Give detailed notes on dacrocystitis with types,, pathophysiology and management
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Searching PubMed
dacryocystitis management treatment
I now have comprehensive information from multiple authoritative textbooks. Let me compile the detailed notes.
Dacryocystitis - Detailed Notes
Definition
Dacryocystitis is inflammation and infection of the lacrimal sac, almost always secondary to obstruction of the nasolacrimal duct. The name comes from Greek: dacryocyst (lacrimal sac) + itis (inflammation).
Relevant Anatomy
The lacrimal drainage system drains tears from the ocular surface:
- Puncta - at the posterior edge of the lid margin, medial one-sixth of each lid
- Canaliculi - 2 mm vertical + 8 mm horizontal; superior and inferior unite (>90%) into a common canaliculus
- Rosenmüller valve - mucosal flap at the junction of the common canaliculus and lacrimal sac; prevents reflux
- Lacrimal sac - 10-12 mm long, lies in the lacrimal fossa between the anterior and posterior lacrimal crests
- Nasolacrimal duct (NLD) - 12-18 mm long, opens into the inferior nasal meatus
- Valve of Hasner - mucosal fold at the distal NLD opening
The lacrimal sac lies below the medial canthal tendon. This is a critical anatomical landmark.
TIP: A mass below the medial canthal tendon = dacryocystitis. A mass above the medial canthal tendon = suspect lacrimal sac tumor.
Classification / Types
1. Acute Dacryocystitis
Clinical features:
- Subacute onset of pain in the medial canthal area
- Epiphora (excessive tearing)
- A very tender, tense red swelling at the medial canthus
- Commonly progresses to abscess formation
- Associated preseptal cellulitis may occur
- Fever, chills
- Mucoid or purulent discharge expressible from the punctum on pressure over the lacrimal sac
Complications if untreated:
- Lacrimal sac abscess
- Preseptal/orbital cellulitis
- Rarely: fistula formation (sac-skin fistula), facial cellulitis
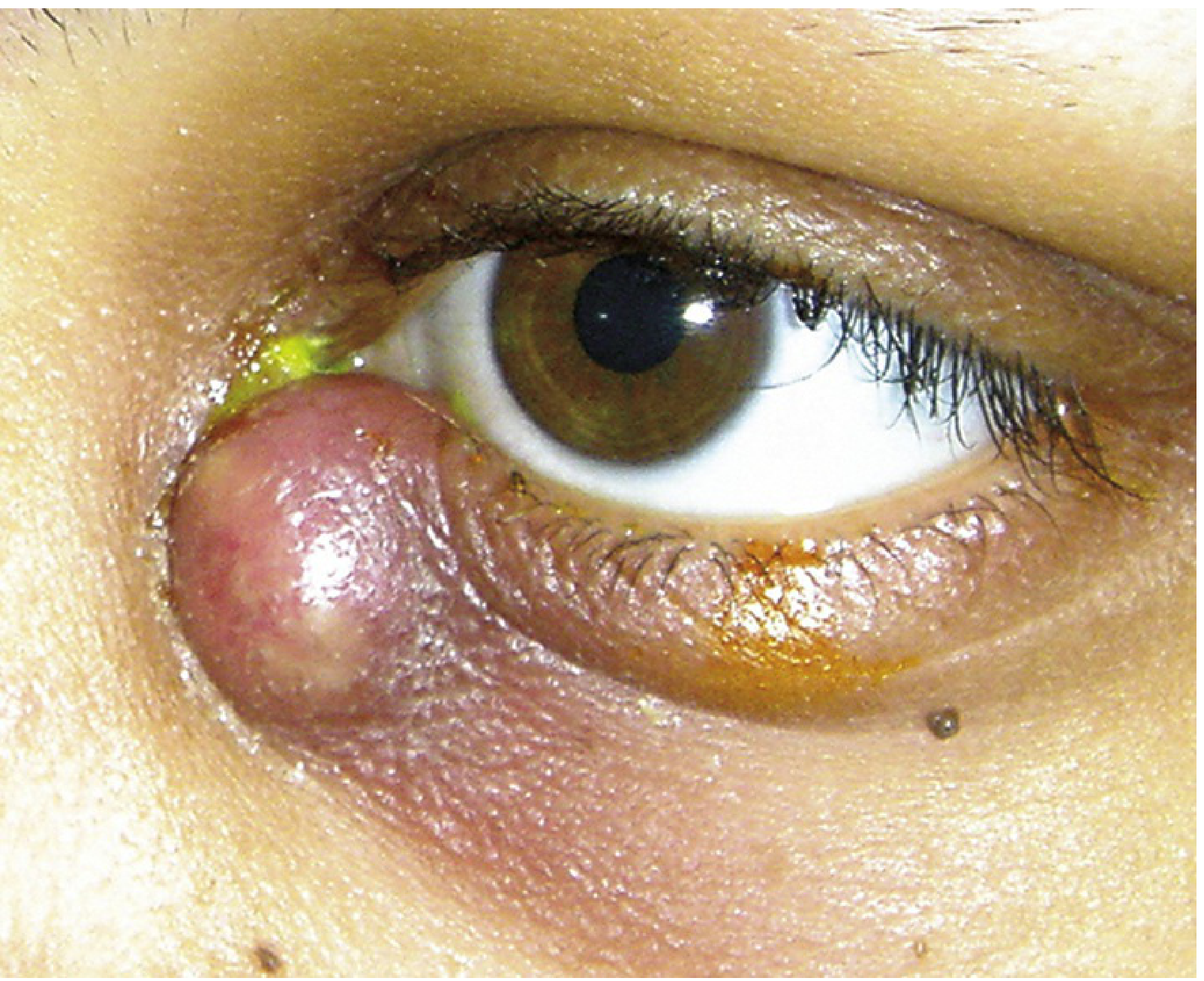
Acute dacryocystitis showing characteristic tense, erythematous swelling below the medial canthal tendon - Wills Eye Manual
2. Chronic Dacryocystitis
Clinical features:
- Chronic epiphora - the dominant symptom
- Chronic or recurrent unilateral conjunctivitis
- A mucocele: painless swelling at the inner canthus (may be absent)
- Pressure over the sac produces mucopurulent canalicular reflux even without obvious swelling
- No acute pain or erythema (unlike acute type)
Silent dacryocystitis: A form of chronic dacryocystitis without obvious clinical signs; detected on careful examination with pressure over the lacrimal sac.
