Omeprazole moa adverse effects
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Reading File
I now have comprehensive information from Goodman & Gilman's. Let me compile the full answer.
Omeprazole - Mechanism of Action & Adverse Effects
Classification
Omeprazole is a proton pump inhibitor (PPI) - the most potent class of gastric acid suppressants, capable of reducing daily acid production (basal and stimulated) by 80-95%.
Mechanism of Action
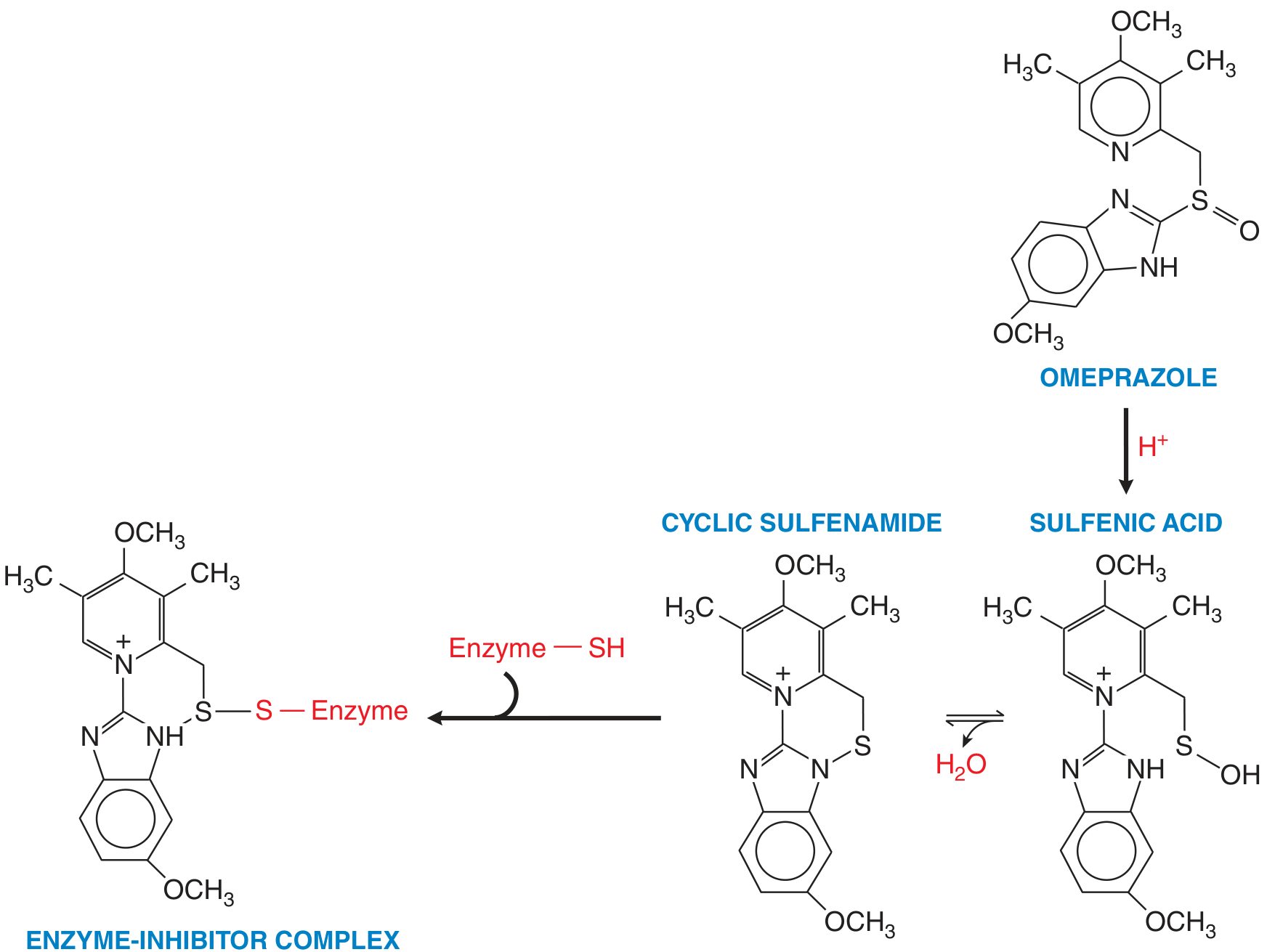
1. Prodrug activation (acid-dependent):
Omeprazole is a weak base prodrug (pKa ~4.0). It is absorbed in the small intestine, enters the systemic circulation, and then accumulates in the acidic secretory canaliculi of gastric parietal cells, where it undergoes protonation and acid-catalyzed conversion to two reactive species:
- Sulfenic acid
- Cyclic sulfenamide
These two forms are in equilibrium with each other in the canalicular lumen.
