Different types of Sutures with images
Reading File
Searching the Web
types of sutures surgery images classification
Finding Sources
Loading Image
Loading Image
Reading File
Reading File
Loading Image
Searching the Web
suture stitch patterns interrupted continuous mattress images diagram
Loading Image
Loading Image
Finding Sources
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Reading File
Loading Image
I now have comprehensive material from authoritative textbooks and multiple diagrams. Here is a complete, well-illustrated guide to suture types:
Types of Sutures
Sutures are classified along two major axes: material (what they're made of) and technique (how they're placed). The classification below follows the structure used in Roberts and Hedges' Clinical Procedures in Emergency Medicine, Andrews' Diseases of the Skin, and Fitzpatrick's Dermatology.
Part 1: Classification by Material
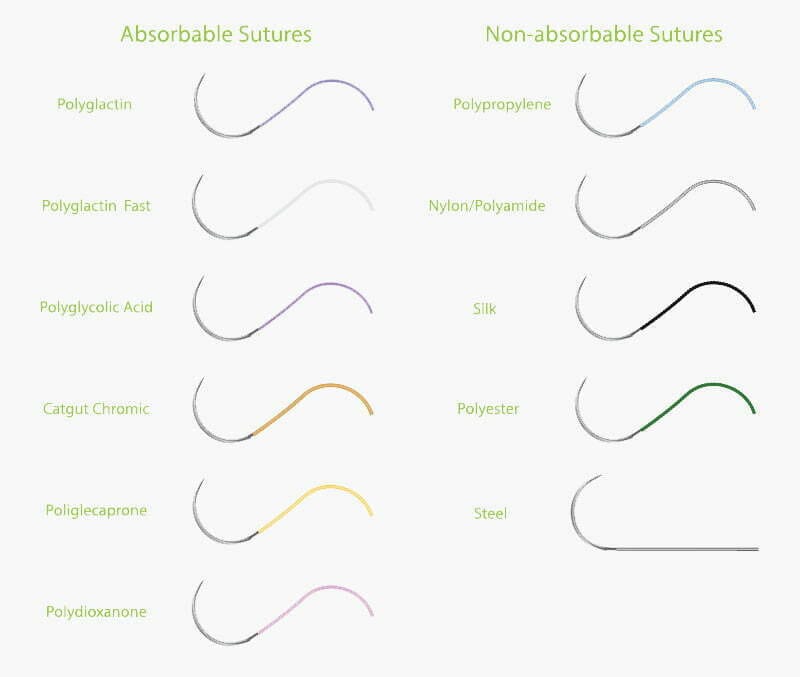
Master Classification Diagram

A. Absorbable Sutures
Defined as losing >50% tensile strength within 60 days of placement. Used primarily for deep (dermal/subcutaneous) layer closure.
| Suture | Type | Tensile Strength Half-Life | Notes |
|---|---|---|---|
| Plain Gut | Natural monofilament | ~7-10 days | Derived from sheep submucosa; high tissue reactivity |
| Chromic Gut | Natural monofilament | ~21 days | Chromium-treated to slow absorption; less reactive than plain gut |
| Polyglycolic Acid (Dexon) | Synthetic multifilament | ~14-21 days | Low tissue reactivity, good handling |
| Polyglactin (Vicryl) | Synthetic multifilament | ~21 days | Most widely used absorbable; Vicryl Rapide absorbs even faster |
| Poliglecaprone (Monocryl) | Synthetic monofilament | ~7-14 days | Excellent tensile strength, low memory |
| Polydioxanone (PDS) | Synthetic monofilament | ~42 days | Longest-lasting absorbable; used for fascia/deep structures |
| Polyglyconate (Maxon) | Synthetic monofilament | ~28 days | Similar to PDS |
B. Non-Absorbable Sutures
Remain indefinitely unless removed. Used for epidermal closure and permanent structural sutures.
| Suture | Type | Memory | Tissue Reactivity | Notes |
|---|---|---|---|---|
| Silk | Natural braided/twisted | Very low | High | Excellent handling and knot security; highest reactivity of common sutures |
| Cotton | Natural twisted | Low | Very high | Rarely used today |
| Nylon (Ethilon, Dermalon) | Synthetic monofilament | High | Low | Standard skin closure; requires extra throws due to high memory |
| Nylon (Nurolon, Surgilon) | Synthetic braided | Low | Low | Better knot security than monofilament nylon |
| Polypropylene (Prolene) | Synthetic monofilament | Very high | Very low | Cardiovascular surgery; lowest tissue reactivity of all sutures |
| Polyester (Mersilene, Ti-Cron) | Synthetic braided | Low | Low | Good knot security; used in cardiac/vascular work |
| Polybutester (Novafil) | Synthetic monofilament | High | Low | Elastic; conforms to wound swelling |
| Stainless Steel | Metallic monofilament | Extreme | Low | Sternum closure; poor handling |
Source: Roberts and Hedges' Clinical Procedures in Emergency Medicine, Table 35.1; Fitzpatrick's Dermatology, Table 202-5
Monofilament vs. Multifilament
| Property | Monofilament | Multifilament (Braided/Twisted) |
|---|---|---|
| Coefficient of friction | Low - passes through tissue easily | High - more drag |
| Capillarity | Low - resistant to bacterial wicking | High - harbors bacteria |
| Memory | High - tends to unravel | Low - knot stays well |
| Knot security | Poor - needs extra throws | Good - fewer throws needed |
| Tissue reactivity | Low | Higher |
Suture Size (USP Scale)
Suture diameter is inversely related to the first digit of the USP designation. Larger number = thinner suture:
| Size | Use |
|---|---|
| 0, 1, 2 | Deep fascia, orthopedics, abdominal wall |
| 2-0, 3-0 | Subcutaneous/deep dermal layers |
| 4-0 | General skin closure (extremities, trunk) |
| 5-0, 6-0 | Face, cosmetically sensitive areas |
Part 2: Classification by Stitch Technique
Basic Suture Patterns

1. Simple Interrupted Suture
The most versatile and widely used stitch. Each suture is placed and tied independently.
