Everything about ctev
Reading File
Finding Sources
Searching PubMed
"clubfoot" OR "talipes equinovarus" AND treatment
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
Reading File
I now have more than enough comprehensive data to write a thorough response. Let me compile everything.
Congenital Talipes Equinovarus (CTEV) - Complete Overview
Definition
Congenital Talipes Equinovarus (CTEV), or clubfoot, is a complex three-dimensional congenital deformity of the foot and ankle characterized by four components remembered by the mnemonic CAVE:
- C - Cavus (high arch, plantar-flexed first ray)
- A - Adductus (forefoot adduction)
- V - Varus (hindfoot varus)
- E - Equinus (plantarflexion of the ankle)
The deformity ranges from mild and passively correctable to severe with rigid hindfoot equinus and forefoot adduction. It is nearly always accompanied by internal tibial torsion.
Incidence & Epidemiology
- Occurs in approximately 1 in 1,000 live births
- Males affected twice as often as females (2:1 ratio)
- 50% of cases are bilateral; when bilateral, severity and treatment response are highly correlated between feet
- Unilateral cases are evenly distributed between right and left sides
- In unilateral cases, the affected foot is typically one-half to one shoe size smaller in both length and width
- No proven correlation with developmental dysplasia of the hip (DDH)
(Campbell's Operative Orthopaedics 15th Ed; Miller's Review of Orthopaedics 9th Ed)
Etiology
The underlying cause remains largely unknown. Several theories exist:
- Primary germplasm/talar defect: A primary defect in the talus causes continued plantarflexion and inversion, with secondary soft-tissue changes
- Primary neuromuscular defect: Abnormalities in neuromuscular units cause secondary bony changes (abnormal distribution of type I and II muscle fibers documented)
- Vascular cause: Many children with CTEV have a hypoplastic or absent anterior tibial artery; the dorsalis pedis may be the dominant vessel
- Genetic cause: The PITX1-TBX4 transcriptional pathway is strongly implicated. Most cases are idiopathic but familial cases follow autosomal dominant inheritance with incomplete penetrance
Risk factors: Maternal and paternal smoking, maternal obesity, family history, amniocentesis, selective serotonin reuptake inhibitors (SSRIs)
Associated conditions: Arthrogryposis, myelomeningocele, hand anomalies (Streeter dysplasia), diastrophic dwarfism, prune-belly syndrome, tibial hemimelia, and other neuromuscular/syndromic conditions
Pathoanatomy
The core structural abnormality is medial displacement of the navicular and calcaneus around the talus (Turco's description). In 3D terms:
- The calcaneus rotates abnormally in sagittal, coronal, and horizontal planes, pivoting on the interosseous ligament
- The calcaneal tuberosity moves toward the fibular malleolus posteriorly
- The talar neck is deviated medially and plantarward
- The navicular and cuboid are displaced medially
Shortened/contracted structures include:
- Achilles tendon
- Tibialis posterior
- Flexor hallucis longus
- Flexor digitorum longus
- Intrinsic foot muscles
- Joint capsules, ligaments, and plantar fascia
The ankle, midtarsal, and subtalar joints are all involved.
