High altitude pulmonary edema
Reading File
Finding Sources
Searching PubMed
"high altitude pulmonary edema"[MeSH Terms]
Reading File
Reading File
Reading File
Reading File
Searching PubMed
"high altitude pulmonary edema" AND pathophysiology
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
I now have comprehensive information from multiple authoritative textbooks. Let me compile the full answer.
High-Altitude Pulmonary Edema (HAPE)
HAPE is the most common fatal manifestation of high-altitude illness. It is a noncardiogenic, hydrostatic pulmonary edema that was historically misdiagnosed as pneumonia or congestive heart failure until landmark work by Hultgren and Houston established it as a distinct entity.
Definition and Epidemiology
- Develops typically 2-4 days after arrival at altitudes >2400 m (8000 ft); rarely after >4-5 days at the same altitude
- Incidence ranges from <0.01% in Colorado skiers to 2-3% of climbers on Mt. Denali; uncommon below 10,000 ft but can be fatal even at 8000 ft
- Men more susceptible than women; strong, fit individuals are paradoxically at higher risk because fitness enables faster ascent
Pathophysiology
HAPE is a noncardiogenic pulmonary edema with normal left ventricular function. Left ventricular end-diastolic pressure, pulmonary capillary wedge pressure, and left atrial pressures are all low-to-normal, while pulmonary vascular resistance and pulmonary artery (PA) pressure are markedly elevated.
The central mechanism involves exaggerated hypoxic pulmonary vasoconstriction (HPV):
- Uneven hypoxic vasoconstriction - some arterioles constrict more than others, causing overperfusion in downstream capillary beds where vasoconstriction fails to protect
- Elevated microvascular pressure (PA pressure >18 mmHg) causes capillary "stress failure" - a mechanical injury to the capillary wall along a continuum from increased permeability to frank rupture and alveolar hemorrhage
- Endothelial dysfunction - hypoxia impairs nitric oxide (NO) release, a vasodilator, worsening vasoconstriction
- Impaired alveolar fluid clearance - hypoxia downregulates epithelial sodium channel (ENaC) activity, reducing transalveolar fluid transport
- Inflammation is secondary, not primary - bronchoalveolar lavage (BAL) within the first 24 hours shows high protein and RBC content (confirming mechanical stress), but no cytokines or neutrophil recruitment. Inflammation may accelerate HAPE when viral respiratory infections prime the endothelium.
HAPE-susceptible individuals have a low hypoxic ventilatory response paired with exaggerated microvascular vasoconstriction, and tend to experience recurrent HAPE with repeated altitude exposure.
Risk Factors
| Factor | Details |
|---|---|
| Rapid ascent | Most important modifiable risk |
| Prior HAPE history | Strong predictor of recurrence |
| Male sex | ~4x more common than in women |
| Cold temperature | Elevates PA pressure |
| Heavy exertion | Increases PA pressure |
| Respiratory infection | Primes endothelial vulnerability; especially important in children |
| Pulmonary hypertension | Mitral stenosis, primary PAH, unilateral absent pulmonary artery |
| Cardiac shunts | ASD, PDA, patent foramen ovale (PFO - 4x more common in HAPE-susceptible individuals) |
| Re-entry HAPE | High-altitude residents returning after a trip to low altitude |
Clinical Features
Early
- Decreased exercise performance (greater than expected for altitude)
- Prolonged recovery from exertion
- Dry, persistent cough
- Dyspnea on exertion
- Localized rales, typically right mid-lung field
- SpO2 typically 10-20 points below expected for that altitude
Progression (worsens at night, typically 2nd night at new altitude)
- Dyspnea at rest (red flag warning)
- Productive cough (clear, watery sputum); hemoptysis in severe cases
- Tachycardia, tachypnea
- Low-grade fever (up to 38.5°C)
- Cyanosis (nail beds → central)
- Diffuse bilateral rales, rhonchi - "gurgles audible without a stethoscope"
Severe / Late
- Ataxia and altered mental status (due to hypoxemia or concurrent HACE)
- Coma, then death if untreated
Note: HAPE may be accompanied by signs of HACE. Rales are absent at rest in ~15% of HAPE patients but can be elicited immediately after brief exercise.
