Carcinoid tumor GIT pathology
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive content from multiple authoritative sources. Let me compile the full detailed answer.
Carcinoid Tumors of the GIT - Pathology
Definition and Nomenclature
Carcinoid tumors (now formally termed neuroendocrine tumors, NETs by the WHO) are neoplasms arising from neuroendocrine cells distributed throughout many organs, particularly the gut and endocrine pancreas. The term "carcinoid" (meaning "carcinoma-like") was coined because these tumors are slower-growing than carcinomas. The current WHO classification uses "low- or intermediate-grade neuroendocrine tumor," reserving "neuroendocrine carcinoma" for high-grade tumors resembling small cell carcinoma.
- Robbins & Kumar Basic Pathology, p. 559
Epidemiology and Distribution
- Most common site: GIT (>40% in the small intestine)
- Second most common: Tracheobronchial tree / lungs
- Peak incidence: Sixth decade, but can occur at any age
- They constitute approximately 50% of all neuroendocrine tumors of the gut and about 5% of all colonic tumors
Cell of Origin
These tumors arise from enterochromaffin (Kultschitzky) cells - the APUD (Amine Precursor Uptake and Decarboxylation) cells of the gut mucosa. These cells are distributed throughout the GIT from stomach to rectum and normally produce vasoactive amines and peptides.
Morphology
Gross Pathology
- Intramural or submucosal masses forming small polypoid lesions
- Yellow or tan in color on cut section
- Elicit an intense desmoplastic reaction that may cause kinking of the bowel and obstruction
- Rarely exceed 3-4 cm at presentation
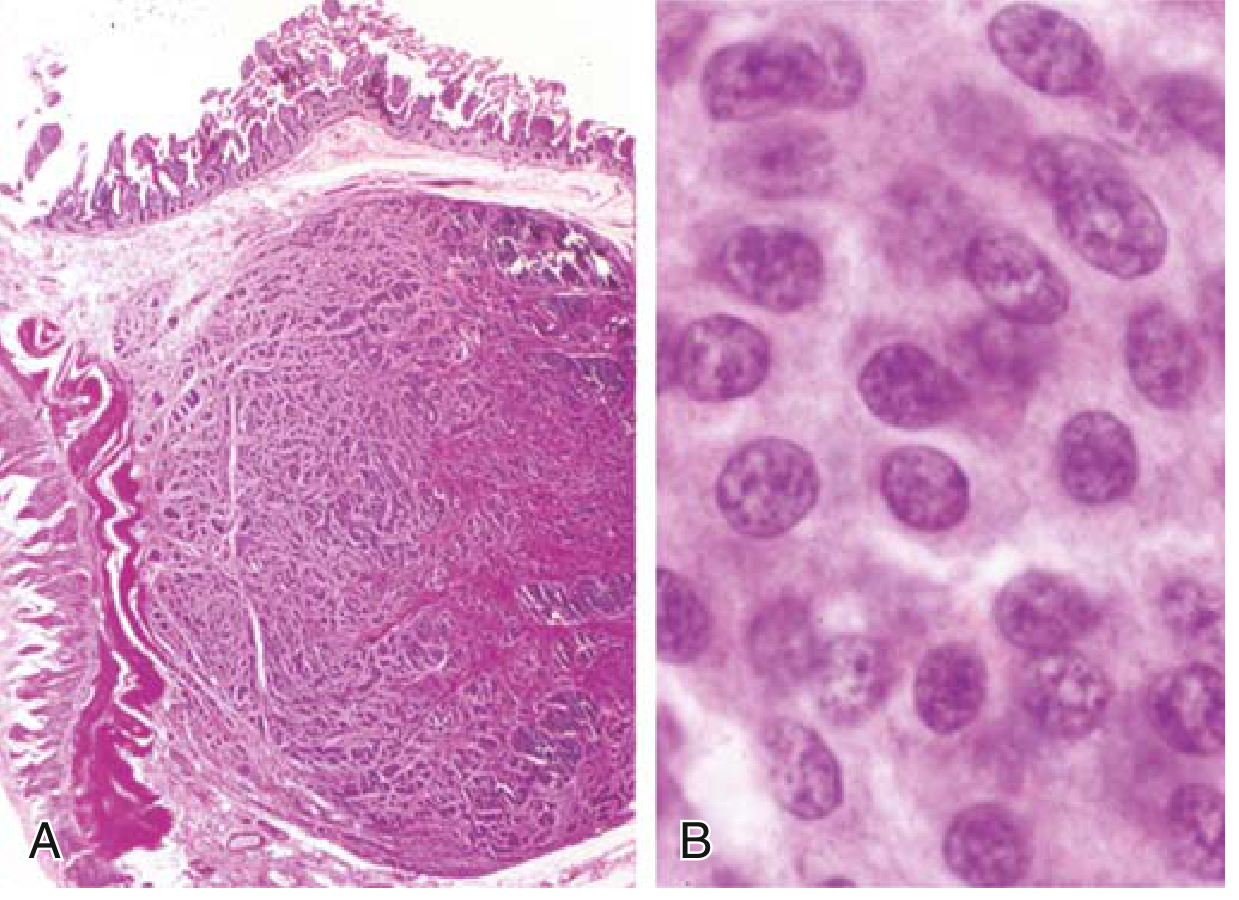
Histological Pathology
-
Composed of islands, trabeculae, strands, glands, or sheets of uniform cells
-
Cells have scant, pink granular cytoplasm and round-to-oval stippled ("salt-and-pepper") nuclei - a hallmark feature
-
Low mitotic activity in low-grade tumors
-
Dense-core neurosecretory granules visible on electron microscopy
-
On electron microscopy: characteristic dense-core granules
-
Robbins & Kumar Basic Pathology, p. 559-560
Classification by Location (Most Important Prognostic Factor)
The most important prognostic factor for GIT neuroendocrine tumors is anatomical location, divided into foregut, midgut, and hindgut:
1. Foregut Tumors (Stomach, Duodenum proximal to Treitz, Esophagus)
- Rarely metastasize
- Generally cured by resection
- Gastric carcinoids may arise in the setting of autoimmune gastritis with hypergastrinemia (hormonal drive causing neuroendocrine cell hyperplasia)
- Rare gastrin-producing foregut tumors (gastrinomas) cause Zollinger-Ellison syndrome - gastroduodenal ulcers, refractory GERD, diarrhea
2. Midgut Tumors (Jejunum and Ileum)
