Cold agglutination test
Reading File
Finding Sources
Finding Sources
Searching PubMed
"cold agglutinin" AND diagnosis
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Reading File
I now have comprehensive information to deliver a thorough answer.
Cold Agglutination Test
What Is It?
The cold agglutination test detects cold agglutinins - antibodies (usually IgM) that bind to red blood cell (RBC) surface carbohydrate antigens at temperatures of 0-4°C, causing erythrocyte agglutination. This agglutination is reversible upon rewarming to 37°C, which distinguishes it from true RBC clumping.
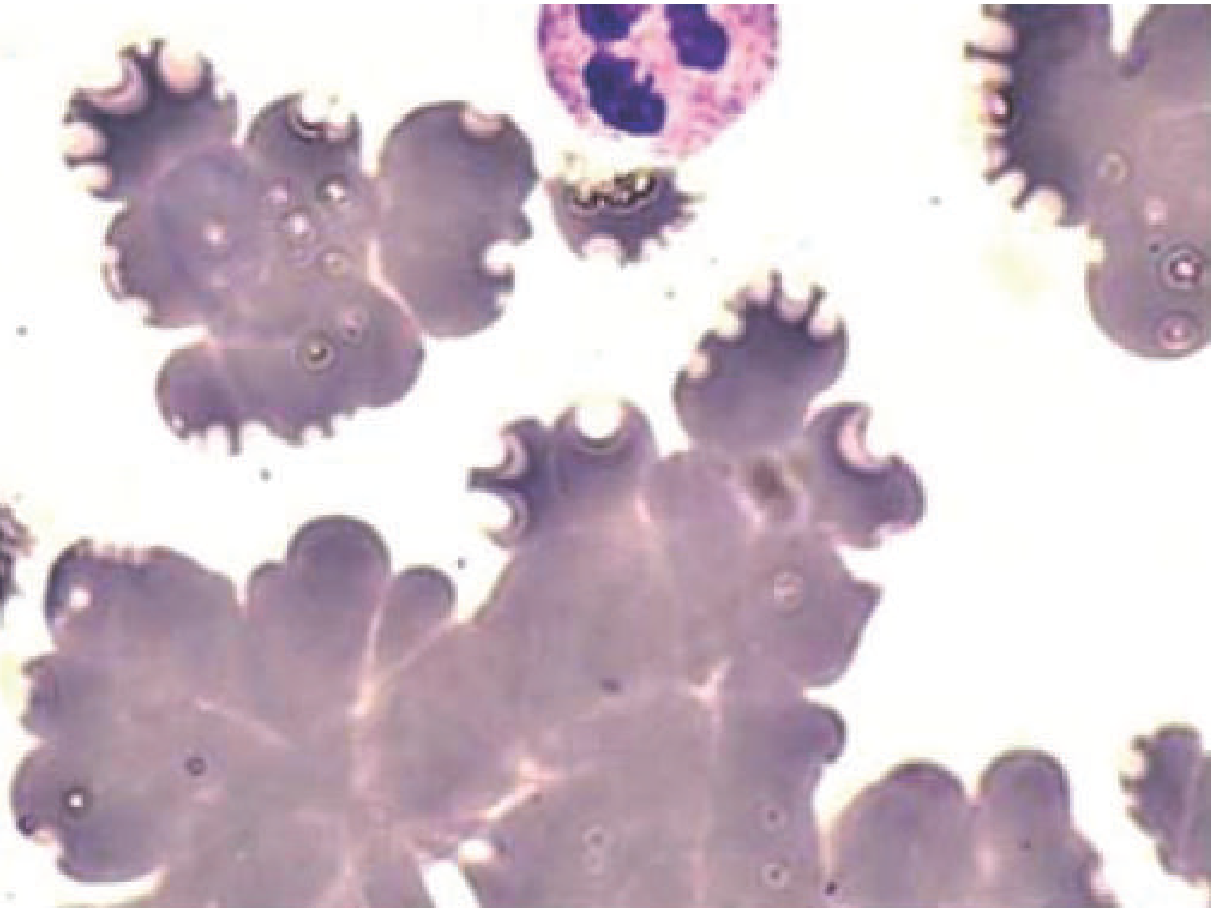
Peripheral Blood Smear Appearance
Below is the characteristic "bunch of grapes" appearance of cold agglutinin-induced RBC clustering (May-Grünwald-Giemsa stain, 1000x), which differs from rouleaux formation ("stack of coins"):
Bedside (Rapid) Cold Agglutination Test
A quick version of the test can be done at the bedside without a laboratory:
- Draw 1 mL of blood into a prothrombin time (citrate) tube
- Before cooling - examine: should see a smooth coating of RBCs on the tube wall
- Cool to 4°C - place on ice or in a standard refrigerator for several minutes
- Examine for macroscopic erythrocyte agglutination (visible clumping)
- Rewarm to 37°C (incubator or body heat)
- Agglutination should completely dissociate, returning to the original smooth appearance
Interpretation:
- Positive bedside test correlates with a laboratory titer of ≥ 1:64 - highly suggestive of Mycoplasma pneumoniae infection
- A titer of ≥ 1:32 is also highly suggestive of M. pneumoniae
- Titers ≥ 1:128 are usually caused by M. pneumoniae infection
(Goldman-Cecil Medicine; Andrews' Diseases of the Skin)
Causes / Associated Conditions
| Antibody Type | Associated Conditions | Titer |
|---|---|---|
| Polyclonal IgM | M. pneumoniae, EBV (infectious mononucleosis), CMV, other viral infections | Moderate |
| Monoclonal IgM | Idiopathic cold agglutinin disease (CAD), B-cell lymphoma, Waldenström macroglobulinemia | Very high (1:10,000 to 1:1,000,000) |
| Benign / normal | Healthy individuals (no clinical significance) | Low (<1:64) |
Cold agglutinin disease (CAD) accounts for about 20% of all autoimmune hemolytic anemias (AIHA). It typically affects individuals over 50 years old, more commonly females.
(Henry's Clinical Diagnosis; Tietz Textbook of Laboratory Medicine)
Antibody Specificity
- Anti-I: Most frequent in idiopathic CAD and M. pneumoniae infection - reacts with virtually all adult RBCs
- Anti-i: Seen in infectious mononucleosis and lymphoproliferative disorders (10-20% of EBV mononucleosis patients have elevated titers)
- Anti-Pr: Less common, also associated with CAD