- Advantage: If one suture fails, the rest hold. Allows precise tension adjustment at each bite.
- Use: Small punch biopsies, layered closures, high-tension wounds, areas needing exact edge apposition
- Key point: A single suture can be removed to inspect the wound without compromising the full closure
2. Buried (Deep Dermal) Suture
Placed within the dermis with the knot buried away from the surface. This is the workhorse for deep layer closure.
- Advantage: Reduces tension on the surface, promotes wound eversion, minimizes dead space, avoids suture spitting
- Variants: Conventional buried suture (mild eversion) and buried vertical mattress (greater eversion)
3. Simple Running (Continuous) Suture
A single suture placed in a continuous fashion with knots only at each end of the wound.
- Advantage: Much faster than interrupted; evenly distributes tension
- Disadvantage: If suture breaks anywhere, the entire closure is compromised
- Use: Long wounds under minimal tension with well-approximated edges
4. Running Locked (Ford Interlocking) Suture
A variant of the simple running suture where the needle passes through the previous loop before entering tissue.
- Advantage: Creates pressure along the wound edge - useful in highly vascularized areas for additional hemostasis
- Use: Scalp wounds, areas with active oozing
5. Running Subcuticular (Intradermal) Suture
Multiple horizontal bites placed alternately in the dermis, just below the epidermis. The suture runs parallel to the skin surface and is not visible externally.
- Advantage: No external suture marks ("railroad tracks"); can be left in place 2-3 weeks; ideal if patient cannot return for removal
- Use: Trunk and extremity closures; cosmetically sensitive wounds
6. Horizontal Mattress Suture
Two parallel bites placed horizontally across the wound, with the suture crossing perpendicular to the incision.
- Advantage: Excellent tension reduction; useful as a retention suture for large wounds; good wound eversion
- Caution: Can strangulate poorly vascularized tissue (e.g., flaps) - use with care
7. Vertical Mattress Suture
Two bites placed in the same plane perpendicular to the wound - one deep and wide, one shallow and narrow (near-far, far-near pattern).
- Advantage: Closes both deep and superficial layers simultaneously; promotes strong wound eversion
- Use: Areas prone to inversion (e.g., back of neck, dorsum of hand); high-tension closures
8. Purse-String Suture
Multiple horizontal bites taken circumferentially around a circular wound, then pulled tight to close it concentrically.
- Use: Partial or complete closure of circular defects (e.g., after punch excisions); reduces healing time for second-intention wounds
Quick Reference Summary
| Technique | Pattern | Best Use |
|---|---|---|
| Simple Interrupted | Individual knots | Most wounds; high-tension areas |
| Buried Dermal | Knot buried in dermis | Deep layer closure; reduces surface tension |
| Simple Running | Continuous, end knots | Long, low-tension wounds; fast closure |
| Running Locked | Continuous with loops | Vascular areas; hemostasis |
| Subcuticular | Intradermal horizontal | Cosmetic closure; no stitch marks |
| Horizontal Mattress | Wide horizontal bites | Tension relief; large wounds |
| Vertical Mattress | Deep + superficial bites | Wound eversion; prone to inversion |
| Purse-String | Circumferential | Circular defects |
Sources: Roberts and Hedges' Clinical Procedures in Emergency Medicine (9780323354783); Andrews' Diseases of the Skin (9780323547536); Fitzpatrick's Dermatology (9780071837781); Pfenninger and Fowler's Procedures for Primary Care (9780323052672)
Mention individual sutures with their images and its detail and uses
Finding Sources
Searching the Web
individual suture techniques images simple interrupted continuous mattress subcuticular purse string
Reading File
Loading Image
Loading Image
Searching the Web
figure-of-eight suture cruciate suture purse-string Connell Lembert suture diagrams images
Reading File
Loading Image
Loading Image
Reading File
Finding Sources
Loading Image
Reading File
Loading Image
Searching the Web
vertical mattress suture horizontal mattress suture figure of eight suture diagram cross section images
Loading Image
Loading Image
Loading Image
Now I have all the material needed. Here is a comprehensive, image-rich guide to every individual suture type:
Individual Sutures - Detailed Guide with Images
The following covers every major suture technique used in surgery, emergency medicine, and dermatology, drawn from Roberts and Hedges' Clinical Procedures in Emergency Medicine, Hinman's Atlas of Urologic Surgery, and Andrews' Diseases of the Skin.
Visual Overview of All Major Suture Patterns
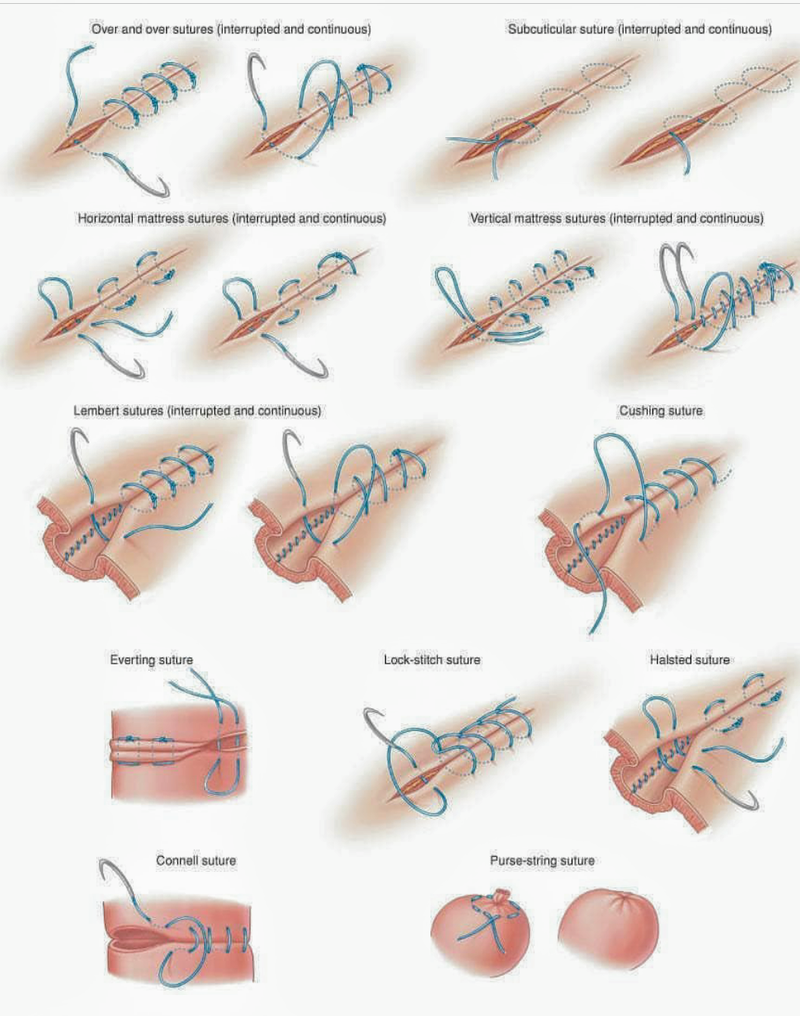
GROUP 1: INTERRUPTED SUTURES
Each stitch is placed and tied independently.
