Deltoid ligament orthopaeic 10 marks pg answer
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have all the content needed for a comprehensive 10-mark orthopaedic answer. Let me compile it:
Deltoid Ligament - Orthopaedics (10 Marks)
Introduction
The deltoid ligament (medial collateral ligament of the ankle) is a large, strong, triangular-shaped ligament on the medial side of the ankle joint. It is the primary stabilizer of the medial ankle during stance phase of gait.
Anatomy
Proximal attachment: Apex attached to the medial malleolus (anterior colliculus, intercollicular groove, and posterior colliculus).
Distal attachment: Broad base fans out to the navicular, talus, and calcaneus.
The ligament is organized into two layers - superficial and deep - comprising five components in total:
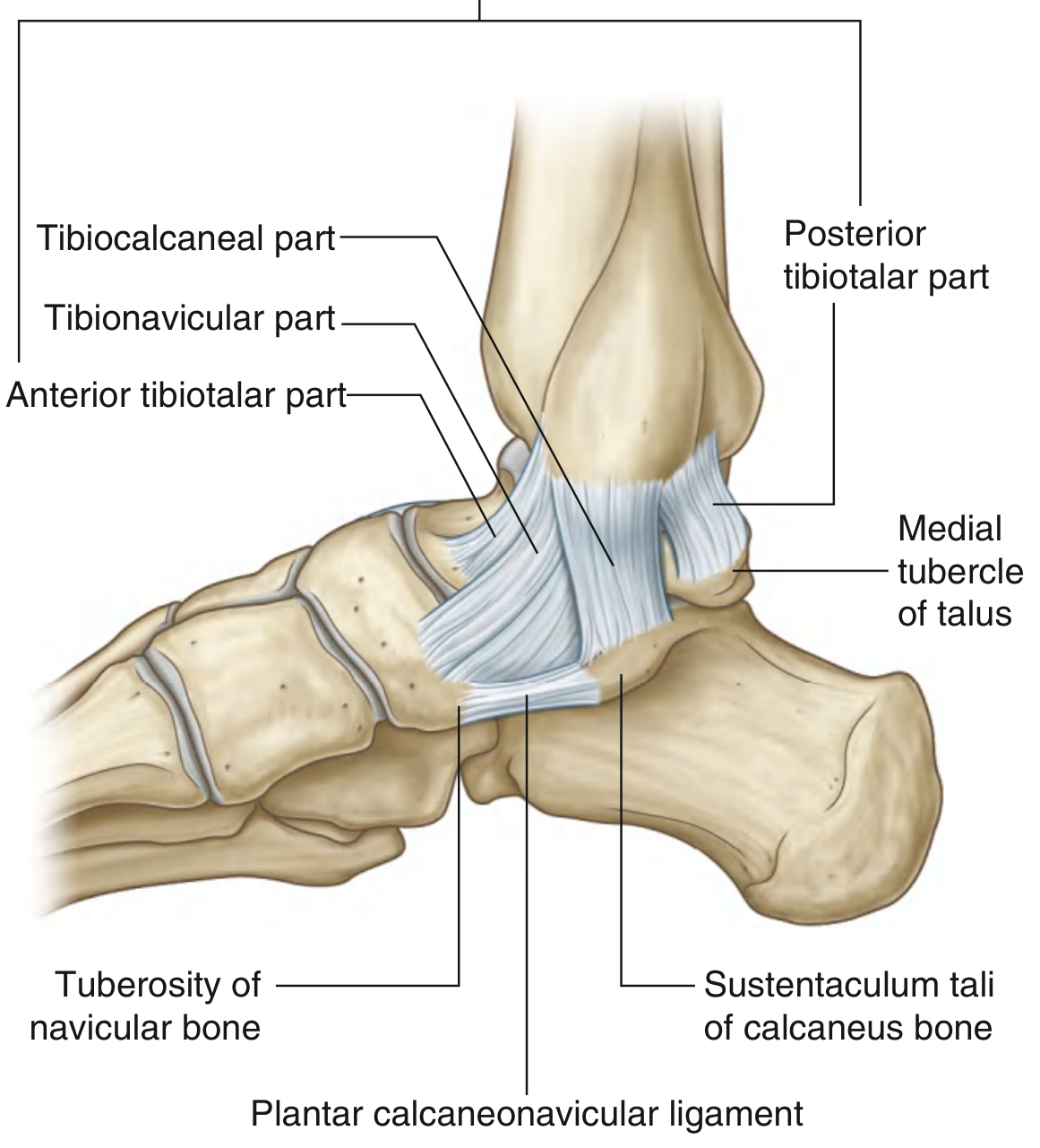
Fig. - Medial Ligament (Deltoid Ligament) of the Ankle Joint - Gray's Anatomy for Students
Superficial Layer (3 components)
| Component | Proximal Attachment | Distal Attachment | Function |
|---|---|---|---|
| Tibionavicular | Anterior medial malleolus | Tuberosity of navicular + spring ligament | Resists eversion / valgus tilt |
| Tibiocalcaneal | Medial malleolus (central) | Sustentaculum tali of calcaneus | Resists valgus tilt, eversion |
| Posterior superficial tibiotalar | Posterior medial malleolus | Medial surface of talus | Resists valgus / eversion |
Deep Layer (2 components)
| Component | Attachment | Function |
|---|---|---|
| Anterior deep tibiotalar | Undersurface of medial malleolus → medial talar body | Resists lateral talar translation + external rotation |
| Posterior deep tibiotalar | Undersurface of medial malleolus → medial talar body | Strongest component - primary restraint vs. lateral translation and external rotation |
Key point: Both deep components are intraarticular but extrasynovial. The posterior deep tibiotalar ligament is the strongest of the entire complex.