- Most common location overall
- Often multiple
- Tend to be aggressive with greater metastatic potential
- Depth of invasion, size, necrosis, and mitoses correlate with poor prognosis
- Even lesions <1 cm in the midgut have been shown to metastasize - radical resection indicated
3. Hindgut Tumors (Appendix and Colorectum)
-
Appendix:
- Most common overall location for carcinoid (incidental finding in appendectomy specimens ~1%)
- Typically submucosal rubbery masses discovered incidentally
- Almost uniformly benign course
- Lesions <1 cm (95% of cases): appendectomy with negative margins is adequate
- Lesions ≥2 cm: right hemicolectomy recommended
- Carcinoid syndrome is rare (only ~2.9% if hepatic metastases develop)
-
Rectum:
- Tend to produce polypeptide hormones
- Usually discovered when small - metastasis is uncommon
- Present with abdominal pain and weight loss
-
Robbins & Kumar Basic Pathology, p. 560; Schwartz's Principles of Surgery, p. 1366
Immunohistochemistry and Markers
Carcinoid tumors stain positively for:
- Chromogranin A (serum marker - also useful for postoperative surveillance)
- Synaptophysin
- Neuron-specific enolase (NSE)
- Serotonin
- Other peptides: bombesin, calcitonin, substance P
Carcinoid Syndrome
Carcinoid syndrome occurs in <10% of patients (due to liver's first-pass metabolism of vasoactive substances).
Requires: Hepatic metastatic disease (or primary bronchial/retroperitoneal tumor draining outside the portal system).
Mediators
The APUD cells produce: serotonin, histamine, kallikrein, bradykinin, prostaglandins
Clinical Features
| Feature | Details |
|---|---|
| Flushing | Most common (~80%); 5-10 min episodes of facial/truncal erythema |
| Diarrhea | Explosive, watery; due to serotonin release |
| Bronchospasm | Wheezing |
| Carcinoid heart disease | Present in 60-70% of advanced cases; right-sided valvular fibrosis (tricuspid + pulmonary); leads to right heart failure |
| Abdominal cramps | Colicky pain |
Diagnosis
-
24-hour urine 5-HIAA (5-hydroxyindoleacetic acid) - primary stable metabolite of serotonin
-
Plasma Chromogranin A
-
Cross-sectional imaging + somatostatin receptor scintigraphy
-
Maingot's Abdominal Operations, pp. 1985-1987
Malignant Potential and Prognosis
| Location | Size | Metastatic Risk |
|---|---|---|
| Appendix <1 cm | Very low (~2%) | Benign course |
| Appendix 1-2 cm | Intermediate | Controversial |
| Appendix ≥2 cm | Higher | Right hemicolectomy |
| Midgut (any size) | Significant | Radical resection |
| Rectum (small) | Low | Local excision |
| Foregut | Low | Resection curative |
5- and 10-year survival for patients with residual abdominal tumor and hepatic metastases approaches 60%, reflecting the relatively slow growth of these tumors.
