Physiology of reproduction
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have excellent comprehensive content from multiple authoritative textbooks. Let me compile this into a thorough response.
Physiology of Reproduction
Reproduction physiology covers the hormonal axes, gametogenesis, cyclical changes, fertilization, and pregnancy. Below is a structured overview drawing from Guyton & Hall Textbook of Medical Physiology, Ganong's Review of Medical Physiology, and Costanzo Physiology.
1. Hypothalamic-Pituitary-Gonadal (HPG) Axis
The HPG axis governs both male and female reproductive function:
- The hypothalamus secretes GnRH (Gonadotropin-releasing hormone) in a pulsatile fashion.
- GnRH acts on the anterior pituitary gonadotropes to stimulate release of LH (luteinizing hormone) and FSH (follicle-stimulating hormone) - both glycoproteins.
- LH and FSH act via cAMP second messenger systems on gonadal target cells.
- In the absence of GnRH, the pituitary secretes virtually no LH or FSH.
2. Male Reproductive Physiology
Testicular Structure and Function
The testes serve two functions: spermatogenesis (in seminiferous tubules) and steroidogenesis (testosterone from Leydig cells).
- Leydig cells (interstitial cells) produce testosterone when stimulated by LH.
- Sertoli cells (inside seminiferous tubules) support spermatogenesis when stimulated by FSH and testosterone.
Spermatogenesis
Spermatogenesis begins at puberty and continues throughout life:
- Spermatogonia (stem cells) undergo mitosis.
- Primary spermatocytes undergo meiosis I → secondary spermatocytes.
- Meiosis II → spermatids, which undergo spermiogenesis to form spermatozoa.
- The entire process takes approximately 64-74 days.
Regulation: Both FSH (acting on Sertoli cells) and testosterone (diffusing from Leydig cells) are necessary to initiate and maintain spermatogenesis. FSH causes Sertoli cells to grow and secrete spermatogenic substances.
Inhibin feedback: When spermatogenesis is excessive, Sertoli cells secrete inhibin, a glycoprotein that directly inhibits pituitary FSH secretion - providing negative feedback control. - Guyton & Hall, p. 1008
Testosterone
Secretion: Testosterone is secreted by Leydig cells in direct proportion to available LH.
Negative feedback: Testosterone inhibits the hypothalamus (decreasing GnRH) and the anterior pituitary (decreasing LH/FSH) - classic negative feedback loop.
Effects of testosterone:
| Domain | Effect |
|---|---|
| Fetal development | Drives male genital tract formation; suppresses female organ formation; promotes testicular descent |
| Puberty | Enlargement of penis, scrotum, testes (~8-fold) |
| Secondary sex characteristics | Pubic/facial/body hair, voice deepening (laryngeal hypertrophy), increased skin thickness, sebum secretion |
| Anabolic effects | Increased muscle mass and protein synthesis, RBC production (via erythropoietin) |
| Bone | Growth spurt at puberty; epiphyseal closure |
| Libido | Maintenance of sexual drive |
Male Sexual Act
- Erection: Parasympathetic (sacral S2-4) impulses cause release of nitric oxide and VIP → activates guanylyl cyclase → increased cGMP → smooth muscle relaxation in corpora cavernosa → vasodilation and engorgement.
- Emission: Sympathetic (T12-L2) impulses cause vas deferens, ampulla, prostate, and seminal vesicles to contract, propelling sperm and seminal fluid into the urethra.