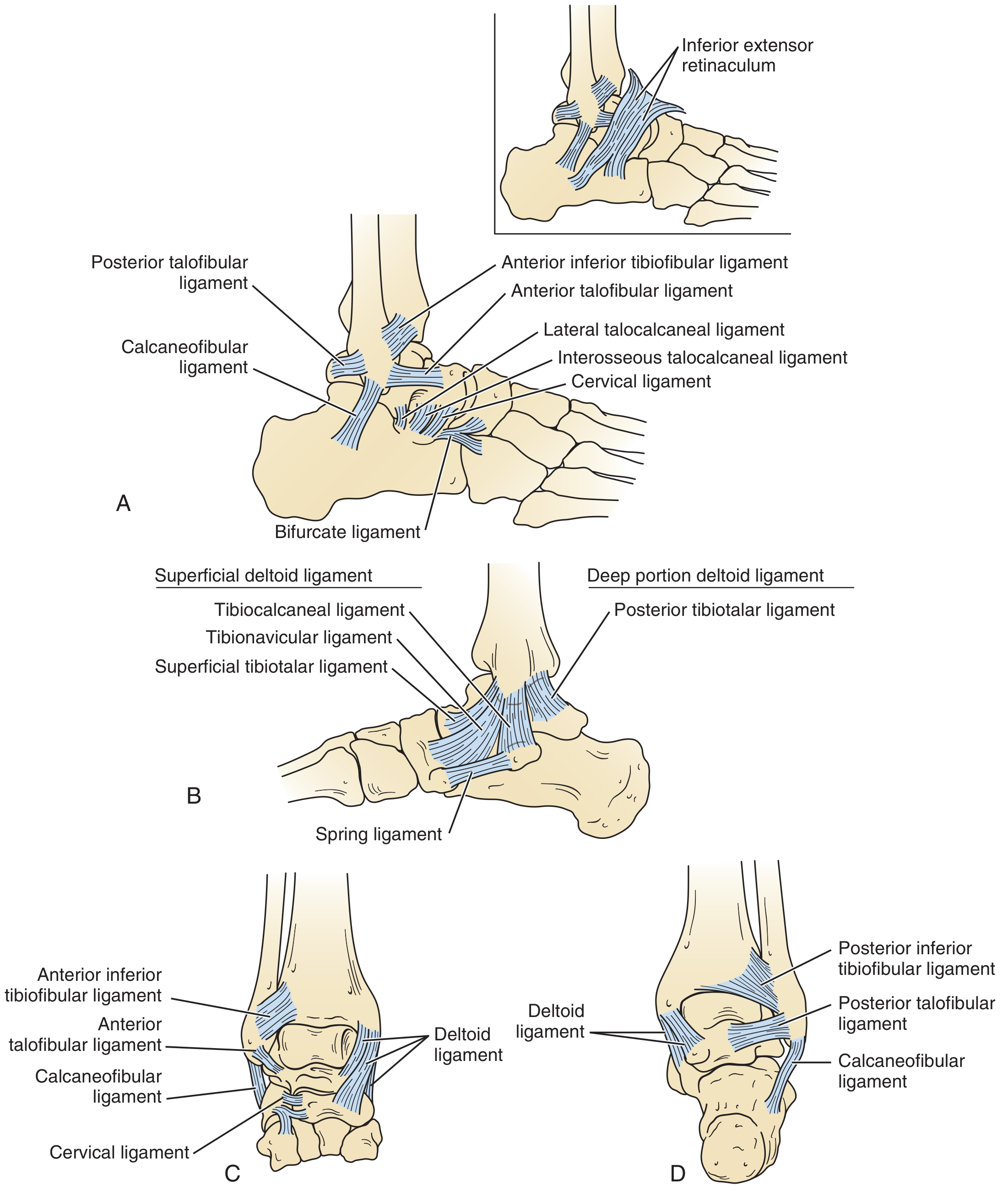
Fig. - Ligaments of the ankle and subtalar joint. (B) Medial view showing superficial and deep deltoid components.
