Give me details regarding normal pressure hydrocephalus from latest textbook of harrison principal medicine
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
I have all the content I need from Harrison's 22nd Edition about NPH. Let me now compile the full answer. The key NPH content was in lines 1268-1275 of block 49 and lines 1596-1597 of block 3. I have everything needed.
Here is a comprehensive presentation of Normal Pressure Hydrocephalus from Harrison's Principles of Internal Medicine, 22nd Edition (2025):
Normal Pressure Hydrocephalus (NPH)
Source: Harrison's Principles of Internal Medicine, 22nd Edition (2025, McGraw Hill)
Overview
NPH is described by Harrison's as "a relatively uncommon but treatable syndrome." The clinical, physiologic, and neuroimaging characteristics must be carefully distinguished from other dementias associated with gait impairment. Historically, many patients treated for NPH have actually suffered from other dementias - particularly Alzheimer's disease (AD), vascular dementia, DLB, and PSP.
Classic Clinical Triad
Harrison's specifies three core features:
- Abnormal gait - ataxic or apractic in character
- Dementia - usually mild to moderate, with emphasis on executive impairment
- Urinary urgency or incontinence
However, the book also notes that "other features of the diagnostic triad (mental changes, incontinence) may be absent in a substantial number of patients," particularly in the gait-dominated presentation.
Gait Characteristics
Harrison's describes the gait disorder under the heading "Frontal Gait Disorder":
- Wide base of support
- Short stride
- Shuffling along the floor
- Difficulty with starts and turns
- Hesitant initiation ("slipping clutch" syndrome or gait ignition failure)
- Described also as "lower-body parkinsonism"
The table in Harrison's comparing gait patterns shows NPH/frontal gait as: wide-based, very slow velocity, short and shuffling stride, hesitant initiation, hesitant and multistep turns.
Neuroimaging Findings
MRI demonstrates:
- Enlarged lateral ventricles (hydrocephaly) with little or no cortical atrophy
- Enlarged flow void about the aqueduct of Sylvius
- Periventricular white matter change
- High-convexity tightness - disproportionate widening of the sylvian fissures versus cortical sulci (so-called "boxcarring," which can be mistaken for perisylvian atrophy)
- Crowding of dorsal frontal-parietal gyri - this helps distinguish NPH from PSP and CBD, where dorsal atrophy with sulcal widening is common
NPH is a communicating hydrocephalus with a patent aqueduct of Sylvius, in contrast to aqueductal stenosis where the aqueduct is small.
MRI Images from Harrison's 22E
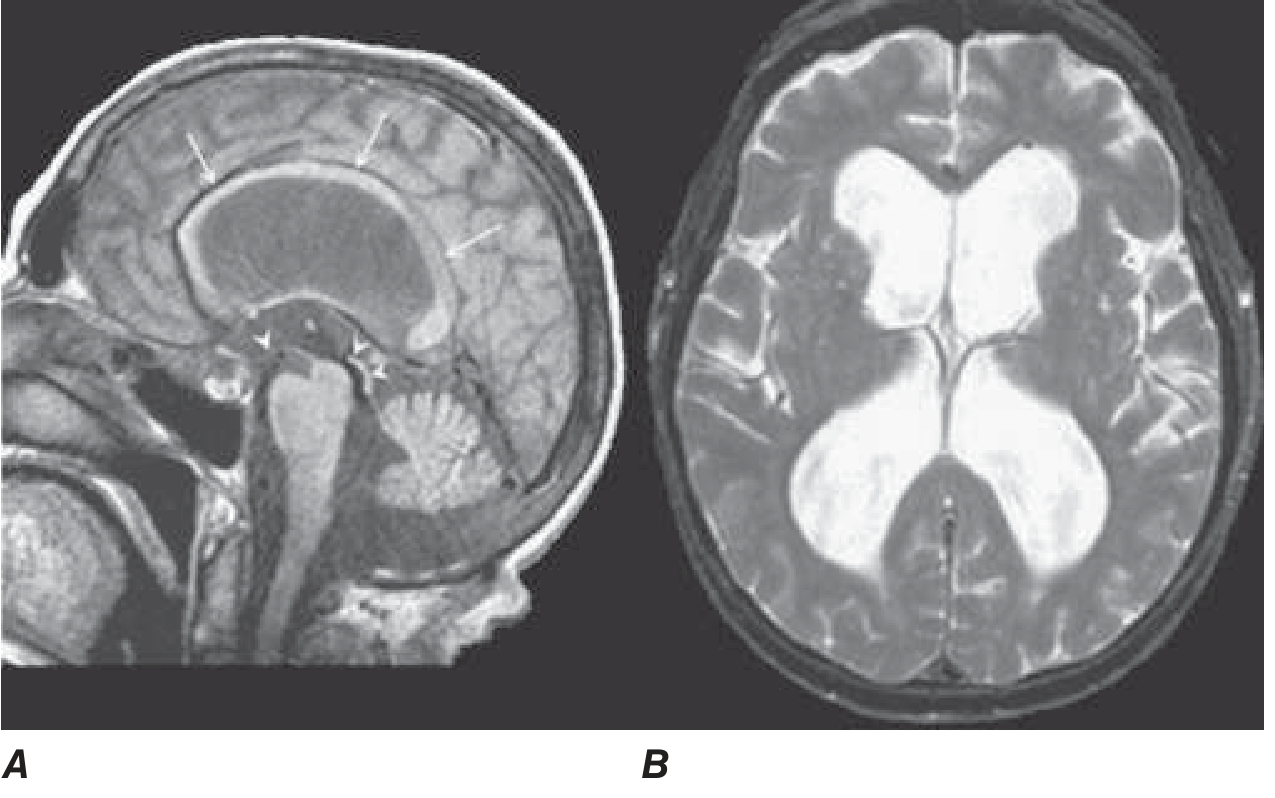
FIGURE 31-3 - Normal-pressure hydrocephalus.