Chest Radiograph
HAPE shows patchy or localized alveolar opacities that are right-sided initially, progressing to bilateral involvement. Normal heart size distinguishes it from cardiogenic edema.
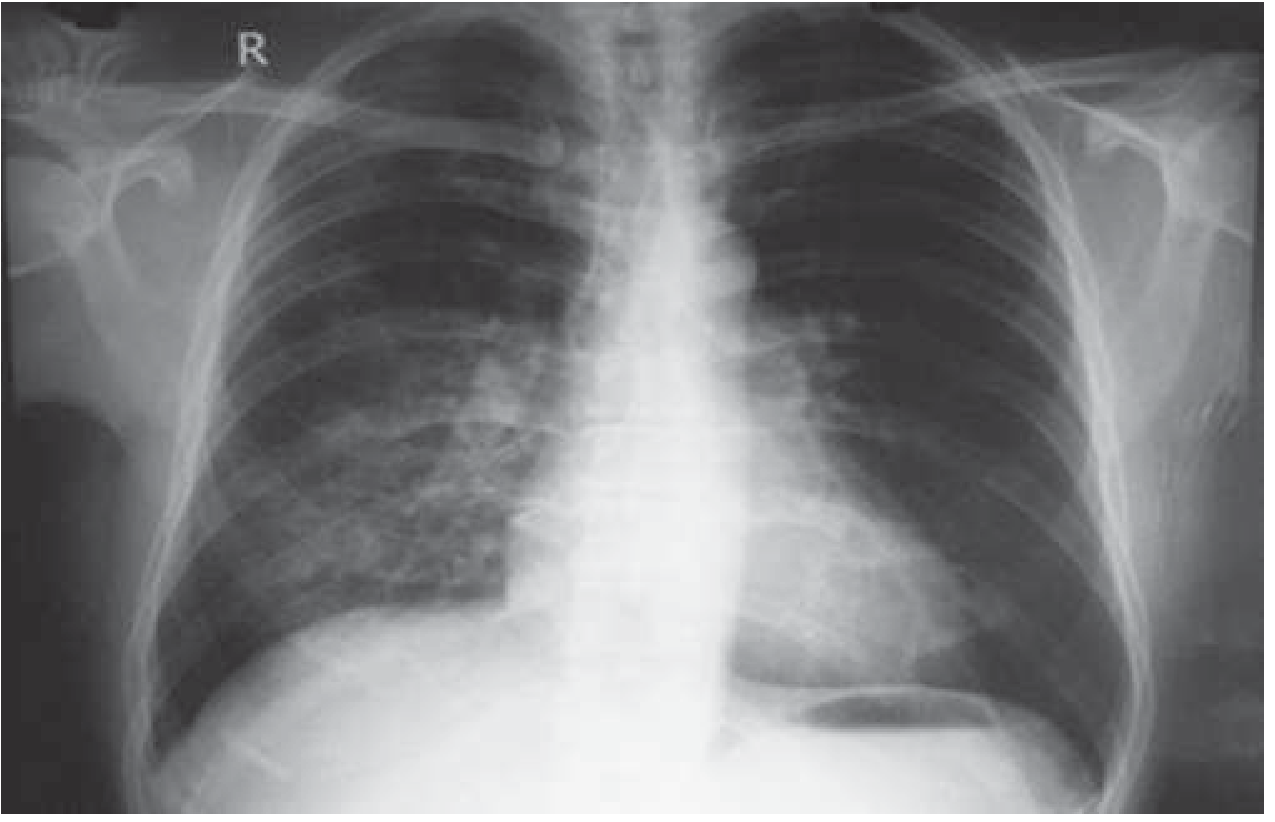
Chest X-ray showing right middle/lower zone opacity in HAPE, which cleared almost completely in 2 days with descent and oxygen (Harrison's Principles of Internal Medicine, 22E)
Key radiology points:
- Kerley B lines and bat-wing appearance are NOT seen (contrast with cardiogenic edema)
- ECG may show right ventricular strain or hypertrophy; right-axis deviation
- ABG: severe hypoxemia + respiratory alkalosis consistently present
- Pulse oximetry is adequate; formal ABG not required for diagnosis
Lung ultrasound: B-lines (comet-tail scoring) are sensitive but not specific - frequently seen in individuals who never develop clinical HAPE; clinical correlation is essential.