Treatment Summary
-
Surgery: First-line for localized disease; debulking/hepatic resection for metastatic disease
-
Hepatic artery embolization / radiofrequency ablation: For widespread hepatic metastases
-
Somatostatin analogues (Octreotide): Palliates carcinoid syndrome in ~90%; inhibits vasoactive peptide release
-
Chemotherapy: Doxorubicin, 5-FU, dacarbazine, interferon-α - response rates ~20%
-
Monitoring: serial 5-HIAA and chromogranin A levels
-
Maingot's Abdominal Operations, pp. 1998-2001; Bailey & Love's Short Practice of Surgery, p. 1411
High-Grade Variant
High-grade neuroendocrine carcinomas (poorly differentiated) resemble small cell carcinoma histologically. In the GIT, these are most common in the jejunum and carry a much worse prognosis.
Sources:
- Robbins & Kumar Basic Pathology, pp. 559-560 (primary pathology reference)
- Maingot's Abdominal Operations, pp. 1983-2001 (carcinoid syndrome)
- Schwartz's Principles of Surgery, p. 1366 (appendiceal carcinoids)
- Bailey & Love's Short Practice of Surgery 28th Ed., p. 1411
Pathogens is morphology
Asking for Preferences
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Excellent - this block has tremendous content. I now have all the information needed for a comprehensive answer. Let me compile the full detailed response.
Pathogens and Their Morphology
A complete guide to the morphological characteristics of the major pathogen groups: bacteria, viruses, fungi, and parasites.
I. BACTERIA
A. General Characteristics
Bacteria are prokaryotes - they lack a membrane-bound nucleus and membrane-enclosed organelles. They are generally 0.5-5 µm in size. Their genome is a single, circular, double-stranded DNA chromosome located in the nucleoid region (not a true nucleus).
Key structures:
- Cell membrane (phospholipid bilayer)
- Cell wall (peptidoglycan - the basis for Gram staining)
- Ribosomes (70S = 50S + 30S subunits)
- No mitochondria - energy generated at cell membrane
B. Basic Bacterial Shapes
| Shape | Term | Examples |
|---|---|---|
| Spherical | Coccus (pl. cocci) | Staphylococcus, Streptococcus, Neisseria |
| Rod-shaped | Bacillus (pl. bacilli) | E. coli, Bacillus, Clostridium, Salmonella |
| Comma-shaped | Vibrio | Vibrio cholerae |
| Spiral, rigid | Spirillum | Helicobacter pylori |
| Spiral, flexible | Spirochete | Treponema pallidum, Borrelia, Leptospira |
| Curved rod | Campylobacter | Campylobacter jejuni |
| Club-shaped | Pleomorphic | Corynebacterium diphtheriae |
C. Arrangement of Cocci
| Arrangement | Description | Example |
|---|---|---|
| Diplococcus | Pairs | Neisseria gonorrhoeae, S. pneumoniae |
| Streptococcus | Chains | Streptococcus pyogenes |
| Tetrad | Groups of 4 | Micrococcus |
| Sarcina | Cuboidal packet of 8 | Sarcina |
| Staphylococcus | Irregular clusters (grapelike) | Staphylococcus aureus |
D. Gram Staining - The Fundamental Classification
The Gram stain divides bacteria based on cell wall composition:
| Feature | Gram-Positive | Gram-Negative |
|---|---|---|
| Color | Purple/violet | Pink/red |
| Cell wall | Thick peptidoglycan (20-80 nm) | Thin peptidoglycan (2-7 nm) + outer membrane |
| Outer membrane | Absent | Present (contains LPS/endotoxin) |
| Teichoic acids | Present | Absent |
| Periplasmic space | Narrow | Wide |