- Ejaculation: Rhythmic contractions of bulbocavernosus and ischiocavernosus muscles expel semen. - Guyton & Hall, p. 1004
3. Female Reproductive Physiology
Functional Anatomy
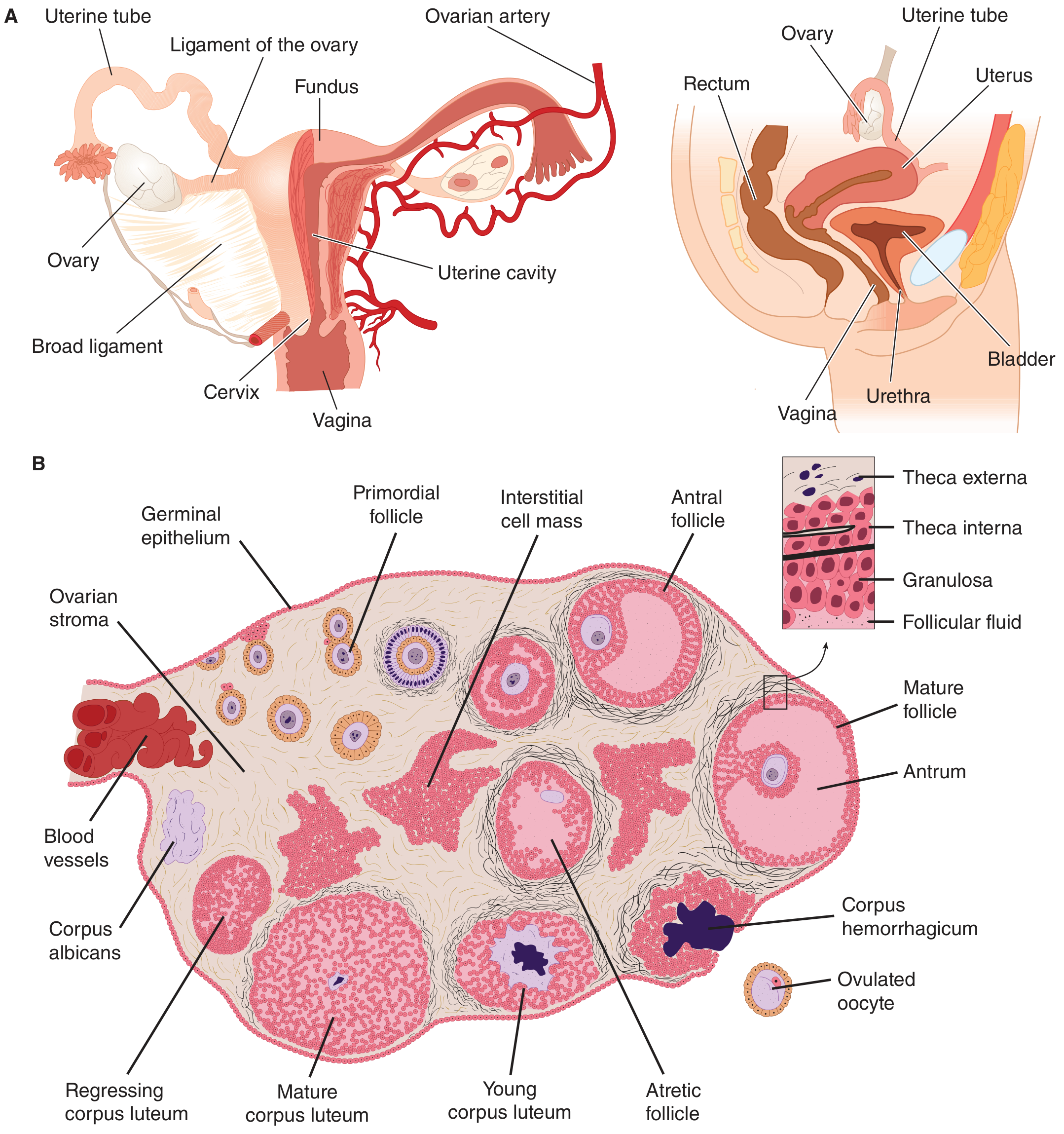
Female reproductive anatomy with ovarian cycle stages (Ganong's Review of Medical Physiology)
The Menstrual Cycle (28-day reference)
The menstrual cycle represents periodic preparation for fertilization. Its most visible feature is periodic vaginal bleeding from shedding of the uterine mucosa.
Two-Cell Theory of Estrogen Synthesis
- Theca interna cells respond to LH → secrete androgens (androstenedione, testosterone)
- Granulosa cells respond to FSH → aromatize those androgens to estrogens (estradiol)
Ovarian Cycle
Follicular Phase (Days 1-14):
- Multiple primordial follicles begin to enlarge at cycle start.
- By day 6, one dominant (Graafian) follicle is selected; others undergo atretic apoptosis.
- The dominant follicle grows, fills with follicular fluid (antrum formation), and is the main source of circulating estradiol.
- Rising estradiol causes positive feedback on the pituitary → LH surge.
Ovulation (~Day 14):
- The LH surge triggers follicular rupture ~9 hours after the LH peak.
- The ovum is extruded into the peritoneal cavity and picked up by the fimbriated ends of the fallopian tube.
