Neuromuscular monitoring in anaesthesia
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Searching PubMed
neuromuscular monitoring residual blockade quantitative
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
I now have comprehensive content from Miller's Anesthesia and Barash's Clinical Anesthesia. Let me compile the full answer.
Neuromuscular Monitoring in Anaesthesia
Neuromuscular monitoring is used to assess the degree of neuromuscular blockade (NMB) at the neuromuscular junction, guide dosing of neuromuscular blocking drugs (NMBDs) and their reversal agents, and confirm adequate recovery before extubation. Without monitoring, residual paralysis affects up to 30-40% of patients reversed with neostigmine.
1. Why Monitor?
Neuromuscular blocking drugs do NOT alter consciousness or cause amnesia - only paralysis. Because of highly significant interpatient variability in response to all NMBDs, time from last administration or clinical signs alone cannot reliably exclude residual block. Studies show:
- 8.4% of patients had TOF ratio <0.80 even 4 hours after a single intubating dose of vecuronium
- 37% of patients had TOF ratio <0.90 when tested ≥2 hours after rocuronium, vecuronium, or atracurium (Debaeene et al.)
- 21% of patients given a single 1×ED95 rocuronium dose still had not recovered to TOF ratio ≥0.90 by the end of surgery despite a mean case duration of 161 minutes
- Barash, Clinical Anesthesia 9e, p.1626; Miller's Anesthesia 10e, p.3403
2. Clinical Assessments - Why They Fail
Traditional clinical tests of recovery (5-second head lift, hand grip, tidal volume, inspiratory force) are all insensitive. The 5-second head lift - once regarded as the gold standard - was performed by 11/12 volunteers despite TOF ratio ≤0.5. Neither time from last dose nor physical tests should be used as the primary means to assess recovery.
- Barash, Clinical Anesthesia 9e, p.1627
3. Peripheral Nerve Stimulators (PNS) - Qualitative Monitoring
A PNS is a battery-operated device that delivers a square wave monophasic current of 10-80 mA for 100-300 microseconds to a peripheral motor nerve. Key technical points:
- The negative electrode (usually black) is placed distally, the positive electrode (usually red) proximally ("red toward the head")
- Proper skin preparation (cleansing + abrasion) reduces skin resistance from ~100,000 to <5,000 ohms
- Standard silver-silver chloride electrodes, ideally 7-8 mm diameter
- Must deliver at least 50 mA across a 1,000-ohm load for supramaximal stimulation
Most common sites:
- Ulnar nerve at the wrist → adductor pollicis and abductor digiti minimi (most commonly used)
- Facial nerve → orbicularis oculi
- Posterior tibial nerve → flexor hallucis brevis
Limitation: Clinicians using qualitative (visual/tactile) assessment cannot reliably detect fade when TOF ratio exceeds 0.30-0.40, making it impossible to exclude clinically significant residual block.