- A (Sagittal T1-weighted MRI): Demonstrates dilation of the lateral ventricle and stretching of the corpus callosum (arrows), depression of the floor of the third ventricle (single arrowhead), and enlargement of the aqueduct (double arrowheads). Note diffuse dilation of lateral, third, and fourth ventricles with a patent aqueduct - typical of communicating hydrocephalus.
- B (Axial T2-weighted MRI): Demonstrates dilation of the lateral ventricles. This patient underwent successful ventriculoperitoneal shunting.
CSF Findings
- Lumbar puncture opening pressure falls in the high-normal range
- CSF protein, glucose, and cell counts are normal
Pathophysiology
The exact mechanism remains unclear, but Harrison's explains:
- NPH is caused by obstruction to normal CSF flow over the cerebral convexities and delayed resorption into the venous system
- The indolent nature of the process results in enlarged lateral ventricles with relatively little increase in CSF pressure (hence "normal pressure")
- Presumed edema, stretching, and distortion of subfrontal white matter tracts lead to clinical symptoms
Etiology / Risk Factors
Some patients give a history of conditions producing meningeal scarring that block CSF resorption:
- Previous meningitis
- Subarachnoid hemorrhage
- Head trauma
Others with longstanding but asymptomatic congenital hydrocephalus may have adult-onset deterioration in gait or memory that mimics NPH.
Diagnosis
Harrison's emphasizes:
- A lumbar puncture or dynamic test is necessary to confirm NPH
- Numerous attempts to improve NPH diagnosis with special studies have been made, including radionuclide cisternography (showing delay in CSF absorption over the convexity) and various CSF monitoring protocols
- The main purpose of structural imaging is to exclude other disorders such as neoplasms, vascular dementia, diffuse white matter disease, and NPH itself
Treatment
Ventricular (ventriculoperitoneal) shunting is the primary treatment:
- 30-50% of patients carefully diagnosed with NPH will improve with ventricular shunting
- Gait may improve more than cognition
- Many reported failures to improve cognitively may have resulted from comorbid AD
- The presence of NPH is listed under "reversible causes" of dementia, alongside hypothyroidism, B12 deficiency, and subdural hematoma
Harrison's treatment chapter states: "Treatment of underlying causes includes... ventricular shunting for NPH."
NPH as a Reversible Dementia
Harrison's Table 3-3 (Evaluation of the Patient with Dementia) explicitly lists NPH under Reversible Causes alongside:
- Hypothyroidism
- Thiamine deficiency
- Vitamin B12 deficiency
- Subdural hematoma
- Chronic infection
- Brain tumor
- Drug intoxication
- Autoimmune encephalopathy
Key Differential Diagnoses
Per Harrison's, NPH must be distinguished from:
- AD - prominent memory loss, cortical atrophy
- Vascular dementia - stepwise progression, risk factors
- DLB - early visual hallucinations, parkinsonism
- PSP and CBD - dorsal atrophy, sulcal widening (unlike NPH's frontal-parietal crowding)
- Subcortical vascular dementia - most common cause of frontal gait disorder; NPH is an important differential
Source: Harrison's Principles of Internal Medicine, 22nd Edition (2025), Chapter 31 (Dementia) and Chapter 26 (Gait Disorders), McGraw Hill Medical. - Harrison's 22E, pp. 239-242 and p. 3526
This is a shared conversation. Sign in to Orris to start your own chat.