| Toxin type | Exotoxins (mainly) | Endotoxin (LPS) + exotoxins |
Important Gram-positive pathogens:
- Cocci: Staphylococcus aureus, Streptococcus pyogenes, S. pneumoniae, Enterococcus
- Rods/Bacilli: Bacillus anthracis, Clostridium tetani, C. perfringens, C. difficile, Listeria, Corynebacterium diphtheriae
Important Gram-negative pathogens:
- Cocci: Neisseria meningitidis, N. gonorrhoeae
- Rods: E. coli, Klebsiella, Salmonella, Shigella, Pseudomonas, Haemophilus influenzae, Campylobacter, Helicobacter pylori, Vibrio cholerae, Yersinia pestis
E. Special Morphological Features
1. Spore-forming bacteria (endospores - highly resistant structures):
- Bacillus anthracis - central spore
- Clostridium tetani - terminal spore ("drumstick")
- C. perfringens - subterminal spore
- C. botulinum - subterminal spore
2. Capsule-forming bacteria (polysaccharide coat; anti-phagocytic):
- Streptococcus pneumoniae (polysaccharide capsule - visualized by Quellung reaction)
- Klebsiella pneumoniae (mucoid colonies)
- Haemophilus influenzae type b
- Neisseria meningitidis
- Cryptococcus neoformans (fungal - detected by India ink)
3. Flagella (motility):
- Monotrichous - single polar flagellum: Vibrio cholerae, Pseudomonas
- Lophotrichous - tuft at one pole: Helicobacter pylori (multiple at one end)
- Amphitrichous - both poles: Campylobacter
- Peritrichous - all around: E. coli, Salmonella, Listeria
- Non-motile (no flagella): Shigella, Klebsiella, Yersinia pestis
4. Fimbriae/Pili:
- Hair-like protein appendages; shorter and more numerous than flagella
- Function in adhesion to host cells
- Sex pili (F-pili): mediate conjugation (DNA transfer)
- E. coli, Neisseria gonorrhoeae (type IV pili)
F. Acid-Fast Bacteria (Mycobacteria)
Do not Gram stain well due to high mycolic acid content in cell wall. Identified by Ziehl-Neelsen (ZN) stain - appear red against blue background.
| Organism | Disease |
|---|---|
| Mycobacterium tuberculosis | Tuberculosis |
| M. leprae | Leprosy |
| M. avium complex | Opportunistic infection |
Morphology: Slender, beaded rods (~2-4 µm); slow-growing; obligate aerobes; waxy hydrophobic cell wall.
G. Atypical Bacteria (No Cell Wall or Different Structure)
| Organism | Morphology | Key Feature |
|---|---|---|
| Mycoplasma | Pleomorphic (no fixed shape) | No cell wall; smallest free-living organism; resistant to beta-lactams |
| Chlamydia | Obligate intracellular; elementary body (infectious) + reticulate body (replicating) | No peptidoglycan; cannot make own ATP |
| Rickettsia | Small coccobacilli | Obligate intracellular; arthropod-borne |
| Spirochetes | Helical, flexible | 0.1-0.5 µm wide, 5-250 µm long; motility via endoflagella (axial filaments) |
Spirochete morphology details:
- Treponema pallidum (syphilis): very thin, tightly coiled (~8-14 coils), 6-15 µm; cannot be cultured
- Borrelia burgdorferi (Lyme disease): loosely coiled, 10-30 µm; visualized on Giemsa
- Leptospira (leptospirosis): hooked ends, 6-20 µm; "shepherd's crook" shape
II. VIRUSES
A. General Structure
Viruses are non-cellular obligate intracellular parasites. They consist of:
- Nucleic acid core - either DNA or RNA (never both), single- or double-stranded
- Capsid - protein coat surrounding the nucleic acid; made of capsomeres