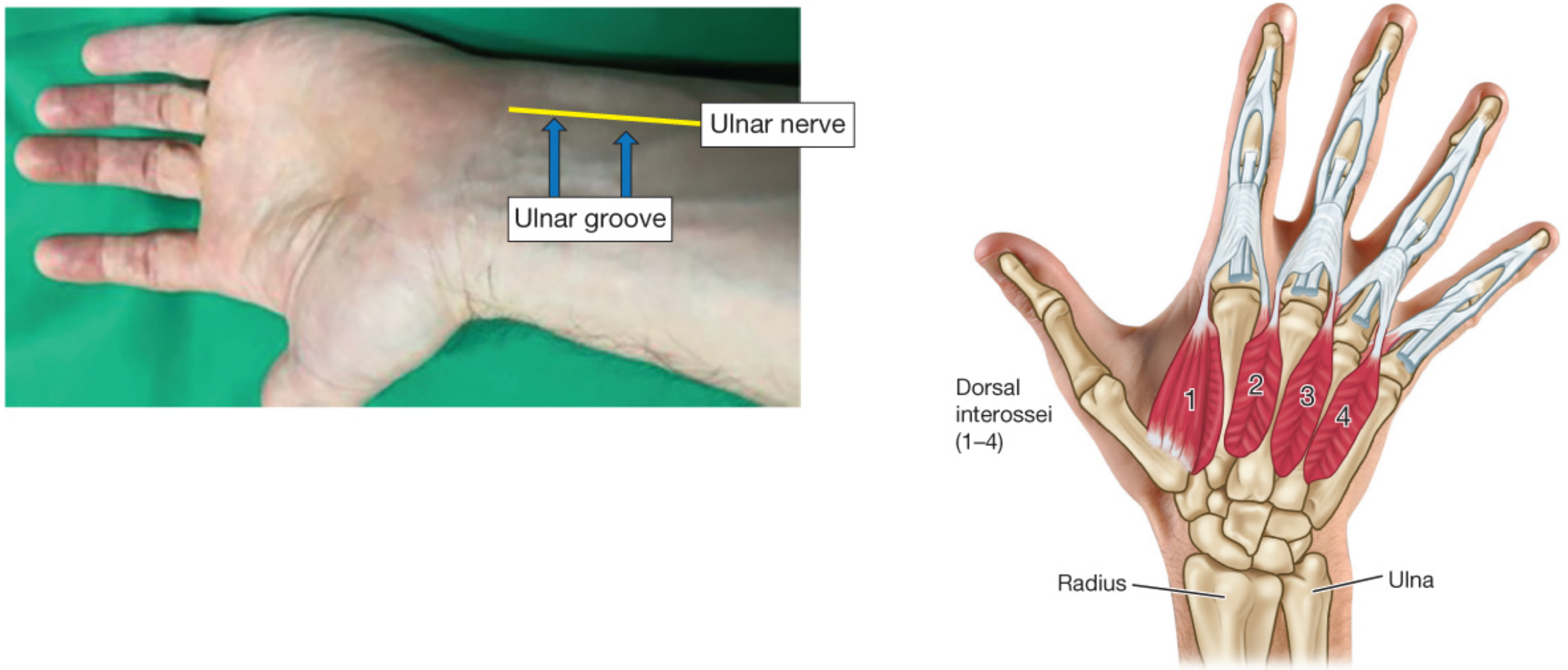
Figure: Ulnar nerve in the ulnar groove. The negative electrode is placed distally over the nerve. Palmar muscles innervated include the adductor pollicis and abductor digiti minimi.
- Barash, Clinical Anesthesia 9e, p.1628-1629; Morgan & Mikhail's Clinical Anesthesiology 7e, p.247
4. Patterns of Nerve Stimulation
4.1 Single Twitch (ST)
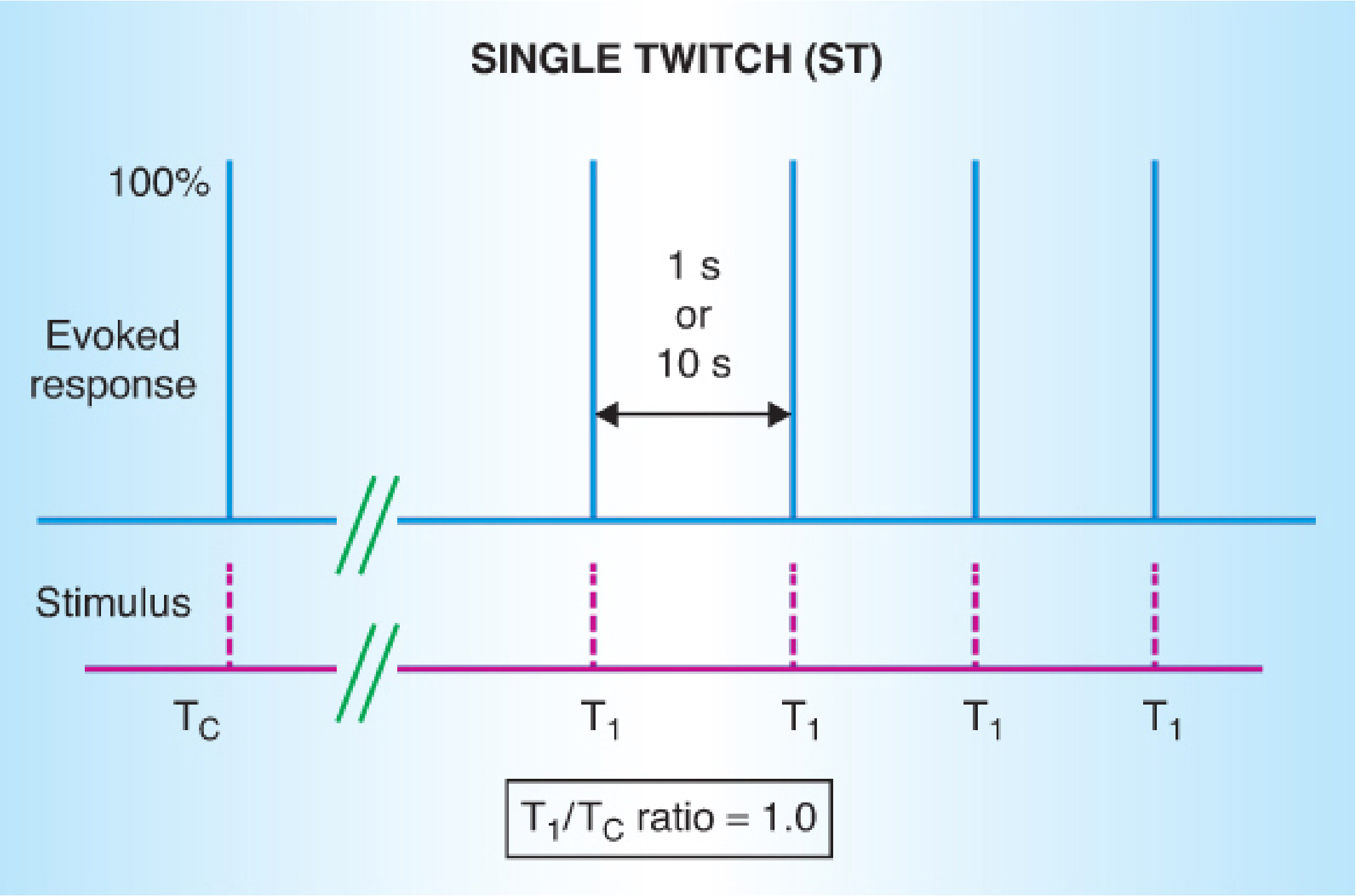
- Frequency: 0.1-1 Hz (1 stimulus per 1-10 seconds)
- Frequencies >0.1 Hz may cause muscle fatigue
