postpartum management of women with GDM - reference fogsi and government of india
FOGSI guidelines postpartum management gestational diabetes mellitus GDM 2023 2024
Government of India MoHFW RSSDI postpartum GDM management guidelines India
https://www.fogsi.org/wp-content/uploads/2024/08/Binder_Hype…
https://www.rssdi.in/newwebsite/RSSDI-Clinical-Practice-Reco…
Postpartum Management of Women with GDM
1. Immediate Postpartum (Day 1-3)
Blood Glucose Management
| Guideline | Recommendation |
|---|---|
| Govt of India / NHM (2018) | Perform FPG and 2-hr PPPG on the 3rd day of delivery before discharge. GDM cases are not discharged before 48 hours (unlike normal PNC). |
| FOGSI (2024) | Women with GDM usually do not need any medical therapy in the immediate postpartum period - blood sugar normalizes on its own. |
| RSSDI (2022) | Most GDM women return to normoglycemia; insulin may be stopped post-delivery. Change glycemic targets to non-pregnant standards. Monitor blood glucose to avoid hypoglycemia. |
Neonatal Care (from Govt of India guidelines)
- All babies born to GDM mothers are monitored for neonatal hypoglycemia (<45 mg/dL) within the first hour of birth and at 4-hour intervals until four stable readings ≥45 mg/dL are achieved.
- Watch for: respiratory distress, convulsions, hyperbilirubinemia.
- If hypoglycemic, refer to a higher centre with 10% dextrose IV infusion (100 mL/kg/day) under paediatric care.
- Children of GDM mothers should be marked as high-risk on the neonatal discharge card for surveillance of obesity, IGT, DM, hypertension, and metabolic syndrome.
2. Postpartum OGTT Screening
Timing
- Govt of India (NHM 2018): 75 g OGTT at 6 weeks postpartum. (ANM performs this at the community level.)
- FOGSI (2024): Postpartum screening at 6-12 weeks for all women with GDM.
- RSSDI (2022): Reassessment at 6-12 weeks postpartum with 75 g OGTT.
Interpretation of 75 g 2-hour OGTT (non-pregnant criteria)
| Result | Fasting PG | 2-hour 75 g PG | Action |
|---|---|---|---|
| Normal / Euglycemic | <100 mg/dL | <140 mg/dL | Lifestyle counseling; repeat OGTT every year |
| Prediabetes / IGT | - | 140-199 mg/dL | Diet, exercise, consider metformin; repeat OGTT yearly |
| Overt Diabetes | ≥126 mg/dL | ≥200 mg/dL | Refer to diabetic clinic for medical therapy |
Subsequent Long-term Screening
- Govt of India: If OGTT is normal at 6 weeks, repeat at 6 months, then every year.
- FOGSI: All women with normal OGTT advised to repeat testing every year.
- RSSDI: Annual screening for prediabetes/T2DM; intensive lifestyle intervention (and/or metformin) for those with prediabetes.
3. Breastfeeding
- FOGSI (2024): Breastfeeding is strongly recommended for all women with DM, whether pregestational or gestational.
- RSSDI (2022): Breastfeeding is recommended as it reduces maternal T2DM risk by ~32%.
- Govt of India / RSSDI: Breastfeeding supports weight management and lowers future NCD risk for both mother and child.
4. Lifestyle Modification and Weight Management
- FOGSI (2024) and Govt of India: Women with GDM are advised to continue a healthy diet and regular exercise to reduce the risk of T2DM.
- Weight retention postpartum is a significant risk factor for future cardiometabolic complications - active weight loss is encouraged.
- RSSDI (2022): Minimum 150 min/week of moderate-intensity physical activity; ≥30 min of aerobic exercise daily (walking, cycling, swimming).
- Medical nutrition therapy (MNT) principles continue into the postpartum period.