- Envelope (some viruses) - lipid bilayer derived from host cell membrane; contains viral glycoproteins
Size: Generally 20-300 nm (smaller than bacteria)
B. Capsid Symmetry
| Type | Description | Examples |
|---|---|---|
| Icosahedral | 20 triangular faces; 12 vertices (spherical-appearing) | Adenovirus, Picornavirus, Herpesvirus (inner capsid), Hepatitis B |
| Helical | Capsomeres arranged in a helix around nucleic acid | Rabies, Influenza, RSV, Measles |
| Complex | Neither icosahedral nor helical | Poxviruses (brick-shaped), Bacteriophages |
C. Enveloped vs. Non-Enveloped
| Feature | Enveloped | Non-Enveloped (Naked) |
|---|---|---|
| Structure | Lipid bilayer + glycoproteins | Capsid only |
| Stability | Labile (destroyed by detergents, heat, drying) | More stable in environment |
| Transmission | Requires close contact; respiratory/sexual/blood | Can survive on surfaces; fecal-oral |
| Examples | Herpesvirus, HIV, Influenza, Hepatitis B/C, Rabies, CMV, EBV | Adenovirus, Poliovirus, Hepatitis A, Norovirus, Rotavirus, Parvovirus |
D. DNA vs. RNA Viruses
DNA Viruses (most replicate in nucleus):
| Family | Morphology | Examples |
|---|---|---|
| Herpesviridae | Enveloped icosahedral; 150-200 nm | HSV-1/2, VZV, CMV, EBV, HHV-6/8 |
| Adenoviridae | Non-enveloped icosahedral; 70-90 nm | Adenovirus (pharyngitis, conjunctivitis) |
| Poxviridae | Complex, brick-shaped; 200-400 nm (largest DNA virus) | Smallpox, Vaccinia, Molluscum |
| Hepadnaviridae | Enveloped; partially dsDNA; 42 nm (Dane particle) | Hepatitis B virus |
| Papillomaviridae | Non-enveloped icosahedral; 55 nm | HPV (warts, cervical cancer) |
| Parvoviridae | Non-enveloped icosahedral; 18-26 nm (smallest DNA virus) | Parvovirus B19 |
RNA Viruses:
| Family | Genome | Morphology | Examples |
|---|---|---|---|
| Picornaviridae | +ssRNA | Non-enveloped icosahedral; 28-30 nm | Poliovirus, Rhinovirus, HAV, Enterovirus |
| Flaviviridae | +ssRNA | Enveloped icosahedral; 40-60 nm | HCV, Dengue, Zika, Yellow fever, WNV |
| Togaviridae | +ssRNA | Enveloped icosahedral; 70 nm | Rubella, Chikungunya |
| Coronaviridae | +ssRNA | Enveloped helical; 80-220 nm; crown-like spikes | SARS-CoV-2, MERS-CoV |
| Orthomyxoviridae | -ssRNA (segmented, 8 segments) | Enveloped helical; 80-120 nm; HA + NA surface proteins | Influenza A, B |
| Paramyxoviridae | -ssRNA | Enveloped helical; 150-300 nm | Measles, Mumps, RSV, Parainfluenza |
| Rhabdoviridae | -ssRNA | Enveloped helical; bullet-shaped; 75x180 nm | Rabies virus |
| Retroviridae | +ssRNA (diploid); reverse transcriptase | Enveloped icosahedral; 80-120 nm | HIV-1/2, HTLV |
| Reoviridae | dsRNA (10-12 segments) | Non-enveloped; double-layered icosahedral; 70-80 nm | Rotavirus, Reovirus |
| Bunyaviridae | -ssRNA (3 segments) | Enveloped; 80-120 nm | Hantavirus, Rift Valley fever |
| Filoviridae | -ssRNA | Enveloped helical; long filamentous; up to 14,000 nm | Ebola, Marburg |
HIV (detailed morphology):
- Enveloped, ~120 nm spherical
- Outer envelope: gp120 (binding) + gp41 (fusion) glycoproteins
- Matrix: p17
- Conical capsid: p24 (truncated cone shape - diagnostic on EM)
- Genome: 2 copies of +ssRNA + reverse transcriptase (p66/p51), integrase, protease
III. FUNGI
A. General Morphology
Fungi are eukaryotes with a cell wall made of chitin (not peptidoglycan). They reproduce by spores.
