classify Cutaneous T Cell Lymphoma .Discuss mycosis fungoides in 10marks format for 3rd yr dermatology post graduate theory examination
Reading File
Finding Sources
Finding Sources
Searching PubMed
"mycosis fungoides" AND "cutaneous T-cell lymphoma"
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Searching Images
mycosis fungoides histopathology epidermotropism Pautrier microabscess
I now have all the information needed to write a comprehensive 10-marks postgraduate answer. Let me compose it.
Classification of Cutaneous T-Cell Lymphoma (CTCL) & Mycosis Fungoides — 10 Marks
CLASSIFICATION OF CUTANEOUS T-CELL LYMPHOMA (CTCL)
CTCL describes a heterogeneous group of neoplasms of skin-homing T cells representing ~75–80% of all primary cutaneous lymphomas. The current classification is based on the WHO-EORTC (2018/2022) consensus, incorporating clinical, histologic, immunophenotypic, and genetic criteria.
WHO-EORTC Classification of Primary Cutaneous T-Cell Lymphomas
Indolent course (good prognosis):
| Entity | 5-yr Survival |
|---|---|
| Mycosis fungoides (MF) | ~88% (early stage) |
| Folliculotropic MF | ~75% |
| Pagetoid reticulosis (Woringer–Kolopp) | Excellent |
| Granulomatous slack skin | ~50% |
| Primary cutaneous CD30+ lymphoproliferative disorders | |
| — Lymphomatoid papulosis (LyP) types A, B, C, D, E | >95% |
| — Primary cutaneous anaplastic large cell lymphoma (pcALCL) | ~95% |
| Primary cutaneous CD4+ small/medium T-cell lymphoproliferative disorder | >90% |
| Primary cutaneous acral CD8+ T-cell lymphoma | Excellent |
Aggressive course (poor prognosis):
| Entity | 5-yr Survival |
|---|---|
| Sézary syndrome | ~24–36% |
| Primary cutaneous aggressive epidermotropic CD8+ cytotoxic T-cell lymphoma | <20% |
| Primary cutaneous γ/δ T-cell lymphoma | <20% |
| Extranodal NK/T-cell lymphoma, nasal type | Poor |
| Subcutaneous panniculitis-like T-cell lymphoma (αβ type) | ~80% |
| Adult T-cell leukemia/lymphoma (HTLV-1 associated) | Poor |
| Primary cutaneous peripheral T-cell lymphoma, NOS | ~16% |
Key principle: CTCLs should NOT be classified as nodal lymphomas presenting in skin. They have distinct biology, prognosis, and management.
MYCOSIS FUNGOIDES (MF)
1. Definition & Epidemiology
Mycosis fungoides is the most common CTCL, accounting for ~50% of all primary cutaneous lymphomas. It is a neoplasm of skin-homing memory CD4+ T-helper cells (rarely CD8+). The incidence is ~0.4 per 100,000/year in the US, with an increasing trend. It predominantly affects older adults (median age at diagnosis: 55–60 years), with a male-to-female ratio of 1.6–2:1, and is more prevalent in Black populations.
The name was coined by Alibert in 1806 (pian fungoide), renamed in 1835 due to tumor resemblance to mushrooms. Bazin (1870) described the classic three-stage progression.
2. Pathogenesis
- Cell of origin: Skin-homing memory T-helper (CD4+) cells expressing CLA (cutaneous lymphocyte antigen) — the ligand for E-selectin on inflamed skin endothelium — and CCR4, which binds ligands on basal keratinocytes, facilitating persistent skin homing.
- Molecular events (multistep model):
- Early MF: overexpression of TOX transcription factor and PDCD1 (PD-1); both are diagnostic markers.
- Advanced MF: deletion of CDKN2A (tumor suppressor), deletions of HNRNPK and SOCS1 (both inhibitors of JAK-STAT pathway) → constitutive STAT3 activation → uncontrolled proliferation.
- Chromosomal gains: 7q36, 7q21–22; losses: 5q13, 9p21.
- Immunologic shift: Early MF has a Th1 microenvironment (CD8+ TILs contain the clone). Advanced MF shifts to Th2 (via IL-4, IL-10), suppressing CD8+ cytotoxic control and enabling immune evasion.
- Staphylococcus aureus colonization activates STAT3 signaling, stimulates IL-2R expression on tumor cells, and α-toxin blocks CD8+ killing — worsening disease activity. Antibiotic treatment can improve clinical scores.
- No definitive viral etiology has been confirmed (HTLV-1 not causative in MF).