1. Simple Interrupted Suture

Technique:
- The needle enters the skin perpendicularly, ~4-8 mm from the wound edge on one side
- It passes through the full thickness of skin and exits the opposite side at the same distance
- The suture is tied and cut; the process repeats along the wound
Characteristics:
- Each suture is completely independent - if one fails, all others remain intact
- Allows precise, individual tension control at each bite
- Slightly time-consuming compared to continuous techniques
Uses:
- The most commonly used suture in clinical practice
- Small punch biopsy closures
- High-tension wounds where individual adjustment is needed
- Layered closures combined with deep dermal sutures
- Wounds where early partial removal may be needed (e.g., infected wound monitoring)
- Facial lacerations requiring precise edge alignment
- Any wound where a step-off deformity (epidermal level mismatch) needs correction
2. Buried (Deep Dermal) Suture
Technique:
- The needle starts deep in the dermis/subcutaneous fat, enters from below, and the knot is buried away from the skin surface
- The stitch is in the dermis and fat; the knot is cut short and buried to minimize tissue reaction
- Two variants: Conventional buried (mild eversion) and buried vertical mattress (moderate to significant eversion)
Characteristics:
- Knot sits entirely below the skin - no external visible suture
- Gradually loses tensile strength as the scar gains its own intrinsic strength
- A scar has only 5-10% of original skin strength at 2 weeks - this suture bridges that gap
- Reduces tension on the surface closure, minimizes dead space, and promotes wound eversion
Uses:
- Deep layer (dermal/subcutaneous) closure in any layered wound
- Prevents wound dehiscence in larger or deeper wounds
- Eliminates dead space to reduce hematoma/seroma risk