5. Contraception and Interconceptional Care
- FOGSI (2024): In women without vascular complications, any contraceptive method may be prescribed (MEC Category 1 or 2). A contraceptive plan should be discussed and implemented before discharge.
- Govt of India (2018): Counseling on postpartum family planning is part of the discharge plan.
- RSSDI (2022): Reminder about the importance of contraception, pre-conception care, and planning for future pregnancies.
- Euglycemic and prediabetic women are given regular follow-up and contraceptive advice.
6. Discharge Counseling (FOGSI 2024)
- Continuation of healthy diet and exercise
- Breastfeeding - strongly encouraged
- Contraception - method to be chosen and initiated
- Need for follow-up OGTT at 6-12 weeks postpartum
- Risk of T2DM - significantly higher risk of progression within 5-10 years
- Other NCDs - dyslipidemia, hypertension, cardiovascular disease
- Child's risk - offspring are high-risk for childhood obesity, metabolic syndrome, IGT, T2DM, and CVD in later life
7. Long-term Surveillance and NCD Linkage
- Govt of India (2018): GDM is classified as part of the NCD programme. Long-term follow-up at NCD clinics, postpartum care clinics, and paediatric setups as per programmatic protocols.
- FOGSI (2024): All women with GDM are advised to visit the clinic for preconceptional evaluation before any subsequent pregnancy.
- RSSDI (2022): Preconception care should be introduced in all women with history of GDM before planning the next pregnancy.
- Postpartum psychosocial assessment and support for self-care is recommended (Govt of India 2018 / RSSDI 2022).
Risk Reminder (FOGSI 2024)
- 30% risk of abnormal OGTT postpartum
- Two-thirds risk of recurrence of GDM in the next pregnancy
- 10-fold increased risk of T2DM compared to non-GDM women
- Increased risk of dyslipidemia, hypertension, and cardiovascular disease
Generate a patient counseling handout on T2DM prevention after GDM diabetes
ls -la /tmp/workspace/ 2>/dev/null || mkdir -p /tmp/workspace && echo "workspace ready"
kindly tell how to manage postpartum women taking insulin in antenatally at higher dose and women who has type 2 diabetes
postpartum insulin management GDM high dose type 2 diabetes FOGSI India guidelines dose reduction
RSSDI postpartum pre-gestational diabetes insulin dose adjustment breastfeeding oral hypoglycemic agents 2022
https://www.fogsi.org/wp-content/uploads/2024/08/Binder_Hype…
https://rssdi.in/newwebsite/pdfdata/Volume-39-Supplement-2-N…
Postpartum Insulin Management: GDM on High-Dose Insulin vs. Pre-existing T2DM
The Physiological Basis
CATEGORY 1: Women with GDM on Insulin Antenatally (including high-dose)
Immediate Postpartum (Day 0-3)
| Step | Recommendation | Source |
|---|---|---|
| Stop insulin at delivery | GDM women on insulin usually do NOT need insulin in the immediate postpartum period. Blood glucose normalizes spontaneously after placental delivery. | FOGSI 2024, DIPSI 2021 |
| Monitor blood glucose | Check FPG and 2-hr PPPG on Day 3 before discharge. GDM cases are NOT discharged before 48 hours. | Govt of India NHM 2018 |
| Do NOT restart insulin unless blood glucose remains elevated | If 2-hr postpartum blood glucose remains ≥140 mg/dL, reassess before restarting insulin. | DIPSI 2021 |
| Watch for rebound hypoglycemia | Women on high antenatal doses are at risk if insulin is continued without dose reduction. | RSSDI 2022 |
What if Blood Glucose Remains High After Delivery?
- If postpartum blood glucose is ≥140 mg/dL, the woman should be re-evaluated for pre-existing undetected T2DM or early diabetes.
- Metformin can be continued (or started) if postpartum blood glucose is high - it is safe during breastfeeding. (DIPSI 2021)
- Insulin is restarted only if glucose remains uncontrolled on lifestyle measures + metformin.
