Acute inflammation
Reading File
Finding Sources
Searching PubMed
"acute inflammation" mechanisms mediators
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive content to write a detailed, well-structured answer on acute inflammation. Let me compose the full response.
Acute Inflammation
Acute inflammation is the rapid, stereotyped response of vascularized tissues to infections and tissue damage. It brings cells and molecules of host defense from the circulation to the site of injury, with the goal of eliminating the offending agent. The response is short-lived (minutes to days) and is dominated by fluid exudation and neutrophil emigration.
Cardinal Signs (Celsus + Virchow)
| Sign | Latin | Mechanism |
|---|---|---|
| Redness | Rubor | Vasodilation → increased blood flow |
| Warmth | Calor | Increased blood flow |
| Swelling | Tumor | Fluid exudation (edema) |
| Pain | Dolor | Prostaglandins, bradykinin, neuropeptides |
| Loss of function | Functio laesa | Pain + tissue damage |
Three Major Components
Acute inflammation has three major components:
- Dilation of small vessels - leading to increased blood flow
- Increased vascular permeability - enabling plasma proteins and leukocytes to leave the circulation
- Emigration and activation of leukocytes - to accumulate at the focus of injury and eliminate the offending agent
Most of these changes occur in postcapillary venules, whose walls are reactive to stimuli and thin enough to allow passage of fluid and proteins.
Vascular Reactions
Changes in Vascular Flow and Caliber
-
Vasodilation - Earliest manifestation. Induced chiefly by histamine acting on vascular smooth muscle of postcapillary venules. Causes redness (rubor) and warmth (calor).
-
Increased vascular permeability - Quickly follows vasodilation. The principal mechanism is contraction of endothelial cells, creating interendothelial openings. Elicited by histamine, bradykinin, and leukotrienes. Occurs within 15-30 minutes and is usually short-lived. In severe injury (burns), direct endothelial damage causes immediate, sustained leakage.
-
Stasis - Loss of fluid and increased vessel diameter slow blood flow. Red cells concentrate in small vessels, increasing viscosity → vascular congestion.
-
Margination and adhesion - With stasis, leukocytes (mainly neutrophils) accumulate along the endothelium, adhere to upregulated adhesion molecules, and migrate into tissue.
Key Terms
- Exudate: Extravascular fluid with high protein concentration and cellular debris - implies increased vascular permeability (inflammation)
- Transudate: Fluid with low protein content (mostly albumin), essentially an ultrafiltrate - osmotic/hydrostatic imbalance without inflammation
- Edema: Excess fluid in interstitial tissue or serous cavities (can be exudate or transudate)
- Pus: Purulent exudate rich in neutrophils, dead cell debris, and microbes
Leukocyte Recruitment
Leukocyte recruitment is a multistep process involving three sequential phases:
Step 1: Rolling (Selectins)
- Loose, reversible attachment to endothelium
- Mediated by selectins (E-selectin, P-selectin on endothelium; L-selectin on leukocytes) binding to carbohydrate ligands
- TNF and IL-1 upregulate selectin expression on endothelium
Step 2: Firm Adhesion (Integrins)
- Stable adhesion mediated by integrins on leukocytes (e.g., LFA-1, Mac-1) binding to ICAM-1 on endothelium
- Chemokines increase integrin avidity (affinity state change via inside-out signaling)
Step 3: Transmigration (Diapedesis)
- Leukocytes migrate through interendothelial junctions (mainly at postcapillary venules)
- CD31 (PECAM-1) plays a key role in this crossing
Step 4: Chemotaxis
- Directed migration toward the injury site along a chemical gradient
- Major chemotactic agents: C5a, IL-8 (CXCL8), leukotriene B4 (LTB4), bacterial products (fMLP)
Neutrophils vs. Macrophages
| Feature | Neutrophils | Macrophages |
|---|---|---|
| Origin | Bone marrow HSCs | Blood monocytes / tissue-resident |
| Lifespan in tissues | Several days | Days to years |
| Response | Rapid, short-lived; degranulation | Slower, prolonged; gene transcription |
| ROS production | Prominent (respiratory burst) | Less prominent |
| Nitric oxide | Low/absent | iNOS-derived |
Neutrophils predominate in early acute inflammation (first 6-24 h); monocytes/macrophages dominate later (24-48 h onwards).