- Useful only during onset of blockade - cannot detect fade, requires a pre-drug baseline twitch height for comparison
- A 25% reduction in twitch height = ~75% receptor occupancy needed for surgical relaxation
4.2 Train-of-Four (TOF) - The Clinical Standard
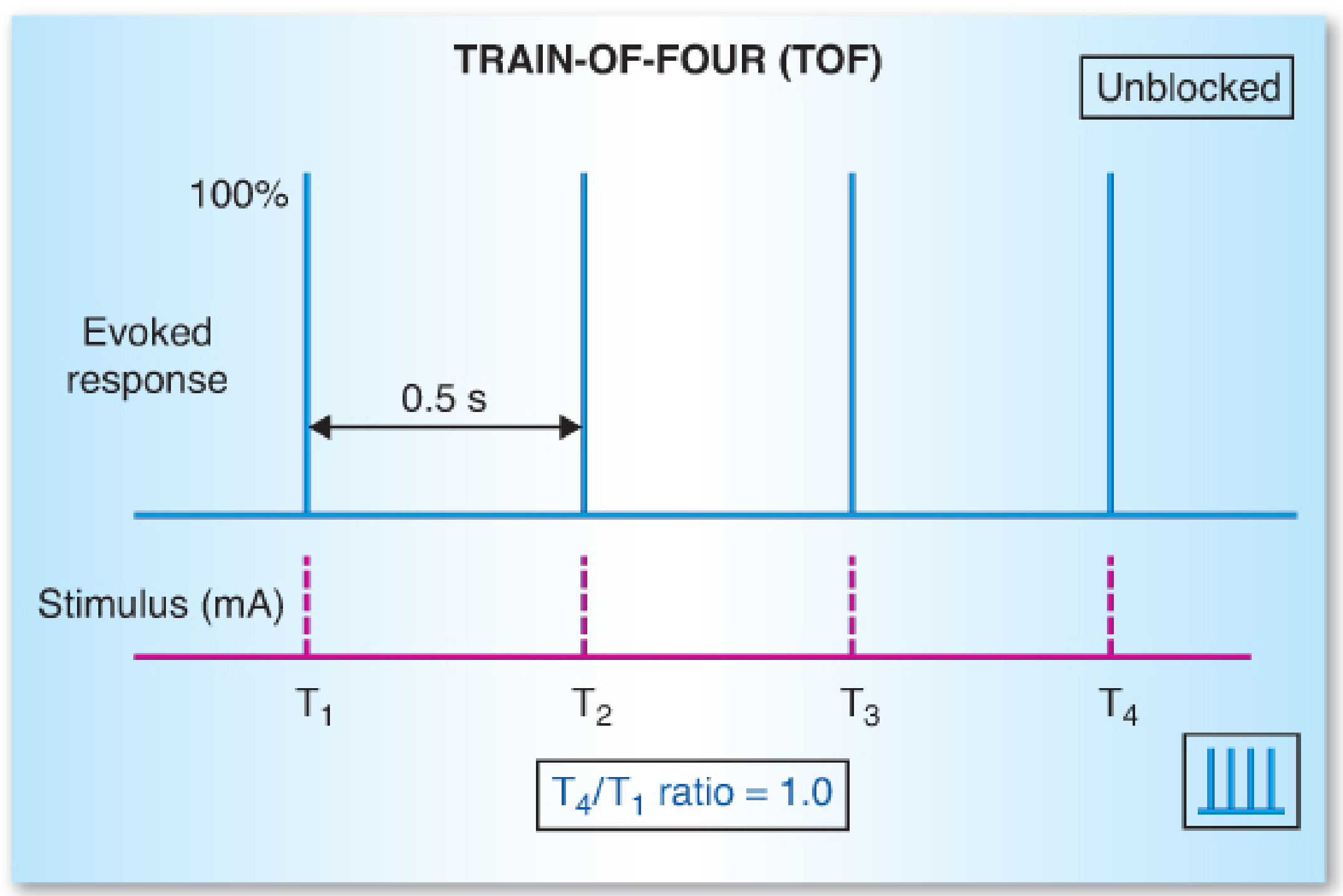
- Four successive 200-μs stimuli over 2 seconds at 2 Hz
- Can be repeated every 10-15 seconds without causing post-tetanic facilitation
- No baseline twitch needed - the ratio is self-referencing (T4/T1)
- TOF ratio = T4/T1 amplitude ratio (normally 1.0)
- With nondepolarizing block, the T4/T1 ratio progressively decreases (fade)
TOF Count correlates with depth of block:
| TOF Count | Approximate Receptor Occupancy | Clinical Correlation |
|---|---|---|
| 4 twitches present | 75% | Minimal/shallow block, clinical relaxation adequate |
| 3 twitches | 80% | Moderate-to-deep block |
| 2 twitches | ~85% | Deep block |
| 1 twitch | ~90% | Very deep block |
| 0 twitches | >90% | Profound block - use PTC |
Disappearance of the 4th twitch = ~75% block; 3rd twitch = 80% block; 2nd twitch = ~90% block. Surgical relaxation usually requires 75-95% blockade.