Two basic morphological forms:
| Form | Description | Examples |
|---|---|---|
| Yeast | Unicellular, round/oval; reproduce by budding | Candida, Cryptococcus |
| Mold (Hyphae) | Multicellular; grow as filamentous branching hyphae; network = mycelium | Aspergillus, Rhizopus, dermatophytes |
| Dimorphic | "MOLD in the cold, YEAST in the heat" - mold at 25°C, yeast at 37°C (body temperature) | Histoplasma, Blastomyces, Coccidioides, Paracoccidioides, Sporothrix |
B. Key Fungal Pathogens and Morphology
| Organism | Morphology | Key Feature |
|---|---|---|
| Candida albicans | Oval budding yeast (3-6 µm) + pseudohyphae + germ tubes at 37°C | Germ tube test (+); most common opportunistic fungus |
| Cryptococcus neoformans | Round yeast (4-20 µm) with large polysaccharide capsule | India ink - clear "halo" around organism; urease (+) |
| Aspergillus fumigatus | Septate hyphae with acute angle (45°) branching | V-shaped branching; conidiophore with conidia |
| Mucor/Rhizopus | Broad, non-septate (aseptate) hyphae with wide-angle (90°) branching | "Ribbon-like" hyphae; causes mucormycosis |
| Histoplasma capsulatum | Yeast inside macrophages (2-4 µm); mold phase has tuberculate macroconidia | Bird/bat droppings; Ohio/Mississippi river valleys |
| Blastomyces dermatitidis | Broad-based budding yeast (8-15 µm); thick double-refractile cell wall | "Figure-8" appearance |
| Coccidioides immitis | Spherules (20-60 µm) containing endospores in tissue | Arthroconidia in mold phase; desert Southwest |
| Pneumocystis jirovecii | Cysts (5-8 µm) with 8 intracystic bodies; trophic forms | Stained by GMS (silver) stain; CD4 <200 |
| Sporothrix schenckii | Cigar-shaped yeast in tissue; mold has "rosette" conidia arrangement | "Rose gardener's disease"; lymphocutaneous |
| Dermatophytes | Septate hyphae + macroconidia/microconidia | Trichophyton, Microsporum, Epidermophyton; infect keratinized tissue only |
C. Special Stains for Fungi
- GMS (Gomori Methenamine Silver): Black fungi on green background
- PAS (Periodic Acid-Schiff): Magenta/pink fungi
- India ink: Cryptococcus capsule (negative stain)
- Calcofluor white: Fluorescent staining of chitin
IV. PARASITES
A. Protozoa (Unicellular Eukaryotes)
1. Intestinal Protozoa
| Organism | Morphology | Key Feature |
|---|---|---|
| Entamoeba histolytica | Trophozoite (15-60 µm): motile, pseudopods, ingested RBCs; Cyst (10-20 µm): 4 nuclei | "Flask-shaped" ulcers; amoebic dysentery |
| Giardia lamblia | Trophozoite: pear-shaped, 2 nuclei, 4 pairs of flagella ("falling leaf" motility); Cyst: oval, 4 nuclei | Ventral sucking disk; mountain stream water |
| Cryptosporidium | Oocysts (4-6 µm): very small, acid-fast; 4 sporozoites per oocyst | Acid-fast stain; immunocompromised |
| Balantidium coli | Largest protozoan (50-100 µm); ciliated trophozoite; bean-shaped macronucleus | Only ciliate infecting humans |
2. Blood/Tissue Protozoa
| Organism | Morphology | Key Feature |
|---|---|---|
| Plasmodium falciparum | Ring forms (appliqué/accole); multiple rings per RBC; banana-shaped gametocytes | RBC not enlarged; causes malaria |
| P. vivax/ovale | Ring forms + trophozoites; enlarged RBCs; Schüffner dots | Amoeboid trophozoite |
| P. malariae | Band-form trophozoite; "rosette" schizonts | Normal or small RBCs |
| Trypanosoma brucei | Spindle-shaped trypomastigote (~25 µm); undulating membrane; single flagellum | Sleeping sickness; tsetse fly |
| Trypanosoma cruzi | Trypomastigote with C- or U-shape; "sickle" form; amastigotes in tissue | Chagas disease; reduviid bug |
| Leishmania | Promastigote (flagellated, extracellular) in sandfly; amastigote (non-flagellated, intracellular) in macrophages | Sandfly transmission |
| Toxoplasma gondii | Tachyzoites: crescent/banana-shaped (3x6 µm); bradyzoites in tissue cysts | Definitive host = cat; congenital infection |
3. Vaginal Protozoa
| Trichomonas vaginalis | Pear-shaped, 5 flagella (4 anterior + 1 in undulating membrane); no cyst stage | Jerky "tumbling" motility; STI |