- Situations where the patient cannot return for suture removal (absorbable suture used)
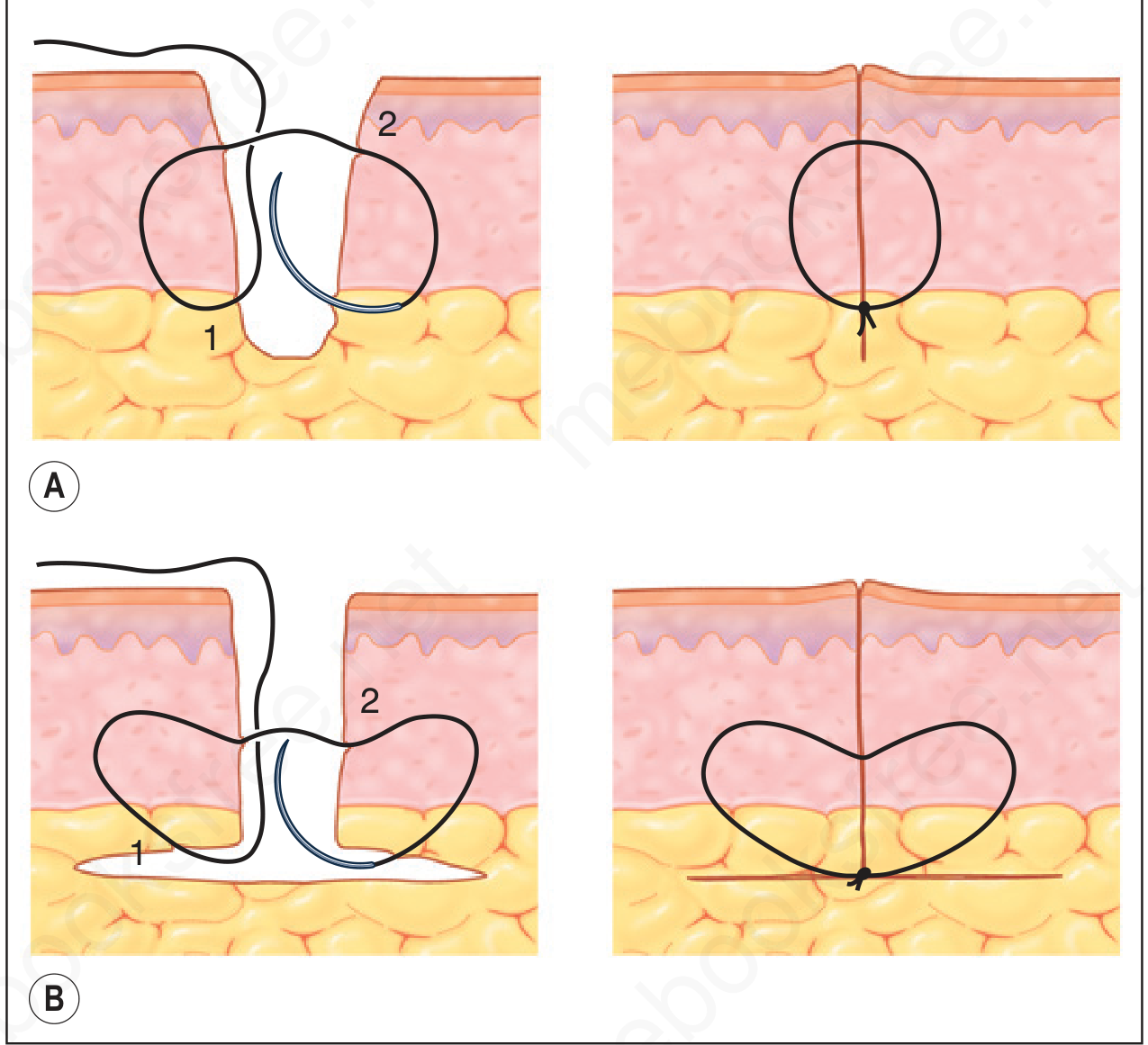
3. Vertical Mattress Suture (Near-Far, Far-Near)
Technique:
- First, a deep wide bite is taken 6-8 mm from the wound edge, passing through full thickness (the "far-far" bite)
- Then a superficial narrow bite is taken 1-2 mm from the wound edge, passing through only the upper dermis (the "near-near" bite)
- Both bites are on the same axis (perpendicular to the wound), creating a figure-8 shape
Characteristics:
- Closes both deep and superficial layers simultaneously with a single suture
- Strong wound eversion - the most reliable technique for everting wound edges
- Eliminates dead space
- Requires more time and may cause more tissue strangulation than simple interrupted
Uses:
- Areas prone to wound inversion (dorsum of hand, back of neck, scalp)
- High-tension closures needing both deep and superficial support
- Alternatively placed between simple interrupted sutures for eversion in difficult areas
- Can replace a two-layer closure (deep + surface) in areas without excessive tension
Source: Roberts and Hedges' Clinical Procedures in Emergency Medicine, p.799
4. Horizontal Mattress Suture
Technique:
- The needle enters the skin and crosses the wound like a simple interrupted suture
- Instead of tying, the needle re-enters 6-8 mm laterally on the same side it exited
- It then crosses back to the starting side, exiting directly across from the second entry
- Both ends end up on the same side and are tied, creating a rectangular suture loop
Characteristics:
- Orients 90 degrees to the vertical mattress pattern
- Distributes tension over a wider area than simple interrupted
- Risk of tissue strangulation and necrosis in poorly vascularized tissue (e.g., flaps)
Uses:
- Reducing tension in large wounds or wounds under high static tension
- "Retention suture" for very large wounds
- Areas where eversion is desired but subcutaneous tissue is sparse
- The half-buried horizontal mattress variant (corner stitch) is ideal for the apex of V-shaped flaps - protects the tip without compromising its blood supply
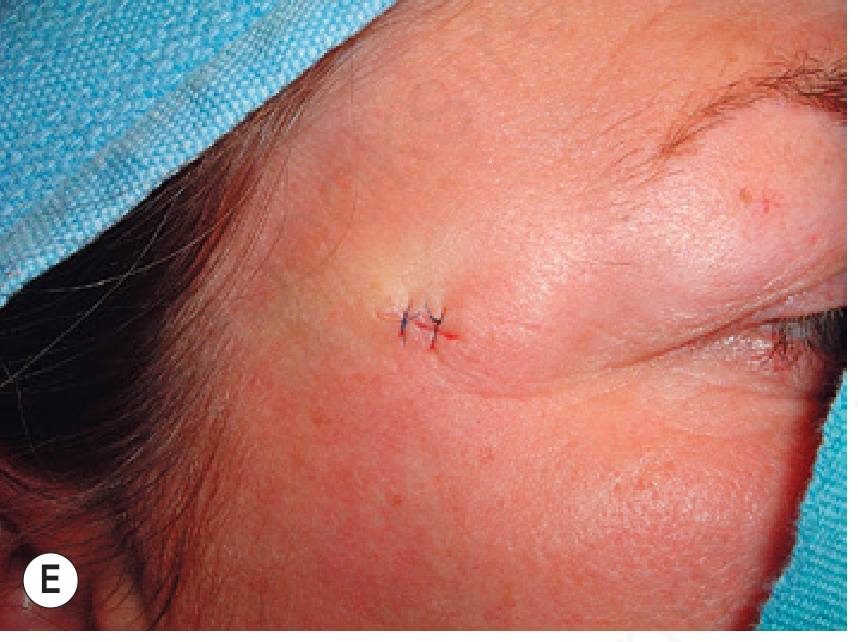
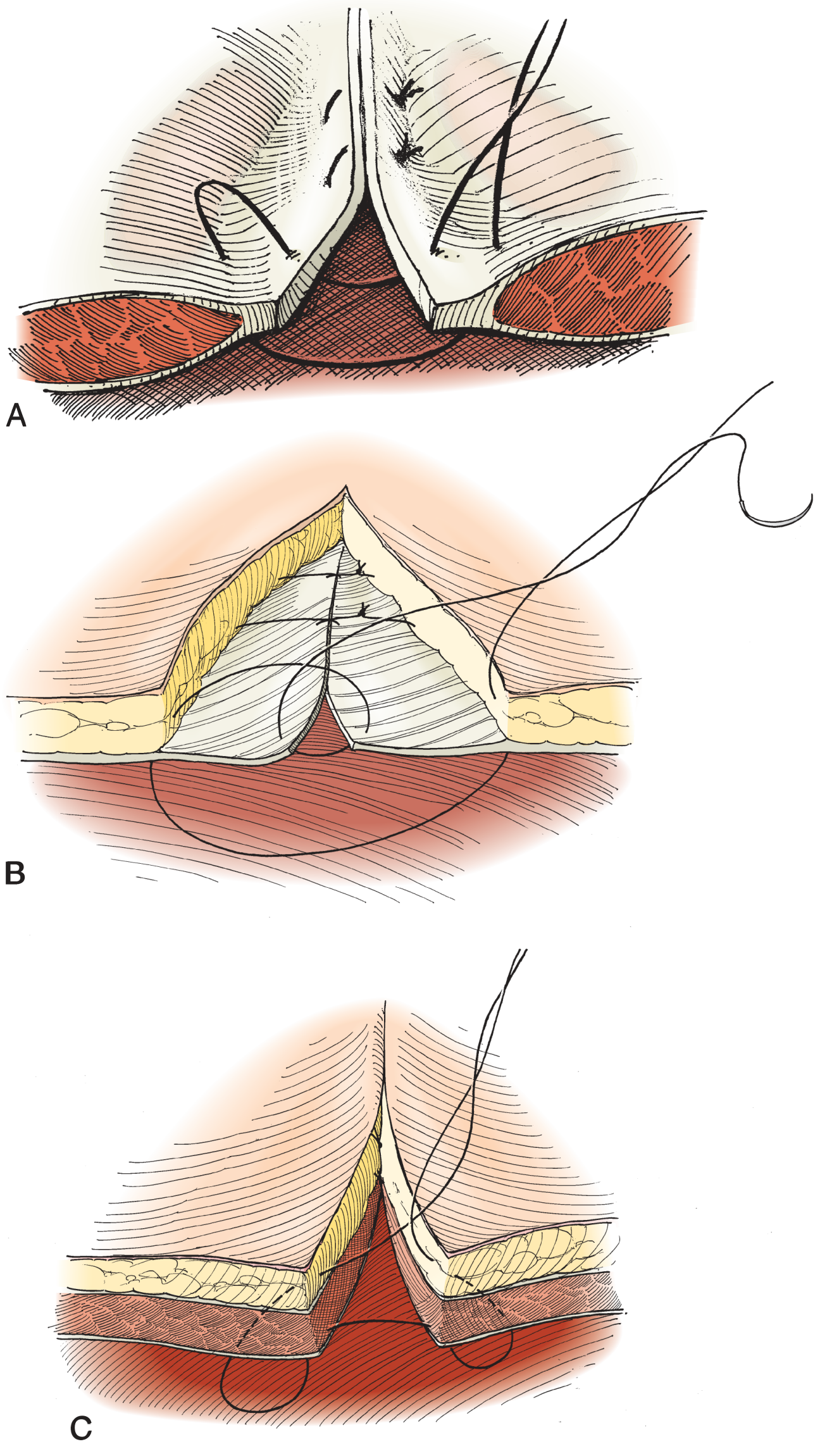
5. Figure-of-Eight (Cruciate Mattress) Suture
Technique:
- Like a horizontal mattress but the second pass crosses diagonally, creating an X (cross) shape on the skin surface
- Results in two overlapping triangular loops that share a common knot
Characteristics:
- Distributes tension in two directions simultaneously
- Strong tension-distributing properties in a compact stitch
- Also called the "cruciate suture" or "cross mattress suture"
Uses:
- Fascial closure (e.g., abdominal wall fascia)
- Tendon repair
- Areas requiring strong tension distribution in a small space
- Bone/periosteum suturing in orthopedic and dental procedures
- Closing the apex of a complex V-shaped wound
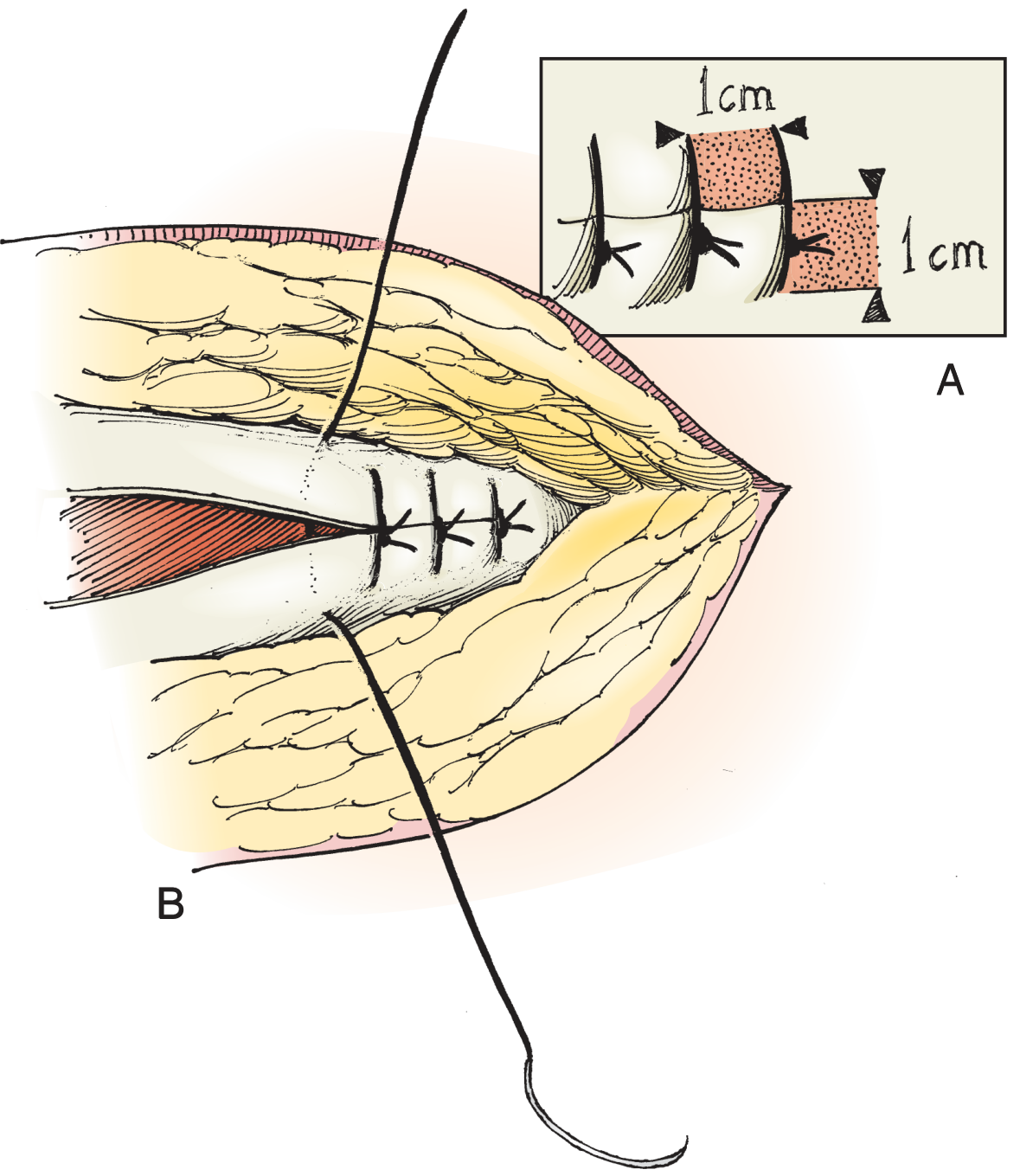
6. Far-and-Near (Smead-Jones) Suture
Technique:
- A large bite (far-far) through all layers of the abdominal wall is taken, then a smaller bite (near-near) through the fascial edge only
- Creates a combined deep and superficial bite in one stitch
Characteristics:
- Provides mass closure of multiple layers simultaneously
- Strong and distributes tension across the entire wound width
Uses:
- Abdominal wall (mass closure) - laparotomy closure
- Closure of fascia in re-operations or contaminated wounds (Smead-Jones technique)
- Reduces risk of incisional hernia in high-tension midline closures
GROUP 2: CONTINUOUS (RUNNING) SUTURES
A single suture is placed in a continuous fashion, with knots only at each end.