- Minor bleeding into the peritoneal cavity may cause mittelschmerz (mid-cycle pain).
- The ovum is fertilizable for ~24 hours (lives up to 72 hours after extrusion).
Luteal Phase (Days 14-28):
- The ruptured follicle fills with blood (corpus hemorrhagicum), then granulosa/theca cells proliferate and differentiate into lipid-rich luteal cells → corpus luteum.
- Corpus luteum secretes estrogen + progesterone (dominant hormone of luteal phase).
- If no pregnancy: corpus luteum regresses → corpus albicans → hormone withdrawal → menstruation.
- If pregnancy occurs: hCG from the embryo rescues the corpus luteum, which persists until the placenta takes over steroid production (~weeks 8-12).
Hormonal Changes Across the Cycle
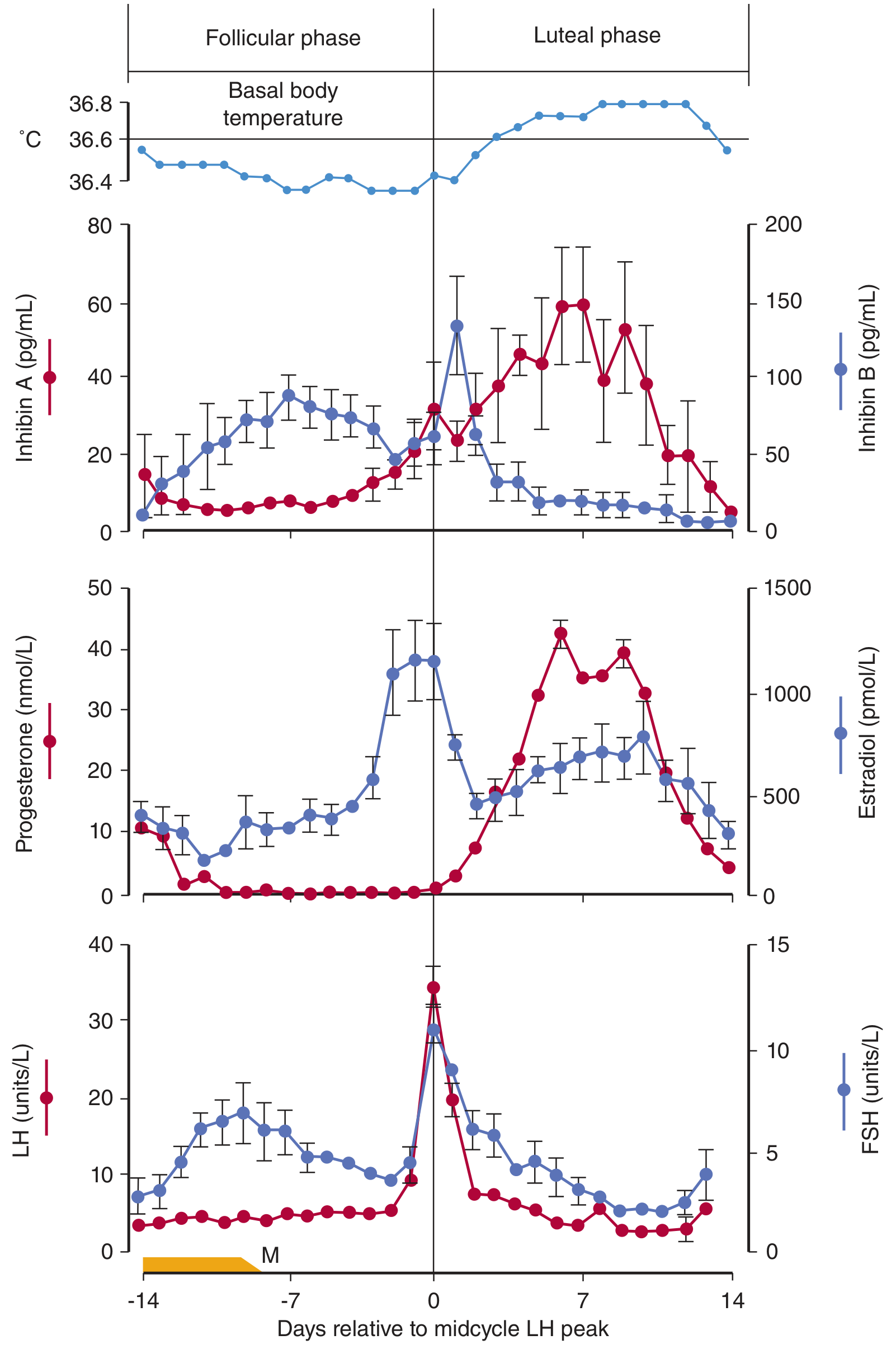
Menstrual cycle hormone profile aligned to midcycle LH peak. Note LH surge triggering ovulation, progesterone rise in luteal phase, and basal body temperature increase. (Ganong's Review of Medical Physiology)
| Parameter | Follicular Phase | Luteal Phase |
|---|---|---|
| Dominant hormone | Estradiol | Progesterone |
| FSH | Rises early, falls mid-cycle | Low |
| LH | Rises to surge at day 14 | Low |
| Endometrium | Proliferative (growth of glands, stroma, spiral arteries) | Secretory (tortuous glands, glycogen vacuoles, edematous stroma) |
| Cervical mucus | Copious, watery, elastic - "ferning" pattern | Thick, non-elastic, does not fern |
| Basal body temperature | Low | Elevated (~0.2-0.5°C rise, due to progesterone thermogenesis) |
Uterine (Endometrial) Cycle
- Menstruation (Days 1-5): Progesterone/estrogen withdrawal → spiral artery spasm → ischemia → endometrial shedding.
- Proliferative phase (Days 6-14): Estradiol drives regrowth of endometrium, glands, stroma, and spiral arteries.
- Secretory phase (Days 15-28): Progesterone causes glands to become tortuous, glycogen-laden, and secretory; prepares endometrium for implantation.
Effects of Estrogen and Progesterone
Estrogen:
- Proliferation of endometrium, ductal growth in breasts
- Puberty: growth spurt, epiphyseal closure, female fat distribution, breast development
- Positive feedback at high levels → LH surge
- Increases prolactin secretion
- Stimulates myometrial growth