With depolarizing block (succinylcholine): all four twitches diminish equally with no fade (because acetylcholine receptors are occupied and depolarized rather than competitively blocked). The TOF ratio remains near 1.0 despite reduced absolute height.
- Barash, Clinical Anesthesia 9e, p.1629-1632; Morgan & Mikhail 7e, p.249
4.3 Tetanic Stimulation
- 50 Hz or 100 Hz sustained stimulus for 5 seconds
- Sustained contraction for 5 seconds indicates adequate (but not complete) reversal
- Very sensitive but painful in awake patients
- Post-tetanic potentiation: following tetanus, single twitch or TOF responses are temporarily enhanced - this is the basis of the Post-Tetanic Count
4.4 Post-Tetanic Count (PTC)
- Used when the TOF count is zero (profound block)
- Deliver a 50-Hz tetanic stimulus for 5 seconds, wait 3 seconds, then deliver single twitches at 1 Hz
- Count the number of single twitches after the tetanus
- PTC 1-2 = very deep block; PTC >10 = TOF count will return within minutes
| Depth of Block | TOF Count | PTC |
|---|---|---|
| Complete | 0 | 0 |
| Deep | 0 | ≥1 |
| Moderate | 1-3 | N/A |
| Shallow | 4 (TOF ratio <0.4) | N/A |
| Minimal | 4 (TOF ratio 0.4-0.9) | N/A |
| Recovered | 4 (TOF ratio ≥0.9) | N/A |
- Barash, Clinical Anesthesia 9e, p.1649-1650; Miller's Anesthesia 10e
4.5 Double-Burst Stimulation (DBS)
- DBS3,3: Three 50-Hz bursts separated by 20 ms, followed 750 ms later by another three bursts
- DBS3,2: Three 50-Hz bursts followed 750 ms later by two bursts
- More sensitive than TOF for visual/tactile detection of fade
- The DBS3,2 variant is most commonly used clinically
- Detects fade at higher TOF ratios than standard TOF when assessed by feel or sight
- Morgan & Mikhail 7e, p.251
5. Differential Muscle Sensitivity
Not all muscle groups recover at the same rate - this is critical for extubation decisions:
| Recovers EARLIER (more resistant) | Recovers LATER (more sensitive) |
|---|---|
| Diaphragm | Adductor pollicis (thumb) |
| Laryngeal adductors | Pharyngeal muscles |
| Orbicularis oculi | Genioglossus |
| Rectus abdominis | Upper airway muscles |
The adductor pollicis is the standard monitoring site but is more sensitive to NMBDs than the diaphragm, larynx, and upper airway muscles. This means when the thumb is showing full recovery (TOF ratio ≥0.9), airway muscles will have already recovered. Conversely, residual pharyngeal dysfunction may persist even when thumb twitch appears adequate on subjective assessment.
- Barash, Clinical Anesthesia 9e, p.1470; Morgan & Mikhail 7e, p.250
6. Quantitative (Objective) Monitoring
Quantitative monitoring precisely measures the evoked muscle response and calculates the TOF ratio automatically. It is the only reliable way to confirm full recovery.
Types of Quantitative Monitors
| Method | Mechanism | Notes |
|---|---|---|
| Mechanomyography (MMG) | Measures isometric muscle force directly | Gold standard/reference; requires immobilized limb setup; not practical clinically |
| Acceleromyography (AMG) | Piezoelectric crystal measures acceleration of thumb movement | Most common clinical device; thumb must be free to move; tends to overestimate TOF ratio vs MMG (bias +5-10%); goal TOF ratio for AMG ≥0.95-1.0 |
| Electromyography (EMG) | Measures compound muscle action potential | Fast onset, accurate, less affected by hypothermia; tends to underestimate vs MMG (bias -4.7%) |
| Kinemyography | Measures thumb bending via piezoelectric film | Less commonly used |
Key AMG bias issue: AMG values are consistently higher than MMG by ~5-10%. If the goal is TOF ratio ≥0.9 by MMG reference, the equivalent AMG value should be ≥0.95-1.0 to ensure true recovery. This is why normalized AMG (baseline calibrated) is preferred.