- Heavy-chain gene restriction IGHV4-34 is characteristic of monoclonal cold agglutinins; primary CAD often has mutations in KMT2D or CARD11 genes
Laboratory Interference (Clinical Pitfalls)
Cold agglutinins cause several spurious CBC results if the sample is analyzed while cold:
| Parameter | Effect |
|---|---|
| RBC count | Falsely low (clumped cells counted as one) |
| Hematocrit | Falsely decreased |
| MCV | Grossly increased (clumps measured as giant cells) |
| MCH / MCHC | Falsely elevated |
| RDW | Falsely increased |
| Hemoglobin | Not affected (lysed before measurement) |
Key: Hemoglobin is measured after RBC lysis, so it is not affected - this creates the paradox of a falsely high MCHC alongside a normal hemoglobin.
Corrective action: Warm the EDTA sample to 37°C and analyze immediately. If the anomaly reappears when the sample cools back to 4°C, cold agglutinins are confirmed.
(Tietz Textbook of Laboratory Medicine)
Pathophysiology of Hemolysis
- Cold agglutinins bind RBCs in peripheral cool vessels (extremities, temperature ≤32°C)
- As blood recirculates to the warm body core (37°C), the antibody dissociates but complement (C3b) remains bound
- Hemolysis occurs primarily via extravascular (C3b-mediated) pathways in the reticuloendothelial system (liver macrophages), though intravascular hemolysis can occur too
- Direct Antiglobulin Test (DAT): positive with polyspecific and anti-C3 reagents, but negative with anti-IgG alone
Clinical Relevance in Mycoplasma pneumoniae
The cold agglutination test was historically used to support a diagnosis of Mycoplasma pneumonia. However, it is now rarely used because:
- PCR assays are far more sensitive and specific
- Cold agglutinins are not accurate in children under 12
- Antibody tests have poor sensitivity/specificity vs. PCR
- Results take at least a day (even the rapid version requires a few hours of processing)
At high titers, cold agglutinins in M. pneumoniae can cause clinical complications: Raynaud phenomenon, acrocyanosis, and rarely digital necrosis (especially in sickle cell disease patients).
Recent Evidence
A 2025 review by Berentsen (PMID 41348049) in Hematology ASH Education Program covers updated diagnosis and management of cold agglutinin disease. Reviews from 2024 (PMIDs 39487134 and 39371250) address autoimmune hemolytic anemias broadly, with no major contradictions to classical textbook guidance on the cold agglutination test itself.
Sources: Goldman-Cecil Medicine; Henry's Clinical Diagnosis and Management by Laboratory Methods; Tietz Textbook of Laboratory Medicine, 7th Ed.; Rosen's Emergency Medicine; Andrews' Diseases of the Skin
This is a shared conversation. Sign in to Orris to start your own chat.