA risk is high in HD patients - never use nafcillin/oxacillin empirically |
| Gram-negative bacilli | Cefepime 2 g IV q8-12h, or piperacillin-tazobactam, or meropenem | Pseudomonas coverage needed |
| Negative / unknown | Vancomycin + broad gram-negative cover | Both gram-positives and gram-negatives possible in CKD |
Definitive therapy once cultures return:
| Organism | First Choice | Alternative |
|---|---|---|
| MSSA | Nafcillin/oxacillin 1.5-2 g IV q4-6h (4-6 wk) or cefazolin 1-2 g IV q8h | Vancomycin 15 mg/kg IV q12h; daptomycin 6-10 mg/kg IV q24h |
| MRSA | Vancomycin 15 mg/kg IV q12h or daptomycin 6-10 mg/kg IV q24h | Linezolid 600 mg PO/IV q12h; dalbavancin |
| Streptococci (pen-sensitive) | Penicillin G 20 MU/24h IV or ceftriaxone 2 g IV q24h | Vancomycin |
| Enterobacteriaceae | Ceftriaxone 1-2 g IV q24h | Ciprofloxacin 500-750 mg PO q12h |
| P. aeruginosa | Cefepime 2 g IV q8-12h | Ceftazidime 2 g IV q8h; imipenem 500 mg IV q6h; meropenem |
(Goldman-Cecil Medicine, Table 251-2)
CKD-Specific Drug Dose Adjustments
"Doses shown are based on normal renal and hepatic function and may need to be adjusted or serum levels monitored (vancomycin)." - Goldman-Cecil, Table 251-2 footnote
Key adjustments:
| Drug | CKD/HD Consideration |
|---|---|
| Vancomycin | Requires therapeutic drug monitoring (trough or AUC-guided); dose interval extended in CKD; HD patients need redosing after each session |
| Daptomycin | Dose every 48h (not 24h) when CrCl < 30 mL/min; HD patients dose after dialysis |
| Cefepime | Dose reduce when CrCl < 60 mL/min; neurotoxicity risk in CKD if not adjusted |
| Ciprofloxacin | Reduce dose in severe CKD (CrCl < 30); use with caution - QTc prolongation risk also relevant |
| Imipenem/Meropenem | Dose reduce in CKD; imipenem has a lower seizure threshold at high doses in renal failure |
| Aminoglycosides (gentamicin) | Avoid or use with extreme caution + TDM in CKD due to nephrotoxicity and ototoxicity |
| Linezolid | No renal dose adjustment needed - useful as an oral option in severe CKD |
Duration of Therapy
- Uncomplicated, susceptible organism, non-immunocompromised: 2 weeks (post-drainage)
- CKD/immunocompromised, abnormal joint, MRSA, gram-negative, or complicating osteomyelitis/bacteremia/endocarditis: 4 to 6 weeks (Firestein & Kelley's Textbook of Rheumatology)
- Consider IV-to-oral switch after 2 weeks if clinical improvement + inflammatory markers falling + bioavailable oral agent available
- Immunosuppression and lack of surgical intervention are associated with recurrence
Joint Drainage
- Serial needle aspiration is first-line for most accessible joints
- Surgical drainage is indicated for:
- Hip joint (always)
- Failure to respond to serial aspiration + antibiotics
- Developing life-threatening complications (e.g., necrotizing fasciitis)
- Arthroscopic lavage is an option where available
- Early mobilisation to prevent contractures
Prognosis in CKD
- ~40% of all septic arthritis patients have less than complete recovery
- CKD worsens outcomes through delayed diagnosis, higher MRSA burden, impaired healing
- S. aureus infection alone carries >50% poor joint outcomes and 10-15% mortality - this rate is further elevated in immunocompromised/CKD patients
- Polyarticular sepsis (more common in immunocompromised patients including CKD) carries especially high mortality
Special Considerations: Dialysis-Related Arthropathy
In long-term HD patients, β2-microglobulin amyloid arthropathy is an important differential and can coexist with septic arthritis. It should be suspected whenever synovial fluid shows an inflammatory cell count. Diagnostic joint aspiration with examination and culture is the same as for non-uremic patients - but superimposed infection on amyloid joints must always be considered. (Rheumatology, Elsevier 2022)
Key Clinical Pearls for CKD
- Don't rely on fever or high WBC to diagnose - both may be blunted in uremia
- Don't rely on a "low" synovial WBC to exclude - counts < 50,000/µL can still represent infection in CKD
- Cover MRSA empirically - hemodialysis is a major risk factor
- Crystal arthritis + infection can coexist - crystals in synovial fluid do not exclude septic arthritis
- Adjust all renally-cleared antibiotics - vancomycin requires TDM; avoid or carefully dose aminoglycosides
- Extend antibiotic duration - 4-6 weeks in immunocompromised/CKD hosts
- Always culture blood + dialysis access site - hematogenous spread from access is a common source
- Screen for endocarditis - S. aureus bacteremia in HD patients has high rates of endocarditis; consider echocardiography
Sources:
- Goldman-Cecil Medicine, International Edition (PMID-linked textbook, Section 251)
- Harrison's Principles of Internal Medicine, 22nd Ed, 2025 (Chapter on nongonococcal bacterial arthritis)
- Firestein & Kelley's Textbook of Rheumatology (Antibiotic therapy chapter)
- Rheumatology, 2-Volume Set, Elsevier 2022 (Dialysis-related arthropathy section)
- Campbell's Operative Orthopaedics, 15th Ed 2026 (MRSA risk factors)
- Khudair A et al. "The prognostic implications of comorbidities in septic arthritis." Front Med (Lausanne) 2025. PMID: 40800124
This is a shared conversation. Sign in to Orris to start your own chat.