Phagocytosis and Killing
Phagocytosis - Three Steps
- Recognition and attachment - facilitated by opsonins (IgG Fc, C3b) binding to specific leukocyte receptors
- Engulfment - pseudopods extend around the particle, forming a phagosome
- Killing and degradation - phagosome fuses with lysosome → phagolysosome
Intracellular Killing
- Reactive oxygen species (ROS): NADPH oxidase generates superoxide → H₂O₂ → hypochlorous acid (HOCl) via myeloperoxidase (MPO). This is the "respiratory burst."
- Nitric oxide (NO): Generated by iNOS in macrophages; reacts with superoxide to form peroxynitrite (ONOO⁻)
- Lysosomal enzymes: Elastase, collagenase, cathepsins - active at acid pH
Neutrophil Extracellular Traps (NETs)
- Extruded chromatin meshworks containing histones and antimicrobial proteins (elastase, MPO)
- Trap and kill microbes extracellularly
- Also contribute to tissue injury and thrombosis
Mediators of Inflammation
Mediators are either cell-derived (released rapidly from granules or synthesized de novo) or plasma-derived (synthesized in liver, circulate as inactive precursors).
| Mediator | Source | Main Actions |
|---|---|---|
| Histamine | Mast cells, basophils, platelets | Vasodilation, ↑ vascular permeability (via H1 receptor), endothelial activation |
| Prostaglandins (PGE₂, PGI₂) | Mast cells, leukocytes | Vasodilation, pain, fever |
| Leukotrienes (LTB4, LTC4/D4/E4) | Mast cells, leukocytes | LTB4: chemotaxis; LTC4/D4/E4: bronchoconstriction, ↑ permeability |
| PAF | Many cell types | Platelet aggregation, vasoconstriction/vasodilation, ↑ permeability |
| TNF and IL-1 | Macrophages, mast cells | Endothelial activation (adhesion molecules), fever, acute-phase response |
| IL-6 | Many cells | Fever, acute-phase protein synthesis |
| Chemokines (IL-8/CXCL8) | Macrophages, endothelium | Leukocyte recruitment, chemotaxis |
