Principles of left heart bypass (left aorta femoral bypass)
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Reading File
Loading Image
Here is a comprehensive overview of the principles of left heart bypass (LHB), also called left atrial-to-femoral bypass or partial bypass:
Left Heart Bypass (Left Atrio-Femoral / Left Aorto-Femoral Bypass)
What It Is and Why It Is Used
LHB is a form of partial cardiopulmonary bypass used during open surgery on the descending thoracic aorta and thoracoabdominal aorta (e.g., descending aortic aneurysm, thoracoabdominal aneurysm, aortic dissection, coarctation). When the aorta is cross-clamped, two problems arise simultaneously:
- Proximal hypertension - acute increase in LV afterload proximal to the clamp
- Distal ischemia - global ischemia of all structures below the clamp (spinal cord, kidneys, gut, lower limbs)
LHB solves both problems by diverting blood from the left side of the heart and returning it to the distal aorta/femoral artery, thus decompressing the proximal circulation and perfusing the distal circulation at the same time. It does not require cardiac arrest or full CPB.
Circuit Components
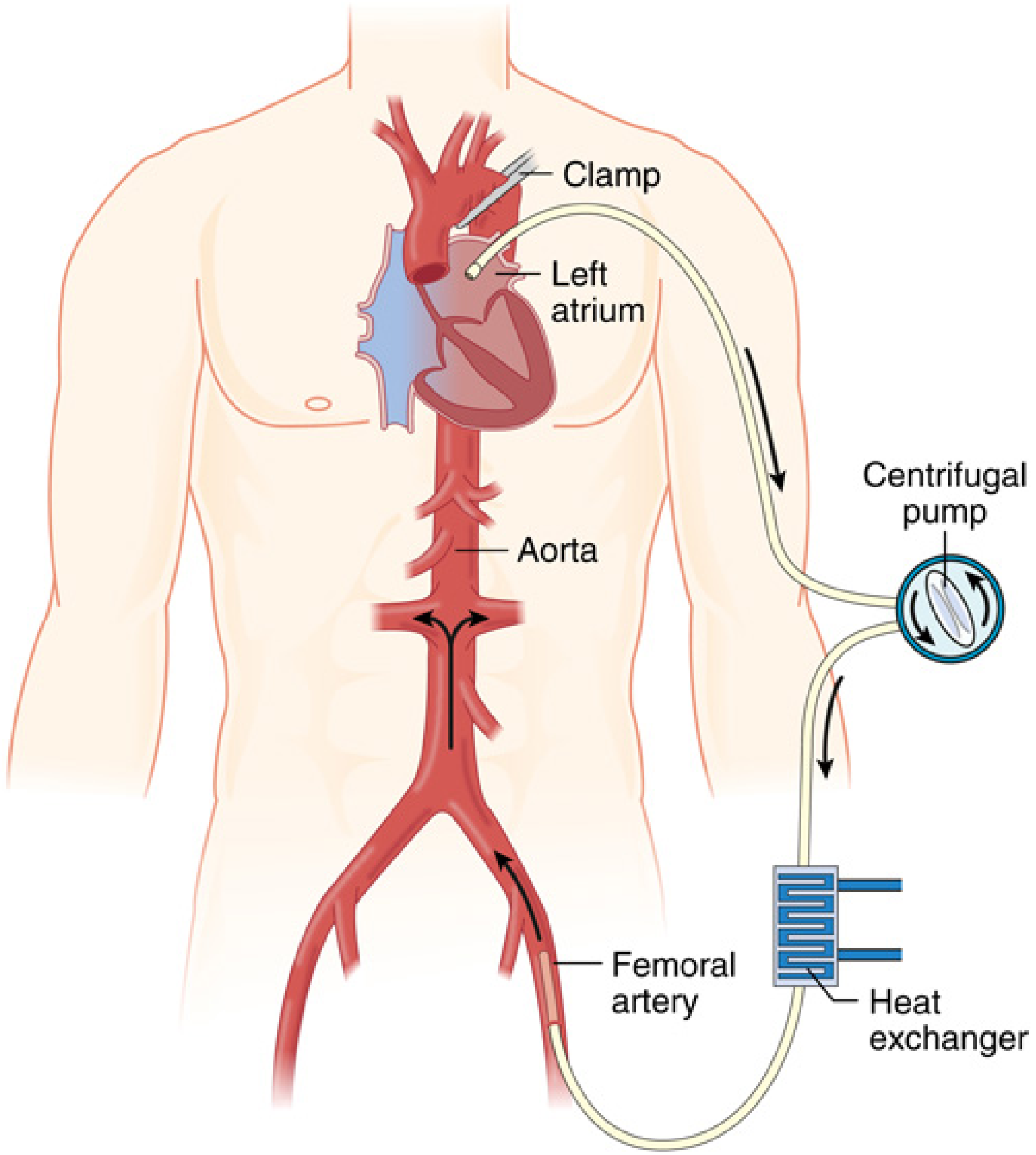
Simple LHB (most common):
- Venous cannula in the left atrium (or left ventricle / proximal descending thoracic aorta as a variant)
- Centrifugal pump (e.g., Biomedicus) - draws blood from the left atrium
- Return cannula in the left femoral artery (retrograde distal perfusion)
- Optional heat exchanger for temperature management
- Heparin-coated tubing - no oxygenator needed (only left-sided bypass, lungs still oxygenate)
Complex/Complete LHB:
Adds an oxygenator, reservoir, and full heat exchanger - useful when the patient has:
- Single-lung ventilation with poor oxygenation
- Significant hypothermia risk
- Major blood loss / hemodynamic instability
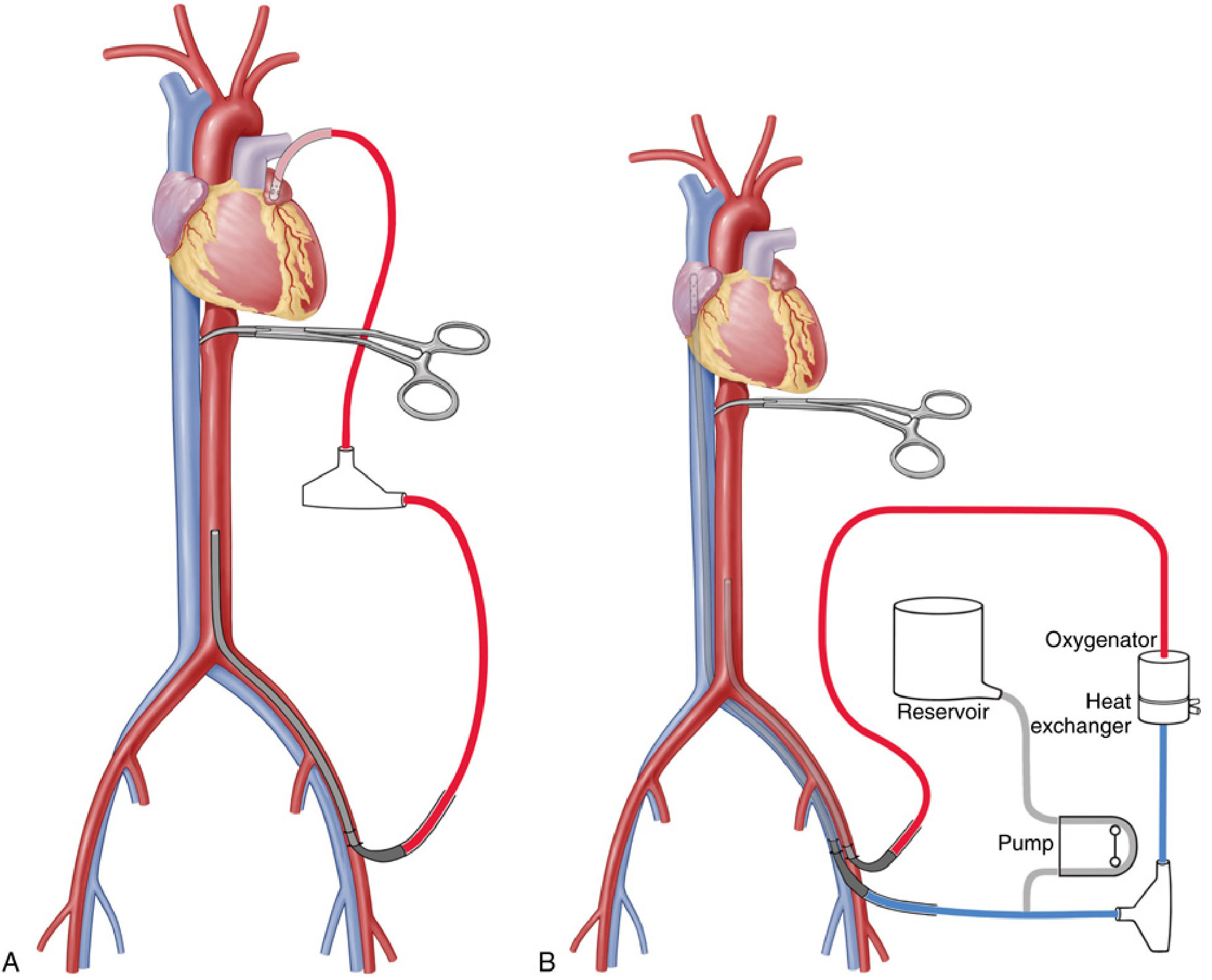
Fig. 50.17 from Miller's Anesthesia - (A) Simple LHB: left atrium, centrifugal cone, and femoral artery. (B) Complex LHB: adds oxygenator, heat exchanger, and reservoir.