Differential Diagnosis
- Pneumonia (most commonly confused with HAPE)
- Pulmonary embolism
- Acute coronary syndrome / heart failure
- Pneumothorax
- Carbon monoxide poisoning
- HACE (can coexist)
- Anxiety attack / panic
Investigations
- Pulse oximetry - adequate for evaluation; SpO2 dramatically lower than others at same altitude
- Chest X-ray - patchy opacities, normal heart size
- ECG - right ventricular strain, right-axis deviation
- Echocardiography - indicated when HAPE occurs at low altitude (<3000 m) or when cardiac abnormality is suspected; also used to exclude cardiac component
- Right heart catheterization (research setting): elevated PA pressure with normal wedge pressure
Treatment
Priority order: Descend → Oxygen → Drugs
| Intervention | Details |
|---|---|
| Immediate descent | Treatment of choice; minimize patient exertion during descent (overexertion during descent has caused deaths) |
| Supplemental oxygen | Immediately lowers PA pressure and improves SaO2; can resolve HAPE without descent but may require 36-72 hours; lifesaving when descent not possible |
| Portable hyperbaric bag (Gamow bag) | Useful adjunct when descent not immediately possible; simulates descent |
| Nifedipine | 30 mg slow-release every 12 hours; reduces PA pressure 30-50% but only slightly increases SaO2; use when O2/descent unavailable |
| Tadalafil | 10 mg every 12 hours; PDE-5 inhibitor, blunts HPV via NO generation |
| Sildenafil | Similar mechanism to tadalafil |
| Salmeterol (inhaled) | Upregulates ENaC, enhances alveolar fluid clearance; limited treatment data, more established for prophylaxis |
| Bed rest | Adequate for very mild cases |
| Keep patient warm | Cold stress elevates PA pressure |
When oxygen is available, adjunctive drugs such as nifedipine may be unnecessary. Antibiotics are only indicated if concurrent infection is confirmed or strongly suspected.
Discharge criteria (hospital setting): Progressive clinical and radiographic improvement + PaO2 ≥60 mmHg or SpO2 >90%
Prophylaxis (for susceptible individuals)
| Drug | Regimen |
|---|---|
| Nifedipine | 30 mg slow-release every 12 hours during ascent, continue 3 days (monitor for hypotension); 20 mg SR every 8 hours is an alternative |
| Tadalafil | 10 mg twice daily, starting 24 hours before ascent |
| Sildenafil | Similar to tadalafil |
| Salmeterol | Twice daily inhaled; reduces HAPE incidence by ~50% in repeat-episode patients |
| Gradual ascent | The most important preventive measure - no more than 300-500 m/day sleeping altitude gain above 3000 m |
Prognosis
- With early recognition and treatment, HAPE is rapidly reversible - one of the most treatable causes of acute respiratory failure
- No residual fibrosis or abnormal pulmonary function reported
- Prior HAPE is not a contraindication to future ascent, but staged ascent and prophylaxis counseling are advised
- Death occurs from failure of early recognition, misdiagnosis, or inability to descend
Sources: Harrison's Principles of Internal Medicine 22E (2025) | Murray & Nadel's Textbook of Respiratory Medicine | Tintinalli's Emergency Medicine | Rosen's Emergency Medicine | Fishman's Pulmonary Diseases and Disorders
Recent PubMed review (PMID 39331568, High Alt Med Biol 2025) confirms the established pathophysiologic framework, with ongoing interest in the molecular mechanisms of HPV and NO signaling. A 2026 review (PMID 41571626, Signal Transduct Target Ther) covers altitude hypoxia management consistent with the above.
This is a shared conversation. Sign in to Orris to start your own chat.