7. Simple Running (Over-and-Over) Suture
Technique:
- Begins with a single interrupted stitch at one end, tied but not cut
- The needle then continues along the wound, taking successive equal bites at equal intervals, crossing the wound at a consistent angle
- A final knot is tied at the other end using the last loop and the free end
Characteristics:
- Tension is distributed evenly along the entire wound length
- Faster than interrupted sutures - only 2 knots for any wound length
- Accommodates mild wound swelling
- Disadvantage: If suture breaks anywhere, the entire closure may fail
Uses:
- Long, low-tension wounds with well-apposed edges
- Cosmetic surface closures when subcutaneous layer has been properly closed
- Scalp lacerations (fast and effective)
- Peritoneum and fascial closures
8. Running Locked (Ford Interlocking) Suture
Technique:
- A continuous suture where the needle passes through the loop of the previous stitch before entering tissue on each pass
- Creates a locked chain pattern where each bite self-locks
Characteristics:
- Creates additional pressure along the wound edges
- More hemostatic than simple running due to compression of wound edges
- Cannot easily adjust individual loop tension after placement
Uses:
- Highly vascularized regions where hemostasis is needed (scalp, oral mucosa)
- Situations requiring firm edge apposition with simultaneous compression
- Gastric or intestinal mucosal edges (avoiding puckering)
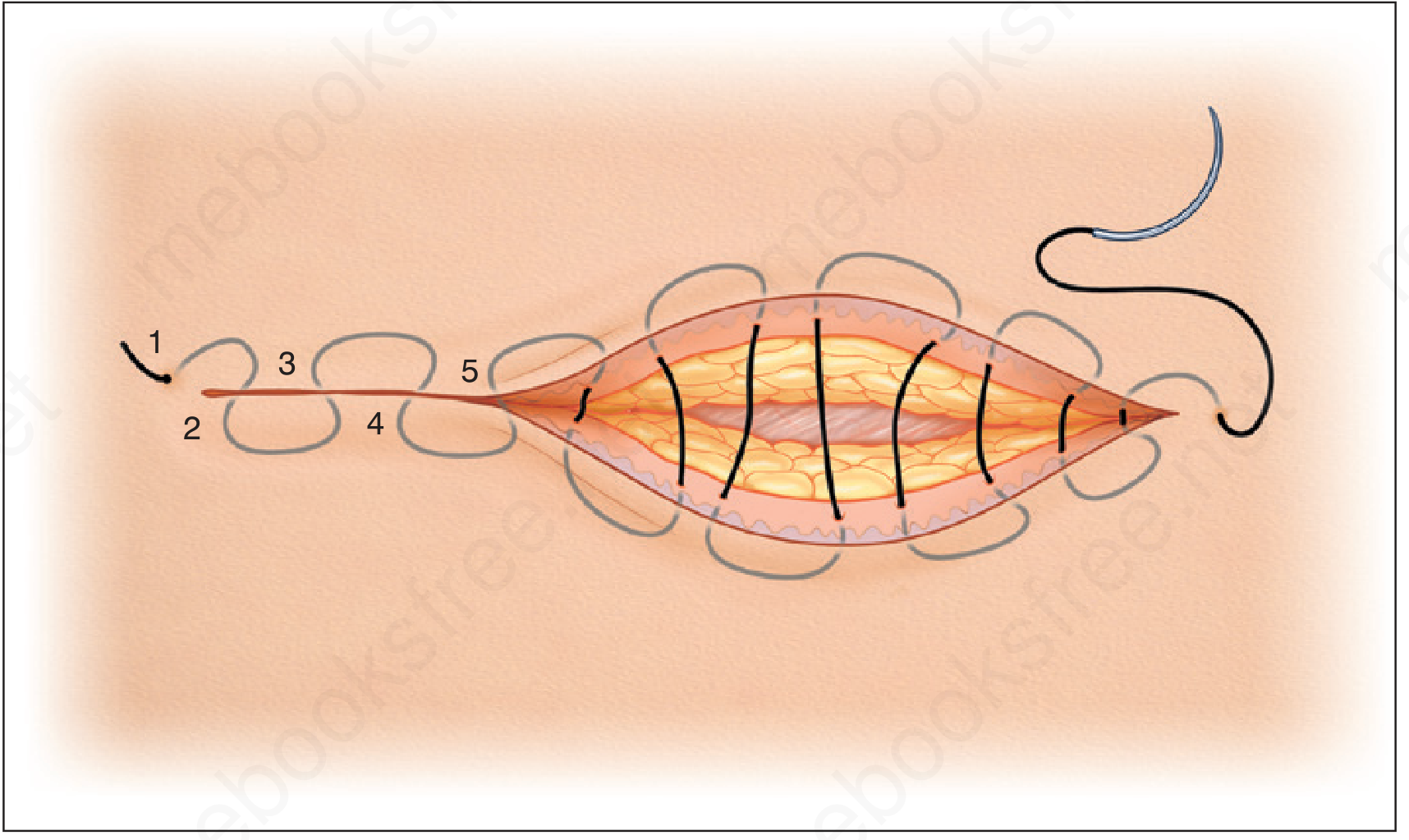
9. Running Subcuticular (Intradermal) Suture
Technique:
- The suture runs horizontally through the dermis just below the epidermis, alternating sides
- The needle enters the wound from one end (parallel to the incision), takes horizontal bites in the dermis alternating between sides, and exits at the far end
- No visible suture crosses the skin surface
Characteristics:
- No "railroad track" or cross-hatch marks from suture penetration
- Can remain in place for 2-3 weeks without scarring
- If a single loop comes out in the middle of a long wound, it facilitates removal
- Absorbable suture eliminates the need for removal entirely
Uses:
- Cosmetically sensitive wounds (face, neck, chest)
- Trunk and extremity closures where sutures must stay 2-3 weeks
- Patients who cannot easily return for suture removal
- Post-surgical incision closure in elective procedures
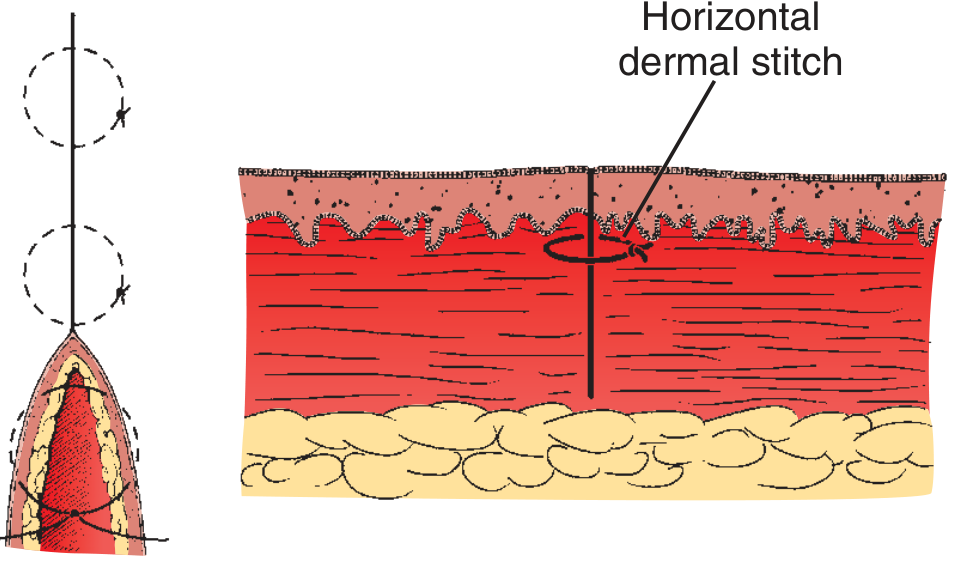
10. Interrupted Subcuticular (Horizontal Dermal) Suture
Technique:
- Individual horizontal bites within the dermis on alternating sides, each tied separately
- The knot is buried beneath the skin surface
Characteristics:
- Provides dermal support without surface penetration
- More flexible than running subcuticular - each bite is independent
- Suitable for wounds with strong static skin tension
Uses:
- Deep dermal closure for wounds requiring prolonged support
- Areas where running subcuticular would fail due to high tension