2. Irreversible covalent binding:
The activated sulfenamide reacts with sulfhydryl (-SH) groups on cysteine residues of the H⁺/K⁺-ATPase (the proton pump), forming a disulfide covalent bond and creating a permanent enzyme-inhibitor complex. This irreversibly inactivates the pump.
3. Target enzyme - H⁺/K⁺-ATPase:
This enzyme (encoded by ATP4A for the catalytic α-subunit, ATP4B for the β-subunit) is responsible for secreting H⁺ into the gastric lumen in exchange for K⁺. It is the final common step in gastric acid secretion, regardless of the stimulus (histamine, gastrin, acetylcholine).
4. Duration of action:
Because the inhibition is irreversible, acid suppression lasts 24-48 hours - until the parietal cell synthesizes new proton pumps. Since not all pumps are active simultaneously, maximal inhibition (~70% at steady state) takes 2-5 days of once-daily dosing.
Key pharmacokinetic note: PPIs must be taken before meals (30-60 min), so they are absorbed and reach parietal cells just as pumps are being activated by food.
Adverse Effects
Common (GI and general)
- Headache
- Nausea
- Abdominal pain
- Constipation or diarrhea
- Flatulence
Drug interactions (CYP450 metabolism)
Omeprazole is metabolized by hepatic CYPs (primarily CYP2C19) and can interfere with:
- Warfarin - increased anticoagulant effect
- Diazepam - reduced clearance
- Clopidogrel - reduced antiplatelet activation (clinically important)
- Atazanavir/nelfinavir - reduced antiretroviral absorption due to raised gastric pH
- Ketoconazole, ampicillin esters, iron salts - reduced bioavailability in less acidic environment
Long-term / chronic use effects
| Effect | Mechanism |
|---|---|
| Hypomagnesemia | Unknown; not via renal wasting. Monitor Mg²⁺ in long-term users, especially those on diuretics |
| Vitamin B12 deficiency | Reduced acid impairs intrinsic factor release and B12 absorption; check levels in long-term/high-dose users |
| Hypergastrinemia | Reduced acid → loss of negative feedback → elevated gastrin. Leads to ECL cell hyperplasia, fundic gland polyposis, atrophic gastritis |
| Rebound acid hypersecretion | On stopping PPIs, elevated gastrin drives surge in acid secretion |
| Bone fractures | Reduced Ca²⁺ and Mg²⁺ absorption; risk increases with high-dose, long-term use |
| Infection susceptibility | Reduced gastric acidity impairs the acid barrier: increased risk of C. difficile, community-acquired pneumonia, spontaneous bacterial peritonitis (in cirrhosis) |
| Small intestinal bacterial overgrowth (SIBO) | Gastric acid normally limits bacterial colonization of the upper GI tract |
Rare/reported effects
- Subacute myopathy
- Arthralgias
- Interstitial nephritis
- Pharyngitis
- Skin rashes
Special populations
- Hepatic disease: Dose reduction needed for esomeprazole and lansoprazole (substantially reduced clearance). Omeprazole itself has moderately prolonged half-life in severe liver disease.
- Pregnancy: Category C; use only if clearly needed.
- Renal failure: No dose adjustment needed with standard dosing.
Sources: Goodman & Gilman's The Pharmacological Basis of Therapeutics, Chapter 53; Harrison's Principles of Internal Medicine 22E; Yamada's Textbook of Gastroenterology 7E.
This is a shared conversation. Sign in to Orris to start your own chat.