Was the Woman on Very High Antenatal Insulin Doses?
- Are at the highest risk of persistent hyperglycemia postpartum
- Should be fast-tracked for postpartum 75 g OGTT at 6 weeks
- If overt diabetes confirmed (2-hr ≥200 mg/dL or FPG ≥126 mg/dL) - refer to diabetic clinic for long-term therapy
- Should not be treated as routine GDM postpartum
CATEGORY 2: Women with Pre-existing Type 2 Diabetes (Pre-gestational T2DM)
Insulin Dose Reduction Protocol
| Timing | Action |
|---|---|
| Immediately after delivery | Reduce insulin dose to at least 50% below the antenatal (third-trimester) dose |
| First 24-48 hours | Monitor capillary blood glucose every 2-4 hours. Titrate insulin based on readings. |
| Target blood glucose (postpartum, non-pregnant) | FPG: <126 mg/dL; 2-hr PPG: <200 mg/dL (non-pregnant criteria). |
| Progressive reduction | Insulin sensitivity continues to increase over several days - continue titrating down. |
- Third-trimester insulin doses can be 0.9-1.2 units/kg/day due to maximal placental insulin resistance
- Postpartum requirements may be even lower than pre-pregnancy levels initially
- Women who were on NPH or premixed insulin: dose should be individualized and reduced
Resuming Oral Hypoglycemic Agents (OHAs) - Pre-gestational T2DM
| Drug | Postpartum Safety | Recommendation |
|---|---|---|
| Metformin | Safe during breastfeeding - very low transfer to breast milk | Resume immediately if previously on metformin. Continue or initiate. (FOGSI 2024, DIPSI 2021) |
| Sulfonylureas | Glibenclamide passes into breast milk - use with caution; preferably avoid while breastfeeding | Discuss risk-benefit; consider alternative |
| SGLT2 inhibitors | Not recommended during breastfeeding - insufficient safety data | Avoid |
| DPP-4 inhibitors | Safety in lactation not established | Avoid |
| GLP-1 agonists | Not recommended during breastfeeding | Avoid |
| Insulin | Safe - does not pass into breast milk | Continue if OHAs insufficient |
FOGSI 2024 Key Statement: "Pregestational diabetic women previously on oral hypoglycemics should resume the same therapy; women who were on insulin need reduced insulin dose titrated with blood glucose levels."
Blood Glucose Monitoring Frequency (T2DM Postpartum)
- SMBG at minimum: fasting + 2-hr post breakfast + 2-hr post-lunch + 2-hr post-dinner
- This is particularly relevant for the first 1-2 weeks postpartum when dose titration is happening
- Women on insulin while breastfeeding: eat a snack before or during breastfeeding to prevent hypoglycemia (RSSDI 2022)
CATEGORY 3: Special Situation - Breastfeeding and Insulin
- Breastfeeding itself lowers blood glucose due to glucose utilization for milk production
- Risk of hypoglycemia is highest during and immediately after feeds