Physiological Principles
| Goal | Mechanism |
|---|---|
| Reduce LV afterload | Unloads the proximal aorta; blood bypasses the clamp |
| Reduce LV preload (with LA cannulation) | Diverts blood before it reaches the LV |
| Maintain distal perfusion | Returns flow to femoral artery, perfusing distal organs |
| Spinal cord protection | Keeps distal aortic pressure >60 mmHg; reduces anterior spinal artery ischemia |
| Renal protection | Continuous perfusion prevents renal tubular ischemia |
| Visceral protection | Balloon perfusion cannulas off the LHB circuit can selectively perfuse the celiac axis and SMA |
The key management goal during LHB is to maintain arterial blood pressure >60 mmHg both proximal AND distal to the aortic cross-clamp throughout the procedure. - Miller's Anesthesia, 10e
Cannulation Sites
- Inflow (venous side): Left atrium (standard via left thoracotomy). Alternatives: left ventricle, aortic arch, or proximal descending thoracic aorta
- Outflow (arterial return): Left femoral artery (standard). Alternative: distal descending aorta
Effect of cannulation site on cardiac physiology:
- Left atrial cannulation → reduces LV preload and reduces cardiac output
- Aortic arch / proximal aorta cannulation → reduces LV afterload
- Either way: proximal hypertension is controlled and distal perfusion is maintained
Anticoagulation
Full-dose heparin (as in standard CPB) is not required because:
- The circuit surface area is reduced (no large reservoir)
- Heparin-bonded/coated tubing is used
Typical dose: 100 units/kg (partial bypass dose). This attenuates contact activation and coagulopathy compared to full CPB. ACTs are kept at 180-250 seconds if an oxygenator is added.
Intraoperative Management
Initial pump flow is set to approximately 50% of the patient's cardiac output when the proximal clamp is applied. Flow is then titrated to maintain target pressures proximal and distal. Key points:
- Dual arterial line monitoring is mandatory - one proximal (radial or brachial) and one distal (femoral), to monitor both sides of the clamp
- Continuous communication between surgeon, anesthesiologist, and perfusionist is essential
- Flow is reduced during visceral/renal artery reimplantation (only lower limbs receive bypass at that point)
- Sequential aortic clamping allows intercostal artery reimplantation with minimal flow adjustments
- Mild permissive hypothermia (32-34°C) protects organs during obligatory ischemia periods
- Active rewarming to 37°C after distal anastomosis completion
Temperature monitoring note: With LHB, the femoral return warms/cools the lower body first. The lower body temperature (bladder/rectal) lags behind the upper body. Unlike full CPB (where upper body lags), the lower body temperature should be the end point for cooling and warming.
Spinal Cord Protection Strategy
LHB is one component of a multimodal protocol for spinal cord protection, especially in Crawford extent I and II thoracoabdominal repairs:
- LHB during proximal anastomosis (maintains distal spinal cord perfusion)
- Cerebrospinal fluid (CSF) drainage - reduces CSF pressure, increases spinal cord perfusion pressure (Class I, Level B recommendation)
- Aggressive reattachment of segmental arteries (T8-L1 are most critical)
- Motor evoked potential monitoring
- Moderate hypothermia (32-34°C)
Comparison to Other Techniques
| Technique | Complexity | Distal Perfusion | Cardiac Unloading | Heparin |
|---|---|---|---|---|
| Clamp-and-sew | Simplest | None | None | None |
| Gott shunt (passive) | Simple | Passive only | Minimal | None (heparin-bonded) |
| LHB (simple) | Moderate | Active, adjustable | Yes | Partial (100 U/kg) |
| Full CPB | Most complex | Active | Full | Full dose |
Decline in Use
The widespread adoption of endovascular techniques (TEVAR) for descending thoracic aortic pathology has significantly reduced the use of LHB in contemporary practice. It remains the preferred perfusion strategy when open repair is required, particularly for extensive thoracoabdominal aneurysms where endovascular repair is not feasible.
Sources:
- Miller's Anesthesia, 10e, pp. 7985-7989 (Chapter 52)
- Miller's Anesthesia, 10e, pp. 7580-7583 (Chapter 50 - circuit design)
- Schwartz's Principles of Surgery, 11e, p. 898
This is a shared conversation. Sign in to Orris to start your own chat.