3. Clinical Features — Three Classic Stages (Alibert–Bazin)
Stage I — Patch Stage:
- Flat, erythematous, slightly scaly patches, often >5 cm
- Distribution: "Bathing suit area" — lower abdomen, buttocks, upper thighs, breasts in women; sparing sun-exposed areas
- Lesions may be atrophic, poikilodermatous (atrophy + telangiectasia + dyspigmentation = Poikilodermia vasculare atrophicans, pathognomonic of patch-stage MF)
- Resembles eczema; pruritus often present; scratch marks and lichenification typically absent (unlike true eczema)
- May persist for years

Stage II — Plaque Stage:
- Lesions become indurated/infiltrated; may resemble psoriasis or subacute dermatitis
- Palpation reveals thickness; coalescence leads to large plaques up to 30 cm
- Palms and soles may show hyperkeratotic, psoriasiform plaques
- Lymph nodes may become enlarged (firm, nontender, freely movable)
Stage III — Tumor Stage:
- Nodular/hemispherical tumors arising on plaques; surface may ulcerate
- Associated with poor prognosis; lymph node and visceral involvement develop
- d'emblée form (tumors from the onset, without preceding patches/plaques) is now recognized as a different type of CTCL
Other presentations:
- Erythrodermic MF: Generalised exfoliative erythroderma
- Folliculotropic MF: Acneiform papules/plaques on head & neck with alopecia; more treatment-resistant
- Hypopigmented MF: Common in darker-skinned children and young adults
- Pagetoid reticulosis (Woringer–Kolopp): Solitary hyperkeratotic lesion on extremity
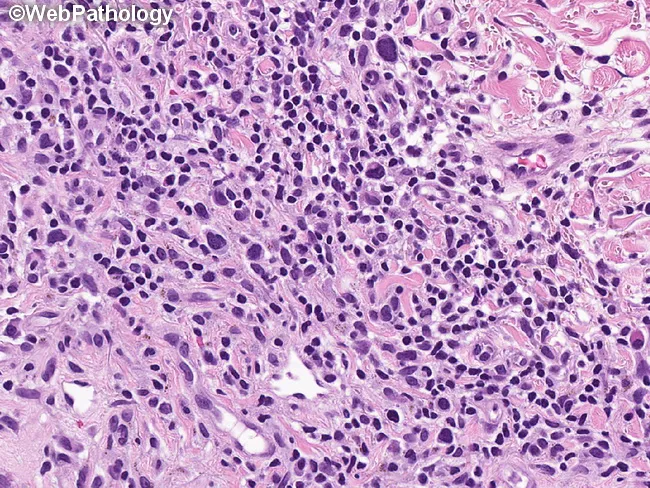
4. Histopathology
The hallmark is epidermotropism — infiltration of epidermis by atypical lymphocytes disproportionate to the degree of spongiosis.
Patch stage:
- Subtle epidermotropism: lymphocytes align along the basal layer (lichenoid pattern)
- Perivascular bandlike infiltrate in papillary dermis
- Papillary dermal fibrosis (haphazardly arranged collagen bundles) — an early sign
- "Bare underbelly" sign: lymphoid infiltrate denser above the postcapillary venule than below
Plaque stage:
- Dense bandlike superficial infiltrate + deeper perivascular component
- Epidermotropism marked, spongiosis minimal or absent (key distinction from eczema)
- Pautrier microabscesses — intraepidermal collections of neoplastic T cells within lacunae (pathognomonic but present in only ~10% of early biopsies; more common in plaques)
Tumor stage:
- Dense sheets of atypical lymphocytes in dermis and subcutis
- Cerebriform nuclei (markedly infolded nuclear membrane) — characteristic
- Epidermotropism may paradoxically diminish
Cardinal histologic features of MF:
- Solitary/small groups of lymphocytes in the basal layer
- Epidermotropism with disproportionately scant spongiosis
- Intraepidermal lymphocytes larger and darker than dermal lymphocytes
- Papillary dermal fibrosis
- Folliculotropism/syringotropism with intrafollicular mucin (follicular mucinosis)
5. Immunophenotype & Molecular Studies
| Marker | Result |
|---|---|
| CD3 | Positive |
| CD4 | Positive (majority) |
| CD8 | Rare aggressive variant |
| CD7 | Lost (key aberrant marker) |
| CD26 | Lost (key aberrant marker; CD4+CD26- clone in peripheral blood) |
| CD5 | Often reduced |
| TCR αβ | Positive (majority) |
| CD30 | Positive in large cell transformation |
- T-cell receptor (TCR) gene rearrangement by PCR or Southern blot: demonstrates clonal T-cell population (identical rearrangement at multiple sites confirms MF)
- Flow cytometry: circulating CD4+CD7− or CD4+CD26− cells increase with disease stage
- In advanced disease, loss of CD7 in epidermal lymphocytes with preserved CD7 in dermal infiltrate strongly supports MF
6. Staging (TNMB System — ISCL/EORTC)
| Component | Score |
|---|---|
| T (Skin) | T1: <10% BSA patches/plaques; T2: ≥10% BSA; T3: tumors; T4: erythroderma |
| N (Nodes) | N0: normal; N1: palpable, pathologically benign; N2: not palpable, pathologically MF; N3: clinically and pathologically involved |
| M (Viscera) | M0: none; M1: involved |
| B (Blood) | B0: none; B1: involved |
Stage groupings:
- Stage IA: T1 N0 M0
- Stage IB: T2 N0 M0
- Stage IIA: T1–2, N1, M0
- Stage IIB: T3, N0–1, M0
- Stage IIIA/B: T4, N0–1, M0
- Stage IVA: any T, N2–3, M0
- Stage IVB: any T, any N, M1
7. Prognosis
| Stage | 10-yr Disease-Related Survival |
|---|---|
| IA | 96% (same as age-matched controls) |
| IB | 77–83% |
| IIB | 42% |
| IV | ~20% |
Poor prognostic factors: lymphadenopathy, skin tumors, ulceration (median survival 1 year if all three present), non-Caucasian race with early onset, large cell transformation (>25% large cells), elevated LDH.