- RSSDI recommendation: Advise women with insulin-treated diabetes that they are at increased risk of hypoglycemia in the postnatal period, especially when breastfeeding
- Advise them to have a meal or snack available before or during feeds
- Insulin dose may need further reduction once breastfeeding is fully established
- An individualized diabetes diet for breastfeeding mothers is recommended (RSSDI Insulin Consensus 2019)
Postpartum OGTT - Mandatory for Both Groups
| Group | Timing | Purpose |
|---|---|---|
| GDM on high-dose insulin | 6 weeks (Govt of India); 6-12 weeks (FOGSI/RSSDI) | Rule out persistent diabetes / detect if truly T2DM |
| Pre-existing T2DM | At 6-12 weeks | Confirm diabetes classification; assess end-organ function; set long-term management goals |
Summary Algorithm
DELIVERY
|
├── GDM on insulin
│ ├── STOP insulin at delivery
│ ├── Check BG on Day 3
│ ├── If BG normal → lifestyle counseling, OGTT at 6 weeks
│ └── If BG ≥140 mg/dL → consider metformin, re-evaluate for T2DM
│
└── Pre-existing T2DM on insulin
├── REDUCE insulin by ≥50% immediately at delivery
├── SMBG every 2-4 hours initially
├── Resume metformin immediately (safe in breastfeeding)
├── Avoid SGLT2i, GLP-1, DPP-4i in breastfeeding
├── Titrate insulin downward over days-weeks
├── Extra snack before/during breastfeeding feeds
└── Set non-pregnant glycemic targets; long-term T2DM follow-up
evaluation of infertility
evaluation of infertility stepwise approach history examination investigations FOGSI guidelines 2023 2024
https://pmc.ncbi.nlm.nih.gov/articles/PMC10942128
Evaluation of Infertility
Definition
- Women ≥32 years: expedited evaluation after 6 months of failed attempts
- Women <32 years with risk factors (family history of early menopause, known PCOS, prior pelvic surgery, etc.): also evaluated after 6 months or earlier
- ~30% of couples will remain unexplained infertility even after complete workup
Principle: Couple-Oriented, Concurrent Evaluation
- Semen abnormalities (male factor)
- Ovulatory dysfunction
- Tubal/peritoneal factor
- Uterine/cervical factor
- Unexplained (~30%)
PART A: FEMALE EVALUATION
1. History
| Domain | Key Points |
|---|---|
| Menstrual history | Cycle regularity, length, flow; oligomenorrhea/amenorrhea suggests anovulation |
| Obstetric history | Prior pregnancies, outcomes, abortions, ectopic pregnancy |
| Duration of infertility | Primary vs secondary; duration of attempting |
| Coital history | Frequency, timing, dyspareunia, sexual dysfunction |
| Gynecological history | PID, STIs, prior infertility treatment, cervical procedures |
| Surgical history | Pelvic/abdominal surgery (adhesions, tube damage) |
| Medical history | Thyroid disease, PCOS, endometriosis, diabetes, autoimmune disease |