| C3a, C5a | Complement cascade | Mast cell degranulation (anaphylatoxins), C5a is potent chemotactic agent |
| C3b | Complement | Opsonization |
| Bradykinin | Plasma (via kallikrein) | ↑ Permeability, pain, vasodilation |
| Nitric oxide | Endothelium, macrophages | Vasodilation, microbicidal |
Arachidonic Acid Pathway (Key for Pharmacology)
- COX pathway → Prostaglandins and thromboxanes - blocked by NSAIDs (aspirin, ibuprofen)
- Lipoxygenase pathway → Leukotrienes - blocked by zileuton (5-LOX inhibitor) and montelukast (LT receptor antagonist)
- Phospholipase A₂ (releases AA from membrane) - blocked by corticosteroids (via lipocortin/annexin-1)
Complement System
Three activation pathways all converge on C3 convertase:
- Classical pathway: Antigen-antibody complexes → C1 activation
- Alternative pathway: Microbial surface molecules directly activate C3
- Lectin pathway: Mannose-binding lectin (MBL) binds microbial carbohydrates
C3 convertase cleaves C3 → C3a + C3b → C5 convertase → C5a + C5b → MAC (C5b-9)
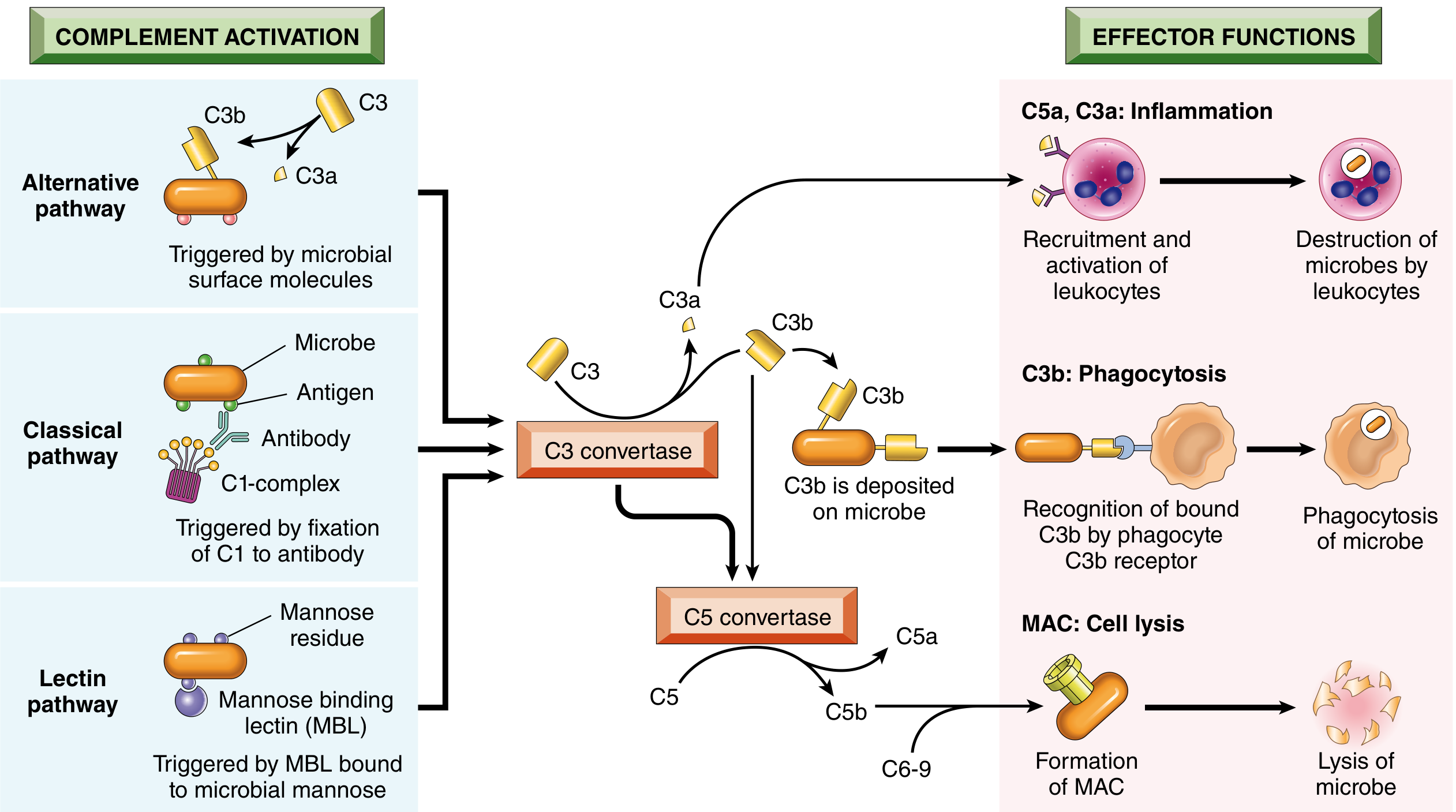
Functions of complement:
- C3a, C5a: Anaphylatoxins - stimulate mast cell degranulation, increase vascular permeability, vasodilation
- C5a: Potent neutrophil/monocyte chemotactic agent
- C3b: Opsonin - promotes phagocytosis
- MAC (C5b-9): Cell lysis (important for thin-walled organisms like Neisseria)
Morphologic Patterns of Acute Inflammation
1. Serous Inflammation
- Outpouring of watery, serum-like fluid into body cavities or spaces created by cell injury
- Few cells, no microbes
- Example: skin blister (burn/viral), pleural/pericardial effusion
2. Fibrinous Inflammation
- Greater vascular permeability allows fibrinogen to escape → fibrin deposited in extracellular space