Cause of death in most cases: septicemia (opportunistic infections due to Th2-mediated immunosuppression).
8. Differential Diagnosis
| Condition | Key Distinguishing Feature |
|---|---|
| Atopic eczema | Scratch marks, lichenification; spongiosis on biopsy |
| Psoriasis | Silvery scales, nail changes; Munro microabscesses |
| Parapsoriasis | Overlaps; large-plaque type is essentially patch MF |
| Pigmented purpuric dermatoses | Hemosiderin, not epidermotropism |
| Drug-induced pseudolymphoma | Drug history; resolves on withdrawal |
| Sézary syndrome | Erythroderma + leukemia of Sézary cells + lymphadenopathy |
9. Variants of Mycosis Fungoides (WHO-EORTC recognized)
- Folliculotropic MF — follicular papules, acneiform lesions, alopecia on head/neck; follicular mucinosis; worse prognosis than classic MF; requires aggressive therapy (radiotherapy, bexarotene)
- Pagetoid reticulosis (Woringer–Kolopp) — solitary localized hyperkeratotic patch/plaque on extremity; epidermis massively infiltrated with CD4+ or CD8+ cells; excellent prognosis; localized RT curative
- Granulomatous slack skin — pendulous skin folds in axillae/groins; granulomatous infiltrate with elastolysis; associated with Hodgkin lymphoma; poor response to therapy
(Clinical variants — bullous, hypopigmented, follicular, vesicular, syringotropic — follow a similar clinical course and are not classified separately.)
10. Treatment (Stage-Based)
Skin-directed therapies (early stages IA–IIA):
- Topical corticosteroids (high-potency): first-line for limited disease
- Topical nitrogen mustard (mechlorethamine HCl): effective; gel formulation (Valchlor) available
- Topical carmustine (BCNU)
- PUVA (psoralen + UVA): highly effective for patch/plaque stage; complete remission in up to 70% stage IB
- Narrowband UVB: for thin patches
- Localised radiotherapy (RT): MF is exquisitely radiosensitive; curative for solitary lesions
- Total skin electron beam therapy (TSEB): 30–36 Gy for extensive plaques/tumors; high response rate
Systemic therapies (advanced stages IIB–IV):
- Retinoids: bexarotene (RXR agonist) — oral; response rate ~45%; hypertriglyceridemia is main side effect
- Interferon-α (IFN-α): immunomodulatory; ~50% response, often combined with PUVA
- HDAC inhibitors: vorinostat and romidepsin (~35% overall response rate); fatigue, thrombocytopenia
- Extracorporeal photopheresis (ECP): first-line for erythrodermic MF/Sézary syndrome
- Mogamulizumab: anti-CCR4 monoclonal antibody; superior to vorinostat in MF/SS
- Brentuximab vedotin: anti-CD30 antibody–drug conjugate; effective in CD30+ MF
- Single-agent chemotherapy: gemcitabine, liposomal doxorubicin for refractory disease
- Combination chemotherapy (CHOP): reserved for unequivocal lymph node/visceral involvement; responses short-lived
- Allogeneic HSCT: for young patients with refractory/progressive MF; graft-versus-tumor effect critical; autologous HSCT results disappointing
Principle: Early aggressive chemotherapy in an attempt to "cure" MF is contraindicated — associated with excess morbidity/mortality. Treatment is palliative and stage-directed.
Summary Box (Examiner's Highlights)
| Feature | Key Point |
|---|---|
| Cell of origin | Memory CD4+ T-helper cells |
| Classic triad | Patches → Plaques → Tumors |
| Distribution | Bathing-suit area (sun-protected) |
| Histology | Epidermotropism, Pautrier microabscesses, cerebriform nuclei |
| Immunophenotype | CD3+, CD4+, CD7−, CD26− |
| Prognosis indicator | Stage; lymphadenopathy, tumors, ulceration = worst |
| Stage IA survival | Identical to general population |
| Most common cause of death | Septicemia |
| First-line early stage | Topical steroids, PUVA, TSEB |
| Novel targeted agents | Mogamulizumab (anti-CCR4), Brentuximab vedotin (anti-CD30) |
Sources: Dermatology 2-Volume Set 5e (Willemze & Kempf, Chapter 120); Andrews' Diseases of the Skin (Chapter 32); Robbins Pathologic Basis of Disease; Fitzpatrick's Dermatology.
Discuss cutaneous tuberculosis.In 10marks format for 3rd yr dermatology post graduate theory examination
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Searching Images
lupus vulgaris apple jelly diascopy cutaneous tuberculosis
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
This is a shared conversation. Sign in to Orris to start your own chat.