| Medications | Chemotherapy, antidepressants (cause hyperprolactinemia), antipsychotics |
| Family history | Early menopause, genetic conditions |
| Lifestyle | Smoking (accelerates ovarian aging), alcohol, BMI, exercise, stress |
| Occupational | Gonadotoxic exposures (radiation, chemicals) |
2. Physical Examination
| System | Look For |
|---|---|
| BMI | Obesity (PCOS, anovulation) or underweight (hypothalamic amenorrhea) |
| External genitalia / hair pattern | Hirsutism, clitoromegaly, virilization (androgen excess - PCOS, CAH) |
| Breasts | Galactorrhea (hyperprolactinemia) |
| Thyroid | Enlargement, nodules |
| Pelvis | Uterine/adnexal masses, nodularity (endometriosis), tenderness |
| Neurological | Anosmia (Kallmann syndrome), visual field defects (pituitary tumor) |
3. Investigations - Female
A. Ovulation Assessment
| Test | When / Interpretation |
|---|---|
| Mid-luteal serum progesterone (Day 21 of 28-day cycle) | >300 ng/dL (9.5 nmol/L) or >3 ng/mL confirms ovulation; primary test |
| Urinary LH kits (OPK) | Detects LH surge 24-36 hrs before ovulation; useful for timing; 70-92% predictive |
| Basal body temperature (BBT) | Rise of 0.1-0.3°C indicates post-ovulatory progesterone rise; only retrospective, low clinical utility now |
| Transvaginal USG (follicle monitoring) | Serial TVS - monitors follicular growth and confirms collapse (gold standard for ovulation confirmation in clinical setting) |
B. Ovarian Reserve Testing
| Test | Normal Values | Significance |
|---|---|---|
| Basal FSH (Day 2-3) | <10 IU/L normal; >30 IU/L = likely POI | High FSH = diminished reserve |
| Basal Estradiol (E2) (Day 2-3) | <80 pg/mL | Elevated E2 with normal FSH can mask poor reserve |
| Anti-Mullerian Hormone (AMH) | 1.0-3.5 ng/mL (varies by age) | Best single marker; does not vary with cycle day; predicts ovarian stimulation response |
| Antral Follicle Count (AFC) | ≥6-10 total | Transvaginal USG Day 2-5; correlates with ovarian reserve and IVF response |
| Inhibin B | Research use only; adds little beyond FSH/AMH |
AMH is the most useful marker: predicts hyper- vs. hypo-response to stimulation; especially valuable when AFC is low or woman is >35 years. (Tietz Textbook, 7th Ed)
C. Endocrine Profile
| Hormone | Indication |
|---|---|
| TSH | Rule out hypothyroidism/hyperthyroidism |
| Prolactin (PRL) | Hyperprolactinemia (draw fasting, early morning) |
| Testosterone (T) | Androgen excess, PCOS, CAH |
| FSH + LH | Distinguish primary (hypergonadotropic) vs central (hypogonadotropic) anovulation |
| 17-OH Progesterone | If hirsutism present - rule out late-onset CAH (21-hydroxylase deficiency) |
| DHEAS | Adrenal androgen excess |
| Fasting glucose / HOMA-IR | PCOS with insulin resistance |