B. Helminths (Worms)
1. Nematodes (Roundworms) - Cylindrical, unsegmented
| Organism | Size/Morphology | Key Feature |
|---|---|---|
| Ascaris lumbricoides | Large (15-35 cm); 3 lips around mouth | Largest intestinal nematode |
| Enterobius vermicularis | Small (1 cm); pointed tail (pinworm) | Scotch tape test; perianal pruritus |
| Trichuris trichiura | Whip-shaped; narrow anterior, thick posterior (whipworm) | Barrel-shaped eggs |
| Hookworms (Ancylostoma/Necator) | Cutting plates (Ancylostoma) or cutting plates with semilunate plates (Necator) | Blood loss; hypochromic anemia |
| Strongyloides stercoralis | Rhabditiform (free-living) vs. filariform (infective) larvae | Autoinfection; filariform larvae in stool |
| Wuchereria bancrofti | Sheathed microfilariae; nocturnal periodicity | Lymphatic filariasis; elephantiasis |
| Loa loa | Sheathed microfilariae; diurnal periodicity | Calabar swellings; eye worm |
| Onchocerca volvulus | Unsheathed microfilariae in skin | River blindness; black fly |
2. Cestodes (Tapeworms) - Flat, segmented
| Organism | Morphology | Key Feature |
|---|---|---|
| Taenia saginata | Unarmed scolex (no hooks); up to 10 m long; >12 uterine branches per proglottid | Beef tapeworm |
| Taenia solium | Armed scolex (hooks + suckers); <7 m; <12 uterine branches per proglottid; cysticerci in tissue | Pork tapeworm; neurocysticercosis |
| Echinococcus granulosus | Small tapeworm (3-6 mm) in dog intestine; hydatid cysts in human liver/lung | Hydatid disease; brood capsules with scolices |
| Diphyllobothrium latum | Broadest tapeworm (up to 15 m); scolex has bothria (grooves, no suckers) | Fish tapeworm; B12 deficiency |
3. Trematodes (Flukes) - Flat, non-segmented, leaf-shaped
| Organism | Morphology | Key Feature |
|---|---|---|
| Schistosoma mansoni | Adult male has gynecophoral canal holding female; eggs with lateral spine | Intestinal schistosomiasis; Africa |
| S. haematobium | Eggs with terminal spine | Urinary schistosomiasis; bladder cancer |
| S. japonicum | Small eggs with rudimentary lateral spine | Most eggs per worm; cerebral disease |
| Clonorchis sinensis | Small (12-20 mm); Chinese liver fluke; flask-shaped eggs with operculum | Bile duct; cholangiocarcinoma |
| Fasciola hepatica | Large (30 mm); sheep liver fluke; large operculated eggs | Liver fluke; biliary obstruction |
| Paragonimus westermani | Lung fluke; reddish-brown, 8-16 mm; operculated eggs | Hemoptysis; raw crab |
C. Ectoparasites
| Organism | Morphology | Key Feature |
|---|---|---|
| Sarcoptes scabiei | Oval mite (0.3-0.4 mm); 4 pairs of legs; burrows in skin | Scabies; intense pruritus |
| Pediculus humanus | Louse with clinging claws; nits attached to hair | Head/body lice |
| Phthirus pubis | Crab louse - short, broad body with crab-like claws | Pubic lice |
Summary: Quick Identification Table
| Pathogen Type | Cell Type | Cell Wall | Size | Unique Feature |
|---|---|---|---|---|
| Gram + bacteria | Prokaryote | Thick peptidoglycan | 0.5-5 µm | Purple on Gram stain |
| Gram - bacteria | Prokaryote | Thin PG + outer membrane (LPS) | 0.5-5 µm | Pink on Gram stain; endotoxin |
| Mycobacteria | Prokaryote | Mycolic acid-rich | 2-4 µm | Acid-fast (ZN stain) |
| Mycoplasma | Prokaryote | None | 0.1-0.3 µm | Smallest free-living organism |
| Viruses | Non-cellular | None (has capsid ± envelope) | 20-400 nm | Obligate intracellular |
| Fungi | Eukaryote | Chitin | 3-30 µm | GMS/PAS staining |
| Protozoa | Eukaryote | None or minimal | 1-100+ µm | Often have cyst + trophozoite stages |
| Helminths | Eukaryote (multicellular) | Cuticle | mm-meters | Eggs/larvae used for identification |
Sources: Jawetz, Melnick & Adelberg's Medical Microbiology, 28th ed. (Fundamentals of Microbiology, pp. 6-140); Medical Microbiology, 9th ed.; Sherris & Ryan's Medical Microbiology, 8th ed.
This is a shared conversation. Sign in to Orris to start your own chat.