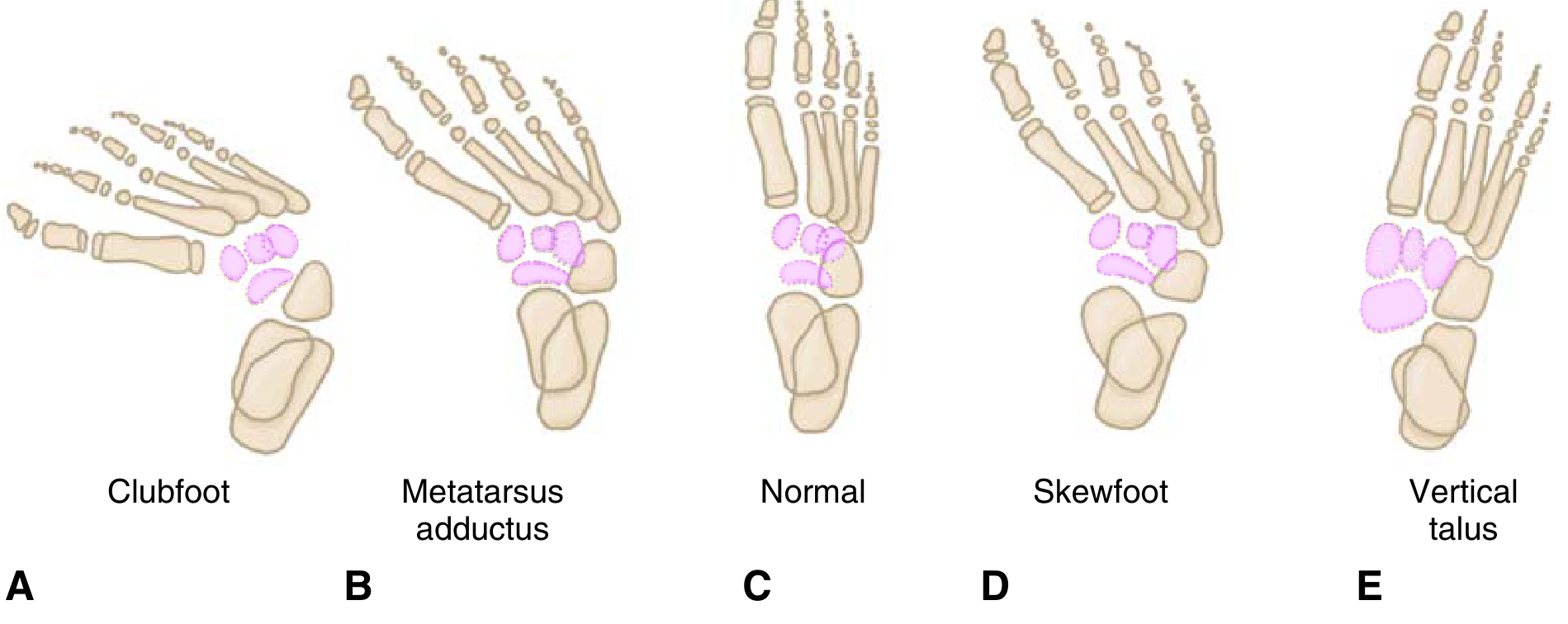
Skeletal AP illustrations comparing Clubfoot, Metatarsus adductus, Normal, Skewfoot, and Vertical talus (Miller's Review of Orthopaedics)
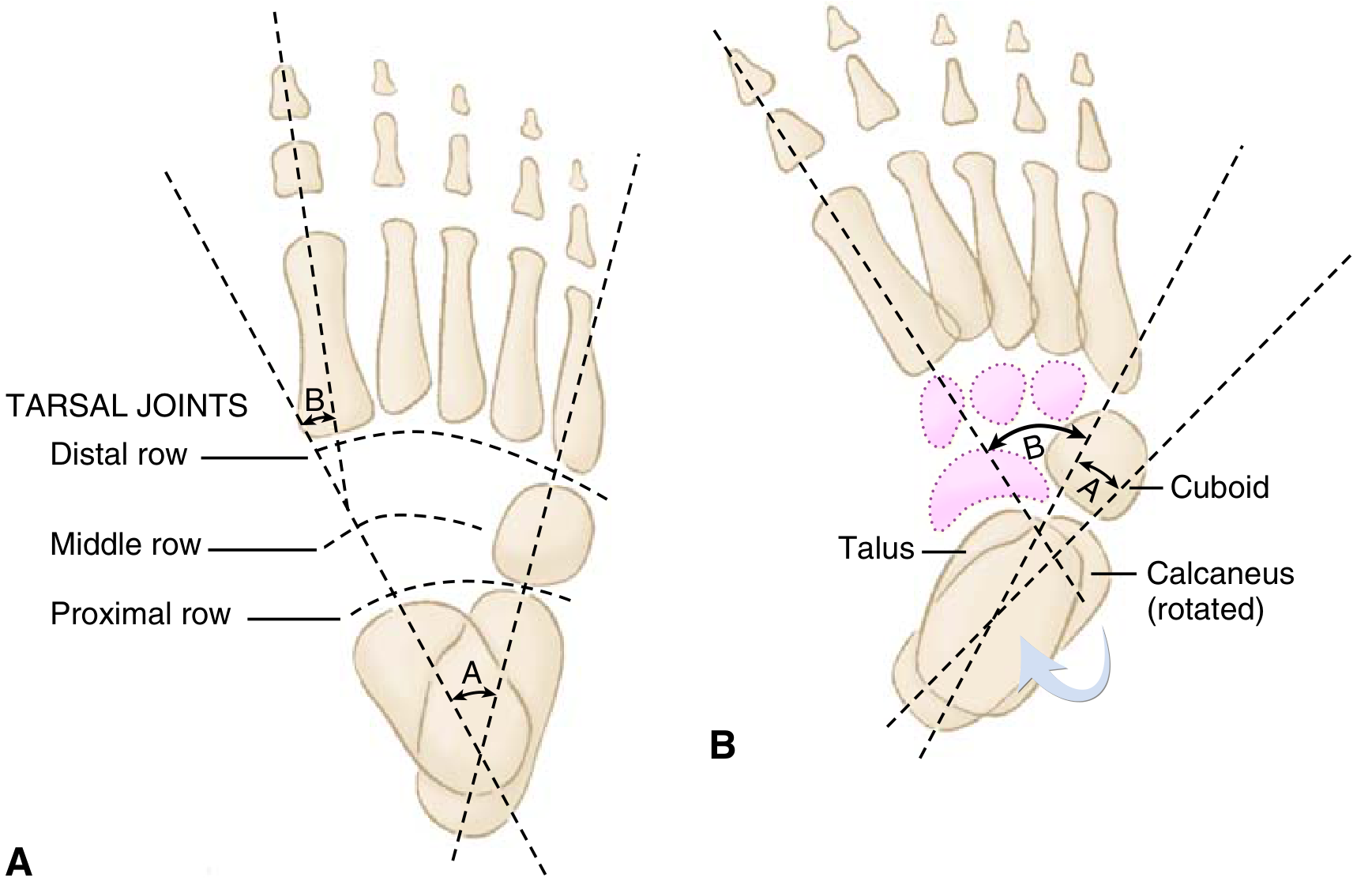
Radiographic evaluation: Normal foot (A) vs Clubfoot (B) - note the "parallelism" of the talus and calcaneus axes (Miller's Review of Orthopaedics)
Classification Systems
1. Pirani Scoring System
Six physical examination findings, split into:
- Hindfoot Contracture Score (posterior crease, empty heel, rigid equinus)
- Midfoot Contracture Score (curved lateral border, medial crease, talar head coverage)
Each component scored: 0 (normal), 0.5 (moderate), 1 (severe)
- Total score: 0-6 (higher = more severe)
- Good interobserver reliability; guides prognosis and number of casts needed
2. Dimeglio Classification
Four parameters assessed by reducibility with gentle manipulation (measured with goniometer):
- Derotation of calcaneopedal block (horizontal plane)
- Adduction of forefoot relative to hindfoot (horizontal plane)
- Varus deviation (frontal plane)
- Equinus (sagittal plane)