- Characteristic of inflammation in body cavity linings
- Example: fibrinous pericarditis ("bread and butter" pericarditis), fibrinous pleuritis
- May undergo resolution (fibrinolysis) or organization (fibrosis → adhesions)
3. Purulent (Suppurative) Inflammation
- Formation of pus - neutrophils, liquefactive necrosis debris, microbes
- Caused mainly by pyogenic bacteria (S. aureus, Streptococcus)
- Abscess: Localized collection of pus surrounded by a wall of inflammatory tissue
- Example: staphylococcal abscess, brain abscess
4. Ulcer
- A discontinuity in the epithelium with underlying acute and chronic inflammation
- Example: peptic ulcer, pressure sore, diabetic foot ulcer
Termination of Acute Inflammation
The response subsides as the initiating stimulus is removed because:
- Mediators are short-lived (quickly decay, inactivated by enzymes, or scavenged)
- Neutrophils are short-lived and undergo apoptosis
- Anti-inflammatory substances are activated (lipoxins, IL-10, TGF-β, resolvins/protectins from omega-3 FAs)
Outcomes of Acute Inflammation
| Outcome | Conditions | Description |
|---|---|---|
| Resolution | Minimal injury, short-lived stimulus | Complete restoration of normal tissue architecture |
| Suppuration (abscess) | Pyogenic organisms | Pus formation; may require drainage |
| Healing by fibrosis (scarring) | Extensive tissue destruction; non-regenerative tissues | Collagen deposition replaces damaged tissue |
| Progression to chronic inflammation | Persistent stimulus (e.g., mycobacteria, foreign bodies, autoimmune disease) | Continued inflammation with macrophages, lymphocytes, fibroblasts |
Summary Box