- Layered wound closure in areas prone to dehiscence
GROUP 3: VISCERAL / BOWEL SUTURES
Used specifically for hollow organs (bowel, bladder, stomach) to achieve watertight closure.
11. Lembert Suture (Inverting)
Technique:
- The needle enters the serosal surface, passes through the muscular layer and into (but not through) the submucosa, then exits the serosa on the same side
- Crosses the anastomosis and mirrors the same bite on the opposite side
- When tied, it inverts (tucks inward) the bowel wall, bringing serosa to serosa
Characteristics:
- The first reliable intestinal suture technique in surgical history
- Achieves serosal apposition - the strongest healing interface in bowel
- Does not penetrate the mucosa - prevents luminal contents from contacting the suture
- Can be used as interrupted or continuous
Uses:
- Bowel anastomosis (intestinal continuity restoration)
- Closure of bowel ends
- Second-layer (serosal) reinforcing suture over a mucosal closure
- Any hollow organ requiring inverting seromuscular repair
Source: Hinman's Atlas of Urologic Surgery, p.35
12. Connell Suture (Inverting, Mucosal)
Technique:
- A continuous suture that enters the bowel from the outside, passes through all layers including mucosa, crosses the lumen, and takes mirror bites on the opposite wall
- The bites are taken in a U-shape pattern, inverting the inner wall
Characteristics:
- Inverts the inner (mucosal) wall of the bowel
- May include mucosa and submucosa only (inner layer only)
- Particularly useful for closing the angles of a bowel anastomosis
Uses:
- Inner layer of a two-layer bowel anastomosis
- Closing angles of bowel anastomosis (corner stitches)
- Bowel closure when mucosa-to-mucosa approximation is desired with inversion
- Bladder and ureter repairs
Source: Hinman's Atlas of Urologic Surgery, p.34
13. Cushing Suture
Technique:
- A continuous inverting suture similar to Lembert but placed parallel to the bowel edge rather than crossing it perpendicularly
- The suture runs parallel to the wound, with each bite taken parallel to the incision line
Characteristics:
- Creates a waterproof serosal layer over a mucosal closure
- Less inverting than Lembert - takes only serosal and muscular layers
- Produces a smooth, continuous serosal surface
Uses:
- Second-layer reinforcing closure over a bowel anastomosis
- Gastric and intestinal closures requiring a watertight serosal seal
- Closure of the appendix stump
14. Purse-String Suture
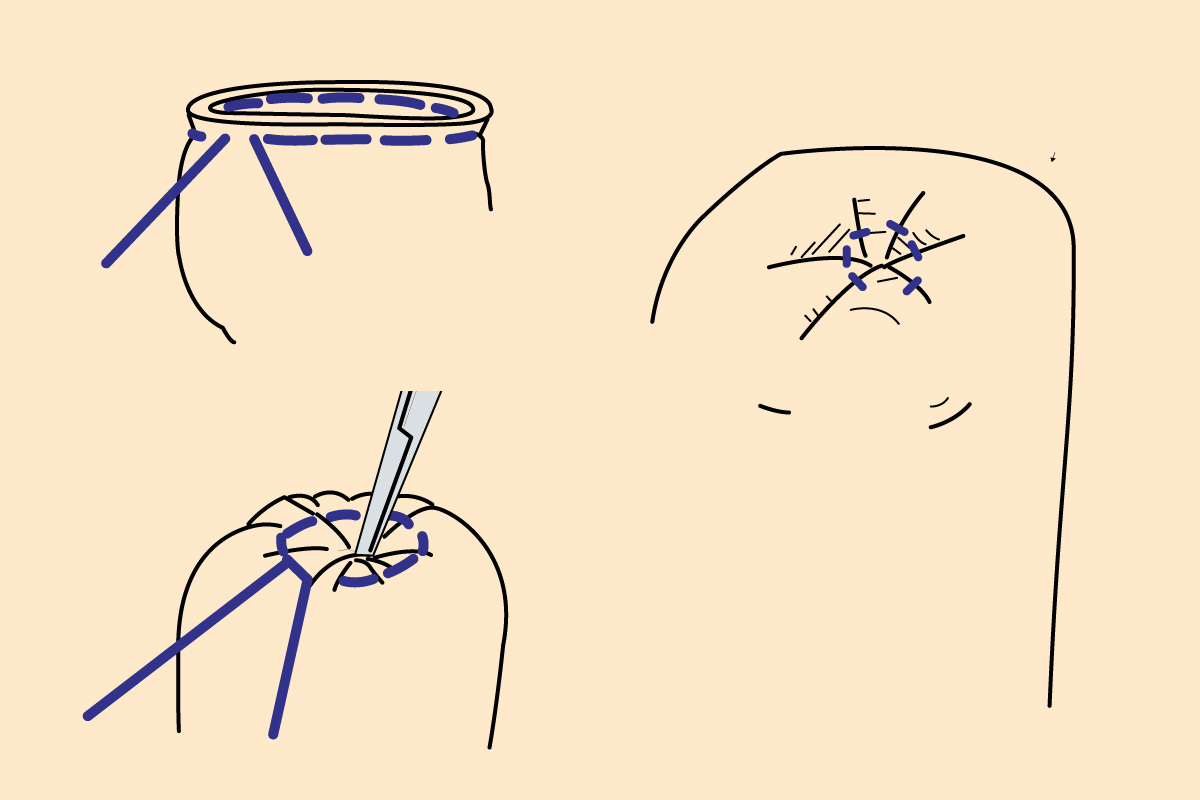
Technique:
- A continuous suture placed circumferentially around the perimeter of a circular opening or defect
- When pulled tight, the edges pucker and close concentrically like the mouth of a drawstring bag
Characteristics:
- Closes a circular defect without creating a linear incision
- Can partially or completely close depending on how tightly it is pulled
- The degree of closure depends on tissue laxity and defect size
Uses:
- Inverting the appendix stump (appendectomy)