One additional point given for each of: posterior skin crease, medial skin crease, rigid cavus, poor muscle condition
Both systems are favored over radiographic classification in infants due to minimal ossification.
Radiographic Evaluation
Radiographs are rarely needed in infants (minimal ossification), but when used:
Anteroposterior (AP) view:
- Talocalcaneal (Kite) angle: normally 20-40°; decreased in CTEV (near 0° or negative)
- Talus-first metatarsal angle: normally 0-20°; negative in CTEV
- Parallelism of the talus and calcaneus axes (lines appear parallel rather than diverging)
Dorsiflexion lateral view (Turco view):
- Talocalcaneal angle: normally ~35°; less than normal in CTEV
- Tibiocalcaneal angle: decreased
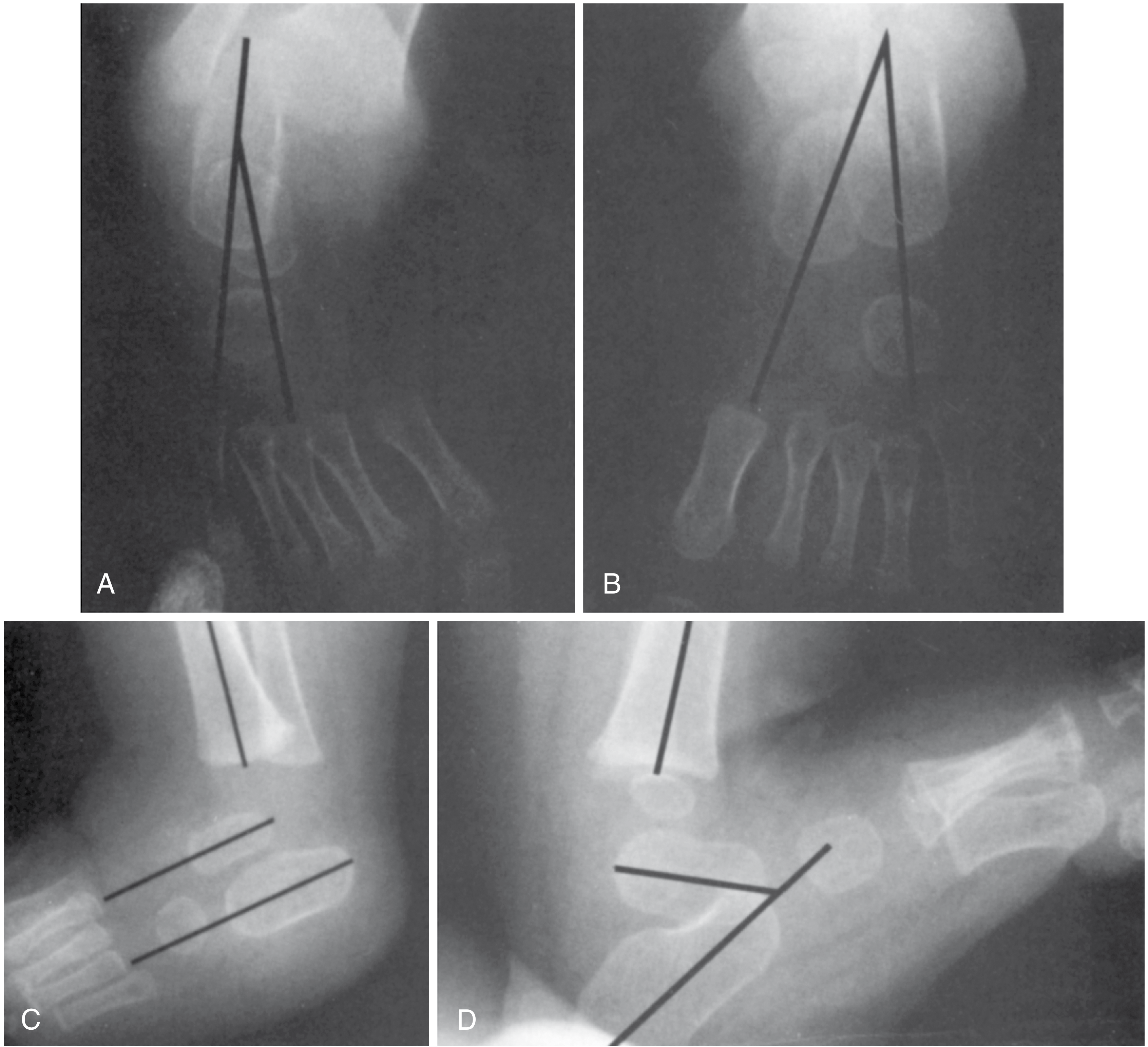
X-rays: (A) AP right clubfoot with decreased talocalcaneal angle and negative talus-first metatarsal angle, (B) Normal left foot AP, (C) Lateral clubfoot with 0° talocalcaneal angle, (D) Normal lateral (Campbell's Operative Orthopaedics)
Treatment
Non-Operative: Ponseti Method (Gold Standard)
The Ponseti method is the first-line treatment for idiopathic clubfoot, achieving correction in ~95% of cases.
Sequence of correction follows CAVE in reverse: Cavus → Adductus → Varus → Equinus
Step-by-step technique:
-
First cast: Corrects cavus by supinating the forefoot and dorsiflexing the first ray. The forefoot is aligned with the heel, outer edge tilted downward due to Achilles tightness. Toe-to-groin long-leg plaster cast.
-
Subsequent casts (weekly): Correct adduction and varus using lateral pressure on the distal talar head as a fulcrum, while foot is abducted around the talar head. Forefoot supination is maintained throughout - pronation must be avoided.
-
Achilles tenotomy: ~90% of patients undergo percutaneous Achilles tendon lengthening at the end of casting to address residual hindfoot equinus. The final cast after tenotomy is placed in 70° abduction and 15° dorsiflexion, maintained for 3 weeks.
-
Foot abduction brace (Denis Browne splint): Essential post-casting step. Worn full-time for 3 months, then during naps and nighttime for 3 years. Brace noncompliance is the strongest predictor of recurrence.
Outcome: No impairment in athletic ability after successful treatment.