3. Neonatal / Congenital Dacryocystitis
Etiology: Failure of canalization of the nasolacrimal duct at the valve of Hasner (most common - accounts for ~90% of congenital NLD obstruction)
Clinical features:
- Pain, tearing, redness, discharge from birth
- Dacryocystocele: bluish-hued mass at the nasolacrimal region
- May be bilateral (if bilateral, assess for nasal obstruction)
Severity: Can progress to sepsis, meningitis, or death in young infants if untreated

Dacryocystitis in a pediatric patient showing erythema over the lacrimal sac region - Tintinalli's Emergency Medicine
Pathophysiology
The pathophysiologic sequence follows these steps:
1. Nasolacrimal Duct Obstruction
- The primary trigger is obstruction anywhere along the lacrimal drainage system, most commonly at the nasolacrimal duct
- In adults: commonly from primary acquired nasolacrimal duct obstruction (PANDO), often idiopathic, exacerbated by chronic nasal/sinus disease, trauma, neoplasm, or scarring
- In neonates: failure of the valve of Hasner to open (membranous obstruction)
- In children: secondary to viral upper respiratory tract infections causing mucosal edema
2. Stasis of Tear Secretions
- Obstruction causes tears and mucus to pool in the lacrimal sac
- Stagnant secretions create a warm, moist, nutrient-rich environment ideal for bacterial proliferation
3. Bacterial Colonization and Superinfection
- Normal commensal organisms colonize the stagnant mucus
- Common pathogens:
- Streptococcus pneumoniae (most common in adults)
- Staphylococcus aureus and other staphylococci
- Haemophilus influenzae (especially in children)
- MRSA (in nosocomial/resistant cases)
- Streptococcal species
4. Inflammatory Response
- Bacterial infection triggers acute inflammation of the sac wall
- The sac dilates with pus, producing the classic painful swelling
- Surrounding tissues (preseptal) may become involved
5. Abscess / Fistula Formation (if untreated)
- Abscess may point and spontaneously drain through the skin, creating a dacryocystocutaneous fistula
- Infection can spread posteriorly to the orbit (orbital cellulitis) - a sight- and life-threatening complication
Microbiology Summary
| Setting | Common Organisms |
|---|---|
| Adults (acute) | S. pneumoniae, S. aureus, streptococci |
| Children | H. influenzae, S. pneumoniae, S. aureus |
| Neonates | S. pneumoniae, S. aureus |
| MRSA risk | Nosocomial, prior antibiotic exposure, community-acquired MRSA areas |
| Chronic/fungal | Actinomyces, Candida (rare) |