- Closing hernia sacs circumferentially
- Partial or complete closure of circular skin defects to reduce healing time (allows second-intention healing for the remainder)
- Securing ostomy appliances and tubes (e.g., gastrostomy, colostomy)
- Rectal prolapse repair
Source: Hinman's Atlas of Urologic Surgery, p.35
15. Lock-Stitch Suture
Technique:
- A continuous suture where every 3rd or 4th bite passes under the previous stitch rather than looping over it
- Creates a locking chain effect along the mucosal edge
Characteristics:
- Prevents puckering of mucosal edges
- Distributes tension more evenly than a simple running suture along mucosal surfaces
Uses:
- Mucosal edges in bowel anastomosis
- Situations where puckering of the anastomosis must be avoided
- Oral mucosal closure
Source: Hinman's Atlas of Urologic Surgery, p.35
16. Figure-Eight Bowel Suture
Technique:
- Used specifically for interrupted bowel wall closure
- The needle takes a bite on one side, crosses diagonally, takes a bite on the other side, then recrosses back to the starting side - creating a figure-8 pattern through the bowel wall
Uses:
- Interrupted closure of bowel wall
- Provides strong individual approximating bites without continuous suture risk
Quick Summary Table
| Suture | Type | Layer | Primary Use |
|---|---|---|---|
| Simple Interrupted | Interrupted | Skin | Universal skin closure |
| Buried (Deep Dermal) | Interrupted | Dermis/SQ | Deep layer support, wound eversion |
| Vertical Mattress | Interrupted | Full thickness | Eversion, high-tension wounds |
| Horizontal Mattress | Interrupted | SQ/skin | Tension relief, retention |
| Figure-of-Eight | Interrupted | Fascia/skin | Fascia, tendons, high tension |
| Far-and-Near (Smead-Jones) | Interrupted | Full abdominal wall | Laparotomy mass closure |
| Simple Running | Continuous | Skin/peritoneum | Long low-tension wounds |
| Running Locked | Continuous | Skin/mucosa | Hemostasis, vascular areas |
| Running Subcuticular | Continuous | Intradermal | Cosmetic closure, no stitch marks |
| Interrupted Subcuticular | Interrupted | Intradermal | High-tension dermal support |
| Lembert | Interrupted/Continuous | Seromuscularis | Bowel anastomosis (outer layer) |
| Connell | Continuous | Mucosa/submucosa | Bowel anastomosis (inner layer) |
| Cushing | Continuous | Seromuscularis | Bowel anastomosis (waterproofing) |
| Purse-String | Continuous | Circumferential | Appendix stump, circular defects |
| Lock-Stitch | Continuous | Mucosa | Bowel/mucosal edges, no puckering |
| Figure-Eight Bowel | Interrupted | Full bowel wall | Interrupted bowel closure |
Sources: Roberts and Hedges' Clinical Procedures in Emergency Medicine (9780323354783); Andrews' Diseases of the Skin - Clinical Dermatology (9780323547536); Hinman's Atlas of Urologic Surgery (9780128016480); Fitzpatrick's Dermatology (9780071837781)
This is a shared conversation. Sign in to Orris to start your own chat.