Progesterone:
- Maintains secretory endometrium for implantation
- Raises uterine threshold to contractile stimuli (preserves pregnancy)
- Thermogenic (raises basal body temperature - basis of rhythm method)
- Reduces quantity and elasticity of cervical mucus post-ovulation
- Stimulates lobular/alveolar development in breast
4. Puberty
Both sexes: onset triggered by increased pulsatile GnRH secretion from the hypothalamus.
- Girls: Average onset 8-13 years; estrogen drives thelarche (breast development) → adrenarche → menarche.
- Boys: Average onset 9-14 years; testosterone drives testicular enlargement → pubic hair → voice change → spermarche.
5. Fertilization and Early Pregnancy
- Fertilization typically occurs in the ampulla of the fallopian tube.
- The fertilized egg (zygote) undergoes cleavage during transport to the uterus (~3-4 days).
- Implantation occurs at days 6-10 post-fertilization in the secretory endometrium.
- The syncytiotrophoblast immediately begins secreting hCG, which maintains the corpus luteum and prevents menstruation.
- In mid-to-late pregnancy, the placenta takes over synthesis of estrogen and progesterone.
- Estrogen stimulates myometrial growth; progesterone raises the uterine contractile threshold and preserves pregnancy.
6. Indicators of Ovulation
- Basal body temperature (BBT): Rises 1-2 days after ovulation due to progesterone thermogenesis; useful retrospectively.
- Cervical mucus: Changes from ferning/elastic (follicular) to thick/non-elastic (post-ovulation).
- LH surge detection: Urine LH kits detect the surge ~24-36 hours before ovulation.
- Progesterone level: Mid-luteal progesterone >3 ng/mL confirms ovulation.
Summary Diagram of HPG Axis
Hypothalamus
↓ GnRH (pulsatile)
Anterior Pituitary
↓ LH ↓ FSH
Leydig cells (♂) Sertoli cells / Granulosa cells (♀)
↓ Testosterone ↓ Estrogen / Progesterone
↑ Negative feedback (–) to hypothalamus & pituitary
↑ Positive feedback (+) from high estradiol → LH surge (♀)
Sources:
- Guyton and Hall Textbook of Medical Physiology, pp. 1004-1010
- Ganong's Review of Medical Physiology, 26th ed., pp. 404-410
- Costanzo Physiology, 7th ed., pp. 479-482
This is a shared conversation. Sign in to Orris to start your own chat.