Functions
- Primary ankle stabilizer during the stance phase of gait.
- Deep deltoid: resists lateral talar translation and external rotation of the talus.
- Superficial deltoid: resists valgus tilting (eversion) of the talus.
- Both layers act as secondary restraints against anterior translation of the talus.
- Prevents lateral displacement of the talus in the ankle mortise - a 1 mm lateral shift reduces tibiotalar weight-bearing area by 20-40%; a 5 mm shift reduces it by 80%.
Mechanism of Injury
- Deltoid ligament tears occur via supination + external rotation mechanism (same as bimalleolar fractures).
- Instead of fracturing the medial malleolus, the deltoid ligament tears, allowing the talus to displace laterally.
- 72% of patients with lateral ankle instability have concurrent deltoid ligament injury.
- 43% have injuries to both deep and superficial components.
- Deltoid lesion incidence significantly increases with complete rupture of the anterior talofibular ligament (ATFL).
Clinical Features
- Medial ankle pain, swelling, tenderness, hematoma after ankle sprain or ankle fracture.
- Isolated complete deltoid rupture is rare - isolated partial ruptures are more common.
- Suspect deltoid tear when a lateral malleolar fracture is accompanied by medial-sided tenderness and swelling (bimalleolar equivalent injury).
Note: No statistically significant relationship has been found between medial tenderness alone and deep deltoid ligament rupture.
Investigations
Radiographs:
- Routine AP may appear normal.
- Stress radiograph (supination + external rotation, ankle in neutral): shows medial clear space widening >4 mm and lateral talar shift in the mortise.
- Gravity external rotation stress radiograph is an alternative.
- Must be done in neutral (not plantarflexion) - plantarflexion brings the narrow part of talus into mortise and may give false widening.
MRI:
- Gold standard to determine extent and location of medial ankle ligament complex injury.
- Comparison MRI of the opposite ankle can be helpful.
Classification / Associated Injuries
- Concomitant pathology almost always present:
- Lateral ligamentous injury (ATFL, CFL)
- Lateral malleolar fracture
- Osteochondral injuries (medial talar dome)
- Distal tibiofibular syndesmotic disruption
Treatment
Non-operative
- Isolated complete disruption: below-knee non-weight-bearing cast for 6 weeks.
- Carefully monitor radiographically for displacement.
- Non-operative management: 1-year functional outcomes equivalent to ORIF of stress-positive fractures; however, risks include residual medial clear space widening and lateral malleolar delayed/non-union.
Operative (ORIF + Deltoid Repair)
Indications:
- Unstable ankle (positive anterior drawer or talar tilt clinically and radiographically).
- Active patients with complete rupture demonstrated on MRI or abnormal talar tilt/shift.
- Wide medial clear space with delayed presentation (ligament may be interposed).
Key principle: If only the fibular fracture is fixed without addressing the deltoid, the ligament may be caught between the medial malleolus and talus (preventing reduction) or relax after healing.
Technique (Technique 59.3 - Campbell's):
- Anteromedial curved incision distal to the medial malleolus.
- Identify the deltoid ligament and clear any interposed tissue from the mortise.
- ORIF of fibula is performed first.
- Repair deltoid ligament with primary suture or suture anchor to its native attachment.
- Many surgeons advocate fibular fixation without routine medial exploration - explore only when reduction is blocked.
Good results have been reported in high-performance athletes after direct repair (approximating the tibionavicular and tibiocalcaneal portions to their native attachment on the medial malleolus).
Deltoid Ligament Reconstruction (Chronic Insufficiency)
- Indicated in select patients with:
- Flexible, reducible deformity
- Less than 10 degrees tibiotalar tilt
- Minimal lateral ankle arthrosis
- Minimally invasive allograft technique (Jeng-Bluman-Myerson): uses tibial tunnel + talar tunnel + sustentaculum tali tunnel with biotenodesis screws.
Summary Table
| Feature | Detail |
|---|---|
| Shape | Triangular, flat |
| Layers | Superficial (3 components) + Deep (2 components) |
| Strongest component | Posterior deep tibiotalar ligament |
| Deep layer location | Intraarticular, extrasynovial |
| Primary function | Medial ankle stability; resist lateral talar translation + eversion |
| Injury mechanism | Supination + external rotation |
| Key radiological sign | Medial clear space >4 mm on stress view |
| Best imaging | MRI |
| Treatment | Cast (isolated) / ORIF ± repair (with fracture) / Reconstruction (chronic) |
Sources:
- Campbell's Operative Orthopaedics, 15th Ed. 2026, Chapter 94 (Ankle Ligaments) and Chapter 59 (Ankle Fractures)
- Miller's Review of Orthopaedics, 9th Edition, Ankle Anatomy
- Gray's Anatomy for Students, Medial Ligament of the Ankle
This is a shared conversation. Sign in to Orris to start your own chat.