Case 3: Presentation: 58-year-old with rapidly progressive perineal pain, erythema, skin necrosis; fever; toxic. Q1. Most important immediate action? Q2. What diagnostic tool is not the priority? 23. Key organisms concept?
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
I have everything needed for a complete, textbook-referenced answer.
Case 3: Fournier Gangrene (Necrotizing Fasciitis of the Perineum)
Diagnosis: This presentation - rapidly progressive perineal pain, erythema with skin necrosis, fever, and a toxic patient - is Fournier Gangrene, a potentially lethal form of necrotizing fasciitis of the perineal/genital/perianal region.
Q1. Most Important Immediate Action
Emergency surgical debridement - taken to the OR immediately.
"FG is a surgical emergency. It is rapidly progressive and quickly leads to sepsis, potentially with multiple organ failure and even death."
- Sabiston Textbook of Surgery, p. 2167
The bedside "finger test" (lack of resistance to blunt probing along fascial planes) confirms the diagnosis intraoperatively. Broad-spectrum IV antibiotics and aggressive fluid resuscitation are started simultaneously, but surgery must not be delayed for any investigation.
The antibiotic regimen should include:
- A beta-lactam/beta-lactamase inhibitor OR carbapenem (for aerobic gram-negatives and anaerobes)
- High-dose penicillin (for streptococci/clostridia)
- Clindamycin (anti-toxin effect, anaerobic coverage)
- Vancomycin added until MRSA is excluded
Re-debridement every 24-48 hours is standard until all necrotic tissue is cleared. Spread is typically far more extensive than external appearance suggests - it can track along fascial planes from the perineum up the anterior abdominal wall to the clavicles.
(Washington Manual of Medical Therapeutics; Campbell-Walsh-Wein Urology)
Q2. Diagnostic Tool That is NOT the Priority
CT scan (or any imaging) is NOT the priority.
The diagnosis is clinical. Waiting for CT before taking the patient to theatre costs lives.
"Diagnosis is clinical. High suspicion should prompt immediate surgical exploration where lack of resistance to probing is diagnostic."
- Washington Manual of Medical Therapeutics, p. 517
Although CT can demonstrate gas in the soft tissues and fascial plane edema, and plain films may also show subcutaneous gas, imaging should never delay surgery in a toxic patient with clinical signs of necrotizing fasciitis. If the clinical picture is clear, the patient goes directly to the OR.
The LRINEC score (Laboratory Risk Indicator for Necrotizing Infection) uses CRP, WBC, Hgb, Na, creatinine, and glucose - but in an overtly toxic patient with skin necrosis, waiting to calculate it adds no value. Individual lab values are described as "largely unhelpful" in distinguishing necrotizing fasciitis from severe cellulitis.
(Sabiston Textbook of Surgery, p. 2167)
Q3. Key Organisms Concept
Fournier Gangrene is characteristically a polymicrobial, synergistic infection (aerobic-anaerobic synergy). This is the core concept.
Two Bacteriological Patterns:
| Pattern | Organisms |
|---|---|
| Type I - Polymicrobial (most common) | Aerobes + anaerobes acting synergistically |
| Type II - Monomicrobial | Group A beta-hemolytic Streptococcus (GABHS) or S. aureus / CA-MRSA |
Typical Polymicrobial Mix:
- Facultative aerobes: E. coli, Klebsiella, Enterococci, Staphylococci
- Anaerobes: Bacteroides, Fusobacterium, Clostridium, microaerophilic Streptococci, Corynebacteria
"Wound cultures generally yield multiple organisms, implicating anaerobic-aerobic synergy. Mixed cultures containing facultative organisms (E. coli, Klebsiella, enterococci) along with anaerobes (Bacteroides, Fusobacterium, Clostridium, microaerophilic streptococci) have been obtained from the lesions."