Draw prolactin fasting, early in the day - levels elevate after meals and stress.
D. Tubal and Uterine Evaluation
| Test | Indication / Comments |
|---|---|
| Hysterosalpingography (HSG) | First-line when no pelvic pathology suspected; assesses tubal patency + uterine cavity; less invasive, cost-effective |
| Transvaginal USG (TVS) | Baseline evaluation - uterine morphology, fibroids, polyps, ovarian cysts (endometrioma), AFC |
| Diagnostic Laparoscopy + Hysteroscopy | When pelvic pathology suspected (endometriosis, hydrosalpinx, adhesions, prior PID, abnormal USG); also indicated in unexplained infertility - evaluates tubes, pelvis, and uterine cavity directly |
| Saline Infusion Sonography (SIS/SHG) | Intrauterine pathology (polyps, submucosal fibroids, adhesions); less invasive than hysteroscopy |
| MRI pelvis | Deep infiltrating endometriosis, uterine anomalies |
PART B: MALE EVALUATION
1. History
- Duration of infertility; prior pregnancies with same/different partner
- Reproductive history: undescended testis (cryptorchidism), orchitis, testicular trauma, torsion
- Sexual history: erectile dysfunction, ejaculatory dysfunction, STIs
- Surgical history: hernia repair (vas deferens injury), pelvic/retroperitoneal surgery, varicocelectomy, vasectomy reversal
- Medical history: chemotherapy, radiotherapy, chronic illness, diabetes
- Medications: anabolic steroids (suppress spermatogenesis), sulfasalazine, nitrofurantoin
- Family history: genetic conditions, cystic fibrosis (CBAVD)
- Lifestyle: smoking, alcohol, heat exposure (hot baths, laptop on lap), occupational gonadotoxins
2. Physical Examination
| Area | Look For |
|---|---|
| General | BMI, gynaecomastia, body habitus, virilization |
| Genitalia | Hypospadias, epispadias, phimosis, penile curvature |
| Testes | Size, texture, consistency (normal volume ≥15 mL each); nodules, pain |
| Epididymis | Induration, cysts (obstruction) |
| Vas deferens | Present or absent (CBAVD - cystic fibrosis mutation) |
| Spermatic cord/scrotum | Varicocele (most common correctable male factor); hydrocele |
| Inguinal area | Surgical scars (hernia repair - risk of vas injury) |
3. Semen Analysis (Cornerstone of Male Evaluation)
| Parameter | WHO 2021 Lower Reference Limit |
|---|---|
| Volume | ≥1.4 mL |
| Total sperm count | ≥39 million per ejaculate |
| Concentration | ≥16 million/mL |
| Total motility (PR + NP) | ≥42% |
| Progressive motility (PR) | ≥30% |
| Vitality | ≥54% live |
| Morphology (Kruger strict) | ≥4% normal forms |
| pH | ≥7.2 |
| Term | Meaning |
|---|---|
| Oligospermia | <16 million/mL sperm concentration |
| Asthenospermia | <30% progressive motility |
| Teratospermia | <4% normal morphology |
| Azoospermia | No sperm in ejaculate |