Acute inflammation = vascular dilation + increased permeability + leukocyte emigration (mainly neutrophils). Orchestrated by cell-derived (histamine, leukotrienes, prostaglandins, cytokines) and plasma-derived (complement, kinins) mediators. The cardinal signs (rubor, calor, tumor, dolor, functio laesa) arise from these vascular and cellular events. Resolution restores normal tissue; failure to eliminate the cause leads to abscess, scarring, or chronic inflammation.
Sources: Robbins, Cotran & Kumar - Pathologic Basis of Disease (10e), Ch. 3; Robbins & Kumar - Basic Pathology (11e), Ch. 2
Phagocytosis and clearance of offending agent
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
I now have everything needed for a thorough, detailed answer. Let me compile it.
Phagocytosis and Clearance of the Offending Agent
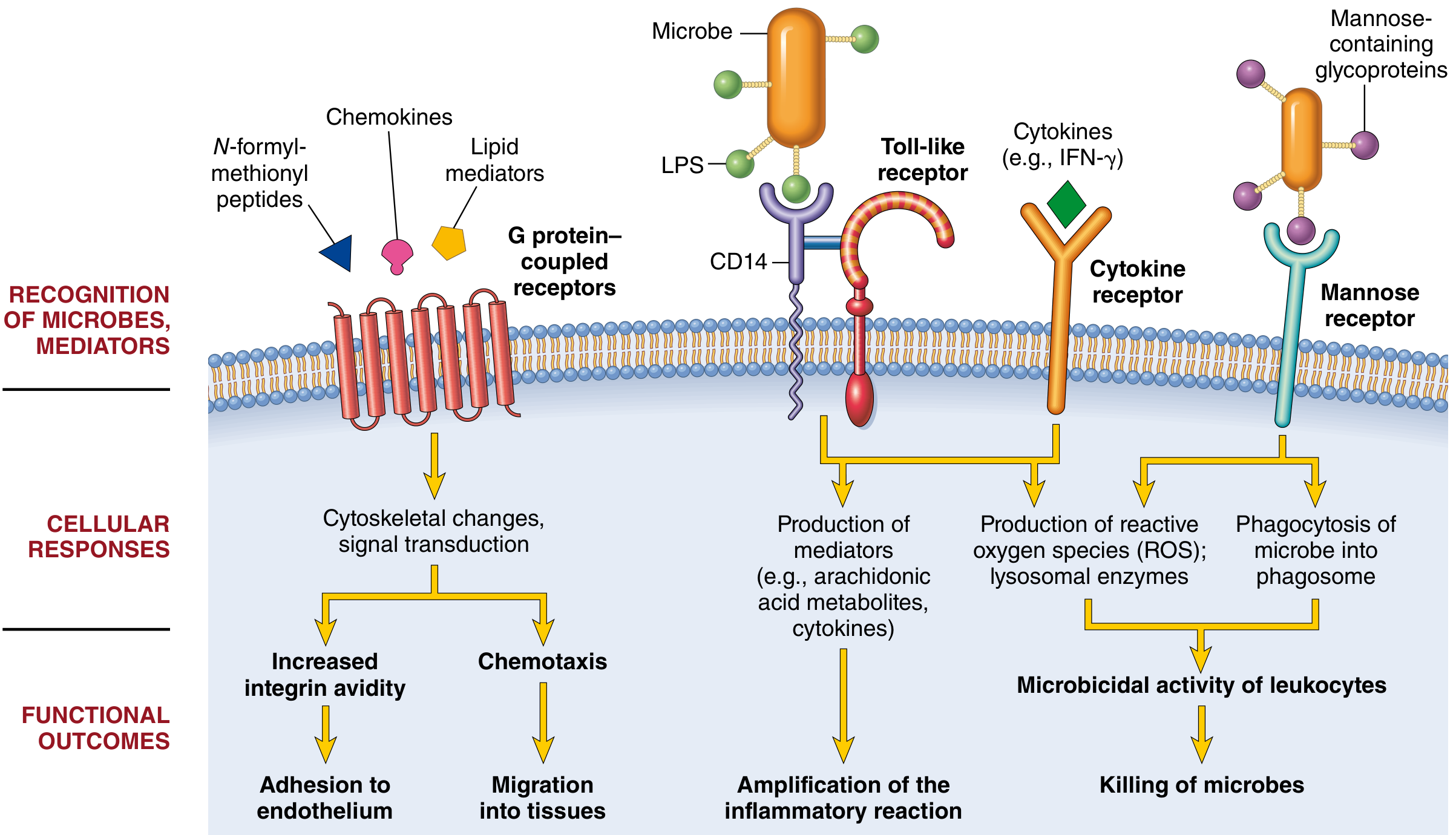
The two principal phagocytes are neutrophils and macrophages. Once leukocytes are recruited to a site of infection or cell death, they must be activated to perform their defensive functions. Recognition of microbes or dead cells triggers a set of leukocyte responses collectively called leukocyte activation.
Neutrophils vs. Macrophages - Key Differences
| Feature | Neutrophils | Macrophages |
|---|---|---|
| Origin | HSCs in bone marrow | HSCs in bone marrow (inflammatory); yolk sac/fetal liver (tissue-resident) |
| Lifespan in tissues | 1-2 days | Days-weeks (inflammatory); years (tissue-resident) |
| Response speed | Rapid, short-lived | Slower, more prolonged |
| ROS production | Prominent respiratory burst | Less prominent |
| Nitric oxide | Low/absent | iNOS-derived (transcriptionally induced) |
| Degranulation | Major response | Not prominent |
| Cytokine production | Low/absent | Major functional activity |
| NET formation | Yes - rapidly induced | No |
| Lysosomal enzyme secretion | Prominent | Less |
Both cell types share phagocytosis, chemotaxis, and ability to migrate through vessels into tissues.