- Campbell-Walsh-Wein Urology
Mechanism of synergy: The aerobic organisms consume oxygen, creating a hypoxic environment that allows anaerobes to proliferate. Bacterial toxins and enzymes cause microthrombosis of small subcutaneous vessels → ischemia → necrosis → further spread along fascial planes. Gas-forming organisms (e.g., Clostridium) produce the crepitus that is a hallmark sign.
The foul odor characteristic of the condition is a clinical clue to the heavy anaerobic burden.
Clinical Image
Below: (A) Fournier Gangrene showing perineal skin necrosis; (B) Appearance after surgical debridement.
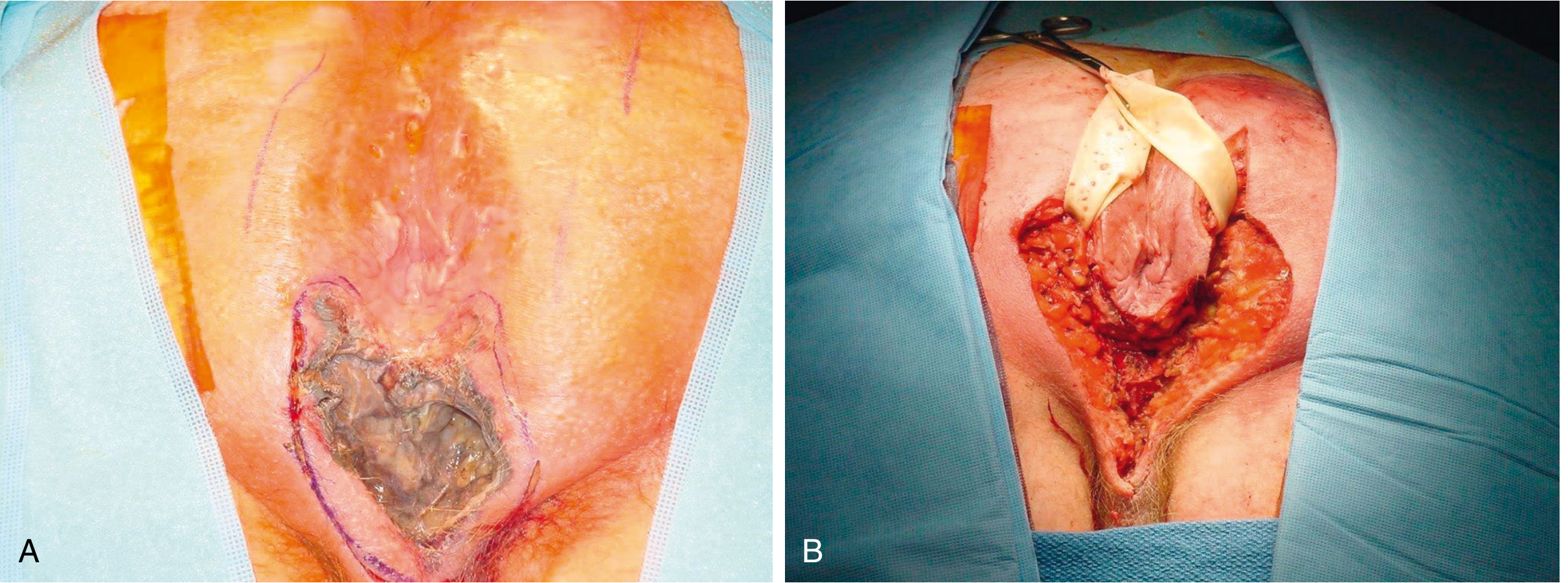
(Sabiston Textbook of Surgery, Fig. 97.22)
Summary Table
| Question | Answer |
|---|---|
| Q1. Most important immediate action | Emergency surgical debridement + IV broad-spectrum antibiotics (do not delay for investigations) |
| Q2. Not the priority diagnostically | CT scan / imaging - diagnosis is clinical; surgery must not wait |
| Q3. Key organisms concept | Polymicrobial aerobic-anaerobic synergy (E. coli, Klebsiella, Enterococci + Bacteroides, Fusobacterium, Clostridium) |
This is a shared conversation. Sign in to Orris to start your own chat.