- Barash, Clinical Anesthesia 9e (Table 21-2), p.1579-1582
7. Residual Neuromuscular Block (RNMB)
Definition: TOF ratio <0.9 at the time of extubation or in the PACU.
Clinical consequences of TOF ratio <0.9:
- Impaired pharyngeal function and risk of aspiration
- Upper airway obstruction
- Impaired hypoxic ventilatory response
- Blurry vision, diplopia, facial weakness
- Inability to seal a mouthpiece; swallowing dysfunction
- Increased PACU length of stay and nursing interventions
- Increased postoperative pulmonary complications
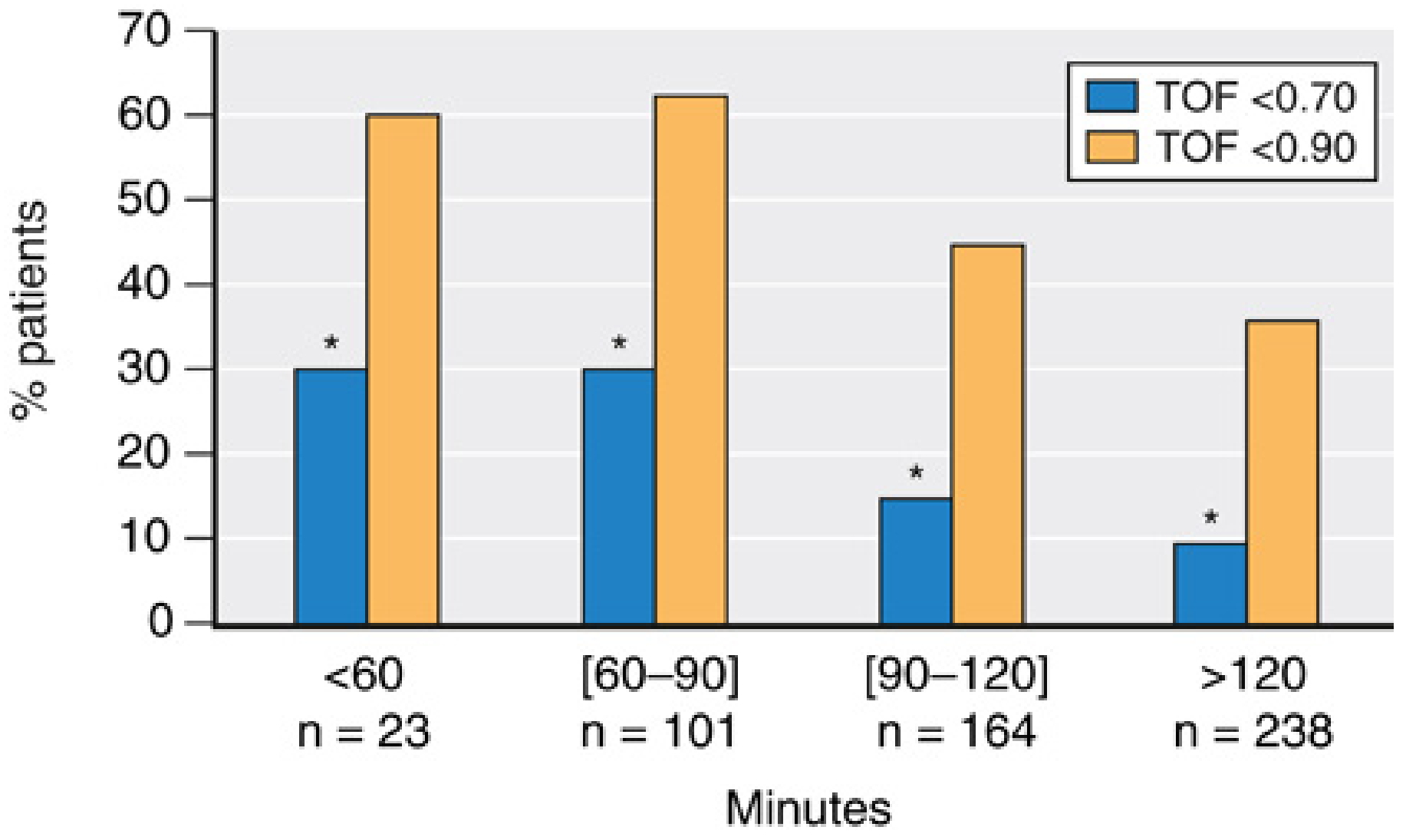
Figure: Even >120 minutes after a single intubating dose of rocuronium, vecuronium, or atracurium, ~35% of patients still have TOF ratio <0.90 and ~10% have TOF ratio <0.70. This demonstrates the unpredictability of spontaneous recovery and the need for monitoring.