Phagocytosis - Three Sequential Steps
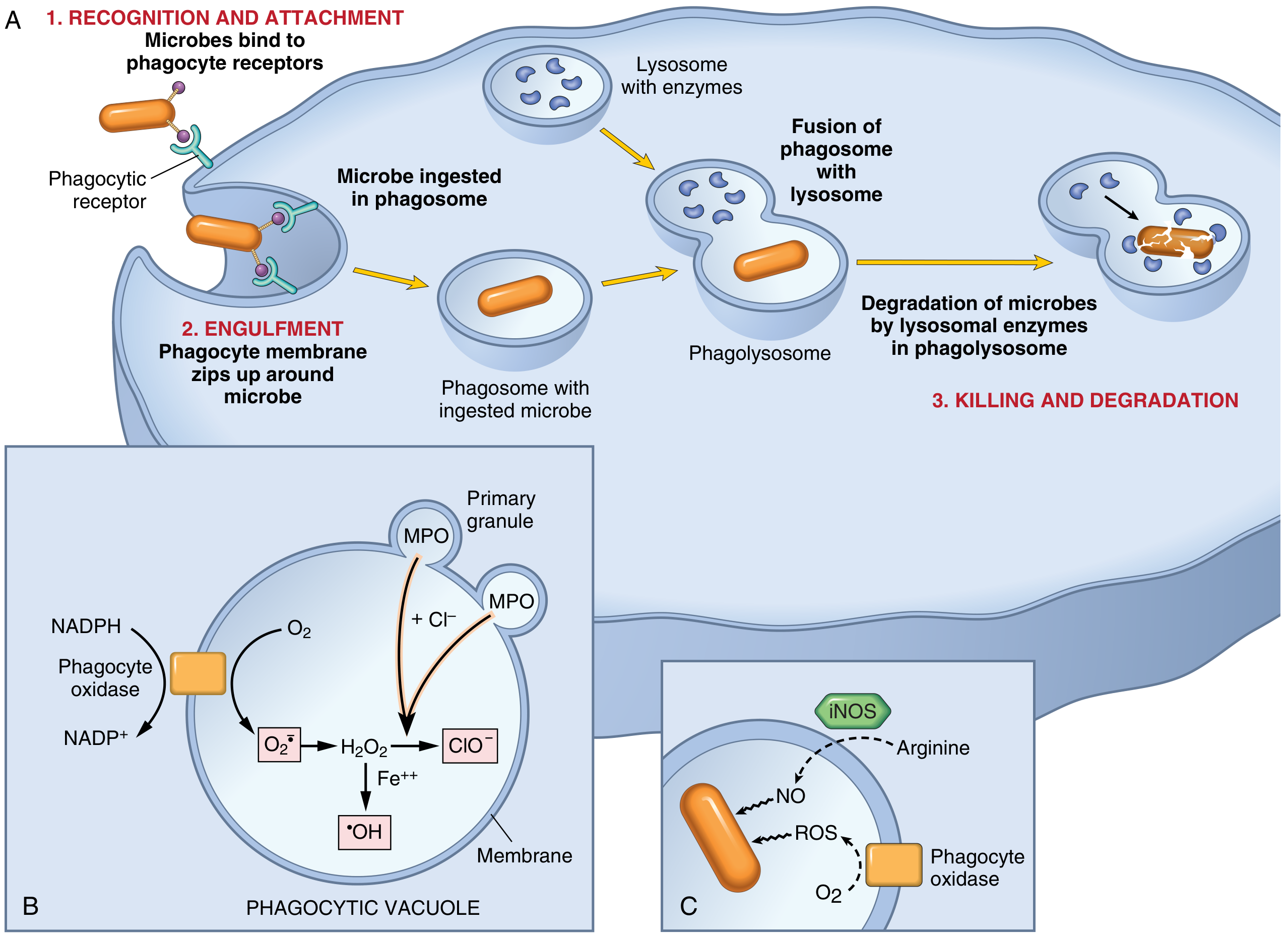
Step 1: Recognition and Attachment
Phagocytes recognize and bind particles via several receptors:
- Mannose receptor - a lectin that binds terminal mannose and fucose residues on microbial glycoproteins/glycolipids. Mammalian glycoproteins have terminal sialic acid or N-acetylgalactosamine instead, so this receptor selectively recognizes microbes, not host cells.