| Oligoasthenoteratozoospermia (OAT) | All three defects combined |
| Aspermia | No ejaculate |
| Hypospermia | Volume <1.4 mL |
| Necrospermia | >96% immotile/dead sperm |
4. Further Male Investigations
| Investigation | When Indicated |
|---|---|
| Repeat semen analysis | All abnormal results; 2-3 samples 2-4 weeks apart |
| FSH, LH, Testosterone | Azoospermia or severe oligospermia; to distinguish obstructive vs non-obstructive azoospermia |
| Prolactin | Suspected hypogonadotropic hypogonadism |
| Karyotype (karyotyping) | Severe oligospermia (<5 million/mL) or non-obstructive azoospermia; Klinefelter syndrome (47,XXY) |
| Y-chromosome microdeletion (AZF) | Non-obstructive azoospermia / severe oligospermia |
| CFTR mutation testing | Bilateral absence of vas deferens (CBAVD) |
| Scrotal Doppler USG | Varicocele (subclinical), testicular masses, epididymal pathology |
| Transrectal USG (TRUS) | Suspected ejaculatory duct obstruction |
| Anti-sperm antibodies | Post-vasectomy reversal, history of testicular trauma/infection |
| Reactive oxygen species (ROS) / Sperm DNA fragmentation | Unexplained infertility, recurrent miscarriage, repeated IVF failure |
| Testicular biopsy / Fine needle aspiration (FNA) | Non-obstructive azoospermia - for sperm retrieval (TESE/micro-TESE) |
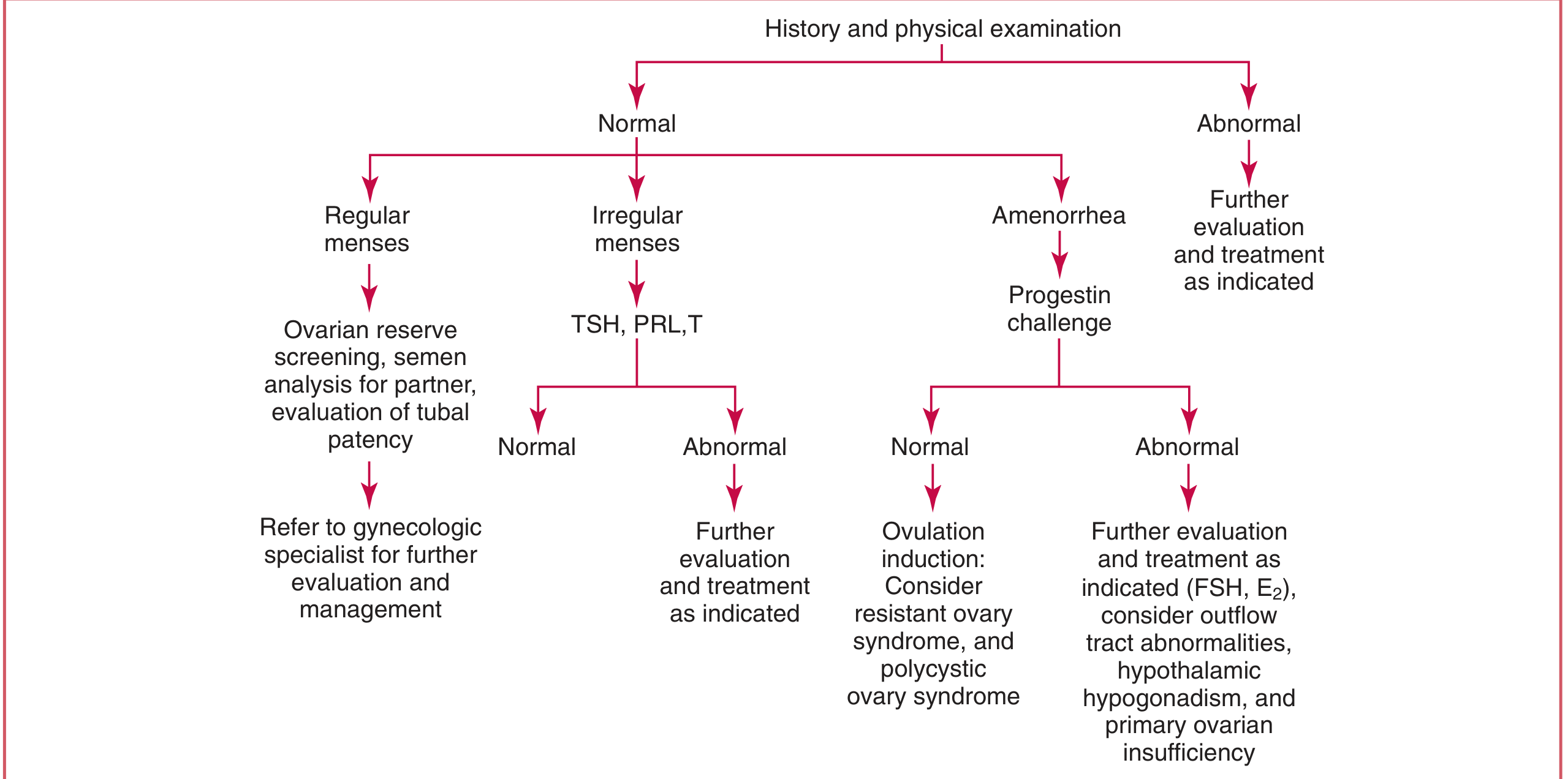
Diagnostic Algorithm for Female Infertility
PART C: WHEN TO EXPEDITE (Indian Context - FOGSI)
- Woman ≥32 years (faster ovarian aging in Indian women)
- Family history of early menopause
- Known/suspected PCOS, endometriosis, uterine anomalies
- Prior pelvic surgery, chemotherapy/radiation
- Oligomenorrhea or amenorrhea (anovulatory - no need to wait 12 months)
- Known male factor (azoospermia, prior vasectomy)
- Both partners HIV positive (immediate referral)
PART D: BASIC INFERTILITY WORKUP - SUMMARY TABLE
| Investigation | Purpose |
|---|---|
| Semen analysis (x2) | Male factor screening |
| Mid-luteal progesterone | Confirm ovulation |
| Basal FSH + E2 (Day 2-3) | Ovarian reserve |
| AMH | Ovarian reserve (especially >32 yrs or risk factors) |
| AFC by TVS | Ovarian reserve + pelvic anatomy |
| TSH, Prolactin, Testosterone | Endocrine causes of anovulation |
| HSG | Tubal patency (first line - no pelvic pathology) |
| Laparoscopy + Hysteroscopy | Tubal/pelvic/uterine pathology (if suspected) |
| Karyotype, Y-microdeletion | Azoospermia / severe oligospermia |
- Tietz Textbook of Laboratory Medicine, 7th Ed - Initial Evaluation of Female Infertility, p. 2381-2385
- Smith & Tanagho's General Urology, 19th Ed - Evaluation of Male Infertility, p. 745
- FOGSI Best Practice Recommendations for Infertility Management - PMC10942128
- WHO/NCBI Approach to Evaluation of Infertility