Clinical Evaluation
History:
- Onset, duration, pain, fever, prior episodes (recurrence), nasal disease, trauma, prior ocular surgery
Examination:
- Inspection: Location of swelling (below vs. above medial canthal tendon), extent of erythema
- Pressure test: Apply gentle pressure over the lacrimal sac with a cotton-tipped swab - express discharge from the punctum (positive = confirming dacryocystitis)
- Evaluate for orbital signs: Pupillary response, extraocular motility, proptosis (rule out concurrent orbital cellulitis)
- Gram stain and blood agar culture of expressed discharge. In children: use chocolate agar (for H. influenzae)
- CT scan of orbits and paranasal sinuses: in atypical, severe, or antibiotic-unresponsive cases
Differential Diagnosis
| Condition | Key Differentiating Features |
|---|---|
| Facial/preseptal cellulitis | No discharge expressed from punctum; lacrimal drainage patent on irrigation |
| Acute ethmoid sinusitis | Erythema over nasal bone, medial to inner canthus; imaging diagnostic |
| Frontal sinus mucocele | Swelling above medial canthal tendon; proptosis, downward/lateral displacement |
| Dacryocystocele (neonatal) | Non-inflamed bluish mass at birth; no erythema/discharge |
| Lacrimal sac tumor | Mass above the medial canthal tendon; no acute inflammation |
| Chalazion | Focal inflammatory eyelid nodule; no discharge from punctum |
Management
A. Acute Dacryocystitis
Medical Management
IMPORTANT: Do NOT probe or irrigate the lacrimal system during acute infection (risk of spreading infection)
Mild (afebrile, systemically well):
Adults:
- Cephalexin 500 mg p.o. q6h, OR
- Amoxicillin/clavulanate 500/125 mg t.i.d. or 875/125 mg b.i.d.
- If MRSA suspected: TMP-SMX (double-strength) 160/800 mg p.o. q12h OR Clindamycin 300 mg p.o. t.i.d.
Children (>5 years, <40 kg):
- Amoxicillin/clavulanate 25-45 mg/kg/day p.o. in two divided doses (max 90 mg/kg/day)
- Alternative: Cefpodoxime 10 mg/kg/day in two divided doses (max 400 mg/day)
UK practice (Kanski):
- Flucloxacillin or co-amoxiclav orally
Severe (febrile, systemically unwell, or unreliable patient):
Adults:
- Hospitalize + Cefazolin 1 g i.v. q8h
- Transition to oral antibiotics once clinically improving
- Total course: 10-14 days
Children:
- Hospitalize + Cefuroxime 50 mg/kg IV q8h (up to 100 mg/kg/day)
- OR Cefazolin 33 mg/kg IV q8h
- Penicillin-allergic: Clindamycin 10 mg/kg IV q6h
- MRSA suspected: Vancomycin 10-13 mg/kg IV q6-8h
Adjunct measures:
- Warm compresses to the inner canthal region for 5-10 minutes q.i.d.
