Difference between ulcerative colitis and chrons diseases according to Robbins pathology
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have all the information I need from both Robbins books to provide a comprehensive answer. Let me compile the full comparison.
Ulcerative Colitis vs. Crohn Disease - According to Robbins Pathology
Here is the diagram from Robbins & Cotran Pathologic Basis of Disease (Fig. 17.35) showing the key differences at a glance:
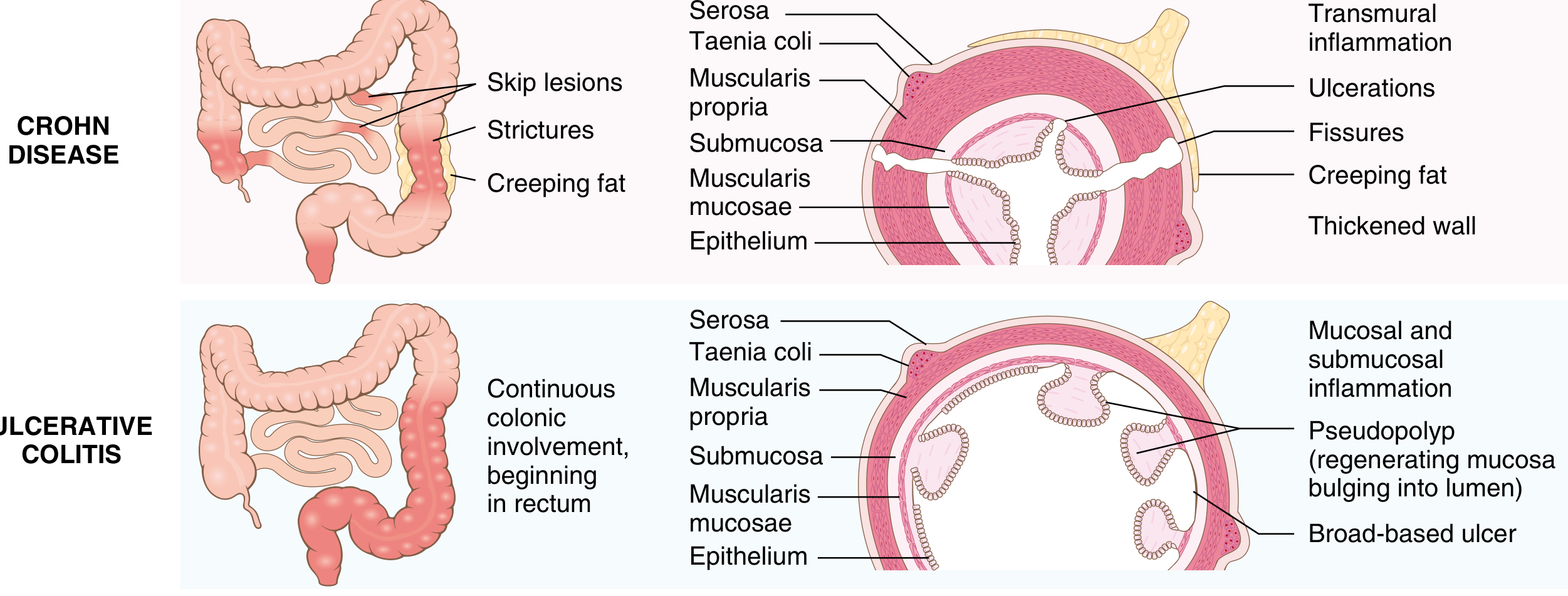
Overview
Both are chronic inflammatory conditions triggered by dysregulated host immune responses to intestinal microbiota in genetically predisposed individuals. The distinction is based primarily on distribution of affected sites and morphologic expression of disease.
The Master Comparison Table (Robbins Table 17.8 / Table 13.5)
| Feature | Crohn Disease | Ulcerative Colitis |
|---|---|---|
| MACROSCOPIC | ||
| Bowel region | Ileum ± colon (any GI tract) | Colon only |
| Rectal involvement | Sometimes | Always |
| Distribution | Skip lesions | Diffuse/continuous |
| Stricture | Yes (common) | Rare |
| Bowel wall | Thick (rubbery) | Thin (normal) |
| Cobblestone mucosa | Yes | No |
| Creeping fat | Yes | No |
| MICROSCOPIC | ||
| Depth of inflammation | Transmural | Limited to mucosa/submucosa |
| Pseudopolyps | Moderate | Marked |
| Ulcers | Deep, knife-like | Superficial, broad-based |
| Lymphoid reaction | Marked | Moderate |
| Fibrosis | Marked | Mild to none |
| Serositis | Marked | Mild to none |
| Granulomas | Yes (~35%) | No |
| Fistulae/sinuses | Yes | No |
| Crypt abscesses | Yes | Yes |
| CLINICAL | ||
| Perianal fistula | Yes (in colonic disease) | No |
| Fecal fat malabsorption | Yes | No |
| Malignant potential | Yes | Yes |
| Recurrence after surgery | Common | No (curative) |
| Toxic megacolon | No | Yes |
| p-ANCA positive | ~10% | ~75% |
| Smoking effect | Worsens disease | Cessation can trigger onset |
Detailed Breakdown
1. Location and Distribution
Crohn Disease:
- Can involve any part of the GI tract from mouth to anus
- Most common sites: terminal ileum, ileocecal valve, and cecum
- ~40% small intestine only; ~30% small intestine + colon; remainder colon only
- Characterized by skip lesions - multiple separate, sharply delineated areas of disease with normal mucosa in between
- Pancolitis (colonic Crohn) can be difficult to distinguish from UC
Ulcerative Colitis:
- Limited strictly to the colon and rectum
- Always involves the rectum and extends proximally in a continuous fashion
- Pancolitis = entire colon involved; or limited to left-sided/proctosigmoiditis
- Mild distal ileal inflammation (backwash ileitis) may occur in severe pancolitis but small intestine is otherwise spared
- A "cecal red spot" may be present in left-sided UC but there are no true skip lesions
2. Gross Morphology
Crohn Disease:
- Earliest lesion: aphthous ulcer, progressing to elongated serpentine ulcers along the long axis
- Edema and loss of normal mucosal folds
- Cobblestone appearance from ulceration with sparing of intervening mucosa
- Fissures extending deeply - form peritoneal abscesses, perforations, or fistula tracts (bowel-bowel, bowel-bladder, bowel-vagina, perianal skin)
- Wall is thickened and rubbery due to transmural edema, inflammation, submucosal fibrosis, and muscularis propria hypertrophy - leads to stricture formation
- Creeping fat: mesenteric adipose tissue extends over serosal surface
Ulcerative Colitis:
- Mucosa ranges from slightly red and granular to extensive broad-based ulcers
- Abrupt transition between diseased and uninvolved colon
- Isolated islands of regenerating mucosa bulge into lumen creating pseudopolyps; tips may fuse to form mucosal bridges