- Scavenger receptors - bind oxidized/acetylated LDL and a variety of microbes
- MAC-1 (CD11b/CD18, integrin) - also binds microbes for phagocytosis
Role of Opsonins (Critical Efficiency Boost)
Phagocytosis is greatly enhanced when microbes are coated with opsonins, for which phagocytes have high-affinity receptors:
| Opsonin | Source | Phagocyte Receptor |
|---|---|---|
| IgG antibodies | B cells/plasma cells | Fc receptor (FcγR) |
| C3b (complement fragment) | Complement cascade | CR1 (complement receptor 1) |
| Mannose-binding lectin (MBL) | Liver | Mannose receptor / collectin receptors |
Step 2: Engulfment
After the particle binds phagocyte receptors, cytoplasmic pseudopods flow around it. The plasma membrane zips up around the particle and pinches off to form an intracellular vesicle called the phagosome. This process requires cytoskeletal changes - particularly actin filament polymerization - and integration of multiple receptor-initiated signals. During this process, the phagocyte may also release lysosomal contents into the extracellular space.
Step 3: Killing and Degradation
The phagosome fuses with a lysosomal granule to form the phagolysosome. Killing and digestion of microbes occur most efficiently after phagocyte activation. All killing mechanisms are normally sequestered in lysosomes - potentially lethal molecules are segregated from the cell's cytoplasm to protect the phagocyte itself.
Intracellular Destruction Mechanisms
1. Reactive Oxygen Species (ROS) - Respiratory Burst
The centerpiece of neutrophil killing:
- Activation assembles NADPH oxidase (phagocyte oxidase) on the phagolysosome membrane
- NADPH oxidase reduces O₂ to superoxide anion (O₂•⁻)
- Superoxide is converted to H₂O₂
- Myeloperoxidase (MPO) in azurophil (primary) granules + Cl⁻ → converts H₂O₂ to hypochlorite (ClO⁻), a potent antimicrobial that kills by halogenation and oxidation of proteins/lipids
- H₂O₂ + Fe²⁺ (Fenton reaction) → hydroxyl radical (•OH) - another powerful destructive agent
The H₂O₂-MPO-halide system is the most efficient bactericidal system of neutrophils.
The production of ROS coupled with oxygen consumption is called the respiratory burst.
Clinical link: Genetic defects in NADPH oxidase (phagocyte oxidase) cause chronic granulomatous disease (CGD) - an immunodeficiency characterized by recurrent bacterial and fungal infections and granuloma formation, because phagocytes can engulf but cannot kill microbes.
2. Reactive Nitrogen Species (RNS) - Nitric Oxide
- iNOS (inducible nitric oxide synthase) is upregulated in macrophages in response to microbial products and IFN-γ
- iNOS converts arginine → NO
- NO + O₂•⁻ → peroxynitrite (ONOO⁻) - a highly reactive molecule that attacks and damages lipids, proteins, and nucleic acids of microbes
- Mainly operative in macrophages (neutrophils produce little/no NO)
3. Lysosomal Granule Enzymes
Neutrophils have two main granule types:
| Granule | Also Called | Contents |
|---|---|---|
| Azurophil (primary) granules | Larger | MPO, defensins, lysozyme, acid hydrolases, elastase, cathepsin G, proteinase 3, nonspecific collagenases |
| Specific (secondary) granules | Smaller | Lysozyme, collagenase, gelatinase, lactoferrin, plasminogen activator, histaminase, alkaline phosphatase |
Both granule types fuse with phagocytic vacuoles, or their contents can be released extracellularly during frustrated phagocytosis.