- Gentle massage
- Topical antibiotics (e.g., trimethoprim/polymyxin B q.i.d.) - adjunct only, not sufficient alone
- Analgesics (acetaminophen ± codeine) p.r.n.
Surgical Management
-
Incision and Drainage (I&D)
- Indicated when abscess is "pointing" (about to drain spontaneously)
- Risk: persistent sac-skin fistula formation
- Alleviates pain and hastens healing
-
Dacryocystorhinostomy (DCR)
- Creates an anastomosis between the lacrimal sac and nasal mucosa, bypassing the NLD obstruction
- Performed after acute infection has resolved
- Indications: following acute dacryocystitis (to prevent recurrence), chronic dacryocystitis, fistula closure
- Can be performed externally (ext-DCR) or endoscopically (endo-DCR)
- A recent 2025 systematic review confirms external DCR as an evidence-based approach: External DCR - current evidence (PMID 38689455)
B. Chronic Dacryocystitis
- Definitive treatment: Dacryocystorhinostomy (DCR)
- DCR creates a new drainage route from the lacrimal sac to the nasal cavity
- Antibiotic therapy alone is insufficient for chronic disease
- Topical fluoroquinolones may be used as temporizing treatment
C. Congenital / Neonatal Dacryocystitis
Conservative (first-line for most):
- Crigler massage (lacrimal sac massage): compress/massage 4-6 times daily
- Topical antibiotics (e.g., fluoroquinolone drops q.i.d.)
- Approximately 80% resolve spontaneously by 6-12 months of age
Systemic antibiotics: Required for acute stage (febrile/ill neonates)
Probing and irrigation:
- Indicated if conservative management fails, or dacryocystitis persists
- Optimal timing: 6-10 months of age
- Single probing is curative in ~90% of cases before 14 months
- Perform under general anesthesia in infants
Surgical referral: Urgently refer if dacryocystocele is present (may require marsupialization by pediatric otolaryngologist or ophthalmologist)
Key Clinical Pearls
| Pearl | Detail |
|---|---|
| Location of swelling | Always BELOW medial canthal tendon (above = tumor) |
| Never probe acutely | Probing/irrigation during acute infection is contraindicated |
| Endophthalmitis risk | Postpone intraocular surgery if any signs of lacrimal drainage infection |
| Bilateral infant cases | Always assess airway - bilateral nasal obstruction possible |
| Culture discharge | Gram stain + culture to guide therapy; chocolate agar in children |
| MRSA coverage | Consider in community MRSA areas, prior antibiotic failure |
| DCR timing | After acute infection fully resolved |
Summary Flowchart
NLD Obstruction
↓
Stasis of secretions in lacrimal sac
↓
Bacterial colonization (S. pneumoniae, S. aureus, H. influenzae)
↓
Acute Dacryocystitis ←──────────────── Chronic Dacryocystitis
(pain, erythema, swelling, (epiphora, mucocele, recurrent
fever, abscess) conjunctivitis - painless)
↓ ↓
Oral/IV antibiotics + DCR (definitive)
warm compresses
± I&D if pointing abscess
↓
Post-acute: DCR to prevent recurrence
Sources:
- Kanski's Clinical Ophthalmology: A Systematic Approach, 10th ed., pp. 110-111, 125
- The Wills Eye Manual, 8th ed., Section 6.9, pp. 399-402
- Tintinalli's Emergency Medicine: A Comprehensive Study, Section 122
- Textbook of Family Medicine, 9th ed., pp. 349-350
- External DCR systematic review, Locatello et al., Eur J Ophthalmol 2025 (PMID 38689455)
This is a shared conversation. Sign in to Orris to start your own chat.