- Chronic disease leads to mucosal atrophy with smooth surface lacking normal folds
- Colon wall is NOT thickened, serosal surface is normal, strictures do not occur
- Perforations uncommon - only in severe toxic megacolon
3. Microscopic (Histologic) Features
Crohn Disease:
- Transmural inflammation - full thickness of the bowel wall
- Abundant neutrophils infiltrate and damage crypt epithelium - crypt abscesses
- Noncaseating granulomas present in ~35% of cases (pathognomonic when present)
- Marked lymphoid reaction, fibrosis, and serositis
- Haphazard crypt organization from repeated injury and regeneration
- Submucosal and serosal granulomas may also be present
Ulcerative Colitis:
- Inflammation strictly limited to mucosa and submucosa
- Crypt abscesses and pseudopolyp/pyloric metaplasia
- No granulomas (their presence argues against UC)
- Moderate lymphoid reaction
- Mild to no fibrosis or serositis
- Compare Fig. 17.38D (Crohn, transmural) vs Fig. 17.40C (UC, mucosal only) in Robbins Cotran
4. Pathogenesis Differences
While both share the same general mechanism of dysregulated mucosal immunity (CD4+ T cells, Th1/Th17 activation, TNF, IL-12/IL-23), there are immunologic differences:
- UC: increased mucosal production of the Th2-derived cytokine IL-13; ~75% have p-ANCA antibodies; smoking cessation can trigger onset
- Crohn Disease: more Th1-predominant; ~10% p-ANCA; smoking worsens disease; defective Paneth cell granules and abnormal tight junction barrier function (co-segregates with NOD2 polymorphisms)
5. Complications and Clinical Features
Crohn Disease:
- Abdominal pain, diarrhea (often non-bloody), malabsorption, weight loss
- Fistulae (enterocutaneous, enterovesical, enterovaginal, perianal)
- Strictures and bowel obstruction
- Fecal fat malabsorption (steatorrhea)
- Vitamin B12 malabsorption (terminal ileum involvement)
- Recurs after surgical resection - surgery is NOT curative
Ulcerative Colitis:
- Bloody diarrhea with stringy mucoid material, lower abdominal cramps temporarily relieved by defecation
- Relapsing-remitting course; >50% have clinically mild disease
- Toxic megacolon - a life-threatening complication not seen in Crohn
- Colectomy is curative for intestinal disease (though extraintestinal manifestations may persist)
- Incidence of colectomy has fallen sharply in the past 20 years due to biologics
6. Extraintestinal Manifestations (Shared)
Both can cause: migratory polyarthritis, sacroiliitis, ankylosing spondylitis, uveitis, skin lesions (erythema nodosum, pyoderma gangrenosum). However:
- Primary sclerosing cholangitis (PSC) is strongly associated with UC specifically - affects ~5% of UC patients; conversely, the majority of PSC patients also have UC
7. Malignant Potential
Both carry increased risk for colorectal carcinoma (colitis-associated dysplasia). The risk is proportional to duration and extent of colonic disease. This is classified as a shared feature in the Robbins comparison table.
8. Indeterminate Colitis
Robbins notes that in up to 10% of IBD patients, it is not possible to establish a definitive diagnosis of either condition. These cases (termed "indeterminate colitis") do not involve the small bowel and show continuous colonic disease typical of UC but also have features suggestive of Crohn (patchy histologic disease, family history of Crohn, perianal lesions). Fortunately, medical management overlaps significantly.
Sources: Robbins & Cotran Pathologic Basis of Disease (9780443264528), pp. 744-749 (Table 17.8, Figs. 17.35-17.40); Robbins & Kumar Basic Pathology (9780323790185), pp. 578-582 (Table 13.5)
This is a shared conversation. Sign in to Orris to start your own chat.