Functions of granule enzymes:
- Acid proteases - degrade bacteria and debris within the acidified phagolysosome
- Neutral proteases (elastase, collagenase) - degrade extracellular components (collagen, basement membrane, fibrin, elastin, cartilage) - causing tissue destruction
- Lysozyme - hydrolyzes the muramic acid-N-acetylglucosamine bond in bacterial glycoprotein coat
- Lactoferrin - iron-binding protein (deprives bacteria of iron)
- Defensins - cationic arginine-rich peptides that are directly toxic to microbes
- Cathelicidins - antimicrobial proteins in neutrophils and other cells
- Major basic protein (eosinophils) - cytotoxic to helminths
Antiprotease control system:
- α₁-antitrypsin - major inhibitor of neutrophil elastase. Deficiency → uncontrolled elastase → emphysema (lung elastic fiber destruction)
- α₂-macroglobulin - antiprotease in serum/secretions
Neutrophil Extracellular Traps (NETs)
NETs are extracellular fibrillar networks that concentrate antimicrobial substances at infection sites and trap microbes to prevent their spread.
Stimuli: Bacteria, fungi, chemokines, cytokines (especially interferons), complement proteins, ROS
Structure: Viscous meshwork of nuclear chromatin (decondensed DNA + histones) studded with:
- Antimicrobial peptides (defensins)
- Enzymes: MPO, elastase
Mechanism of formation:
- ROS-dependent activation of an arginine deaminase converts arginines → citrulline
- Chromatin decondensation begins
- MPO and elastase enter the nucleus → further chromatin decondensation
- Nuclear envelope ruptures → chromatin is extruded
- Neutrophil loses its nucleus and dies (NETosis)
Functional significance:
- Trap and kill bacteria and fungi extracellularly
- Detected in blood during sepsis
- NETs can cause collateral tissue damage - NET-derived histones are cytotoxic and contribute to endothelial injury
- NETs promote thrombosis - implicated in some vascular diseases
Leukocyte-Mediated Tissue Injury
The same mechanisms that kill microbes can injure the host. This occurs when:
- Inflammation is triggered by non-degradable stimuli (e.g., urate crystals in gout, silica in silicosis)
- Frustrated phagocytosis - when phagocytes encounter materials too large to ingest (e.g., immune complexes on glomerular basement membranes), they are strongly activated and release lysosomal enzymes extracellularly
- Autoimmune disease - host tissues are attacked
- Hypersensitivity reactions (allergy, asthma) - response to harmless environmental antigens
The mechanisms that function to eliminate microbes (physiologic role) are also capable of damaging normal tissues (pathologic consequence).
Lysosomal contents released extracellularly by:
- Controlled secretion during normal leukocyte activation
- Frustrated phagocytosis
- Phagolysosome membrane damage (e.g., by urate crystals)
Other Functional Responses of Activated Leukocytes (Macrophages)
Beyond microbicidal activity, activated macrophages also:
- Produce cytokines (TNF, IL-1, IL-12) - amplify or limit inflammation
- Produce growth factors (VEGF, PDGF, TGF-β) - stimulate endothelial cells and fibroblasts
- Secrete enzymes (collagenase, MMP) - remodel connective tissue
- Initiate tissue repair and scar formation
This makes macrophages central cells not only in acute inflammation but also in chronic inflammation and tissue repair.
Summary Box
Phagocytosis proceeds through recognition (via mannose receptor, scavenger receptors, or opsonin receptors for IgG and C3b) → engulfment (phagosome formation via actin polymerization) → killing (ROS via NADPH oxidase, NO via iNOS, lysosomal enzymes in the phagolysosome). NETs provide an additional extracellular trapping mechanism. The same weapons used against microbes can damage host tissue if directed inappropriately.
Sources: Robbins, Cotran & Kumar - Pathologic Basis of Disease (10e), Ch. 3; Robbins & Kumar - Basic Pathology (11e), Ch. 2
This is a shared conversation. Sign in to Orris to start your own chat.