Management of Recurrence
- Recurrence is closely tied to brace noncompliance
- Early recurrences: repeat manipulation and casting, possible repeat Achilles tendon lengthening
- Tibialis anterior tendon transfer: Indicated for persistent dynamic supination/supination during swing phase, where there is imbalance between inverters and everters. Transferred laterally (to third cuneiform or cuboid)
- Rate of additional surgical procedures beyond Achilles tenotomy was ~35% in recent studies
Operative Treatment
Reserved for resistant/refractory cases (~5% of idiopathic clubfeet) or failed conservative treatment:
| Procedure | Indication |
|---|---|
| Posteromedial release (PMR) | Resistant/refractory clubfoot; includes tendon lengthening, subtalar, tibiotalar, and talonavicular release and realignment. The posterior tibial artery must be protected. |
| Medial opening-wedge or lateral column-shortening osteotomy / Cuboid decancellation | Older patients (3-10 years) with residual adductus |
| Tibialis anterior tendon transfer | Persistent dynamic supination deformity |
| Triple arthrodesis | Late-presenting children; contraindicated in insensate feet (causes rigidity, leading to ulceration) |
| External fixator (Ilizarov/Taylor Spatial Frame) | Recurrent/neglected clubfoot |
Note: The dorsalis pedis artery is often insufficient alone - protect the posterior tibial artery during all medial releases.
Complications
| Complication | Cause |
|---|---|
| Recurrence | Brace non-compliance (most common cause) |
| Rocker-bottom deformity | Attempted dorsiflexion of hindfoot before varus is corrected |
| Flat-top talus | Aggressive dorsiflexion causing flattening of talar dome |
| Dorsal bunion | Post-clubfoot surgery; due to strong tibialis anterior and flexor hallucis brevis/abductor hallucis; may be iatrogenic if peroneus longus divided. Treated with capsulotomy, FHL lengthening, FHB transfer as MTP extensor |
| Dynamic supination | Occurs in 15-20% after treatment; overpull of anterior tibialis with weak peroneus longus or undercorrected forefoot supination. Treated with tibialis anterior transfer |
| Avascular necrosis of talus | Over-aggressive surgical correction |
| Wound complications | More common with extensive PMR |
Prenatal Diagnosis
Clubfoot can be detected on fetal ultrasound (typically from 18-20 weeks gestation). It is defined as malformation of the fetal ankle producing abnormal foot posturing. Prenatal counseling and preparation of parents for post-natal management is recommended. Detailed fetal anatomical survey and karyotyping may be offered to rule out associated syndromes.
Differential Diagnosis
| Condition | Key Distinguishing Feature |
|---|---|
| Metatarsus adductus | Forefoot adduction with normal hindfoot alignment; passively correctable |
| Positional clubfoot | Passively correctable to neutral; no structural deformity |
| Vertical talus (congenital) | Rocker-bottom foot; talus vertically oriented; dorsal dislocation of navicular |
| Skewfoot (Z-foot) | Adductus with hindfoot valgus and lateral subluxation of navicular |
| Calcaneovalgus | Dorsiflexed and everted foot; opposite of clubfoot |
Key Mnemonics Summary
| Mnemonic | Meaning |
|---|---|
| CAVE | Components: Cavus, Adductus, Varus, Equinus |
| Ponseti correction order | Correct Cavus first, then Adductus + Varus, then Equinus last |
| Pirani score 0-6 | Higher = more severe; 0 = normal, 1 = severe per component |
Recent Evidence (2024-2025)
Recent systematic reviews and meta-analyses confirm:
- The Ponseti method remains effective even for neurogenic clubfoot (myelodysplastic cases) - PMID 41272751, 2025 meta-analysis
- A 2024 network meta-analysis in JBJS identified Ponseti as the optimal treatment for idiopathic clubfoot among all RCT-based interventions - PMID 38015923
- External fixation for recurrent clubfoot shows correction rates but higher complication rates compared to repeat casting - PMID 39932573
- Anterior tibial tendon transfer pull-out fixation vs other fixation methods show comparable outcomes - PMID 39134994
Sources: Campbell's Operative Orthopaedics 15th Ed 2026 | Miller's Review of Orthopaedics 9th Ed | Schwartz's Principles of Surgery 11th Ed | Adams & Victor's Principles of Neurology 12th Ed | Creasy & Resnik's Maternal-Fetal Medicine
This is a shared conversation. Sign in to Orris to start your own chat.