- Miller's Anesthesia 10e, p.3403-3404
8. Guiding Reversal with Monitoring
Neostigmine (Anticholinesterase)
- Mechanism: inhibits acetylcholinesterase → increases ACh at NMJ → competes with NMBD
- Most effective when the block is minimal (TOF count of 4, ratio 0.4-0.9)
- Dose: 20-70 mcg/kg IV (combined with glycopyrrolate 10 mcg/kg or atropine to block muscarinic effects)
- Should NOT be given at deep block (TOF count 0-2) - cannot adequately reverse and may paradoxically worsen block (neostigmine weakness/overshoot)
- Onset: 5-10 minutes
- Duration: 60-120 minutes
Sugammadex (Selective Relaxant Binding Agent)
- Encapsulates steroidal NMBDs (rocuronium >> vecuronium)
- Dose depends on depth of block:
- Immediate reversal (no twitches, no PTC): 16 mg/kg
- Deep block (PTC ≥1, TOF count 0): 4 mg/kg
- Moderate block (TOF count 1-2): 2-4 mg/kg
- Shallow to minimal block (TOF count ≥2): 2 mg/kg
- Residual paralysis with sugammadex is much less common (~5%) vs neostigmine (~30-40%)
- Safe in patients with pseudocholinesterase deficiency (doesn't affect succinylcholine reversal)
- Barash, Clinical Anesthesia 9e, p.1725-1740
9. Adoption and Guidelines
Multiple national guidelines now recommend quantitative monitoring as standard practice:
- Canadian, French, Spanish, Australian, New Zealand, Czech, Portuguese, Japanese, and US guidelines all advocate for quantitative neuromuscular monitoring to guide dosing of NMBDs and their antagonists
- Guidelines recommend TOF ratio ≥0.9 (by quantitative monitor) before extubation
- If only a qualitative PNS is available and four twitches are present with no discernible fade, low-dose neostigmine (~20 mcg/kg) can be considered
- Barash, Clinical Anesthesia 9e, p.1626; Miller's Anesthesia 10e, p.3161
10. Practical Summary
| Clinical Goal | Monitoring Action |
|---|---|
| Confirm intubating conditions | TOF count 0 (or PTC = 0 for complete block) |
| Intraoperative deep block for surgery | TOF count 0, PTC 1-5 |
| Intraoperative moderate block | TOF count 1-3 |
| When to give neostigmine | TOF count 4 with minimal fade |
| When sugammadex is preferred | Any depth, especially deep block |
| Safe extubation criterion | TOF ratio ≥0.9 (quantitative) |
Recent Evidence (2024-2026)
Two recent systematic reviews confirm the ongoing burden of RNMB:
- Bijkerk et al. (Br J Anaesth, Feb 2025) found persistent residual neuromuscular block in the PACU remains common, reinforcing the case for routine quantitative monitoring. [PMID: 39443187]
- Alderman & Smith-Steinert (J Perianesth Nurs, Jun 2026) published an evidence-based summary on recognizing and treating postoperative residual paralysis. [PMID: 41460225]
Sources: Miller's Anesthesia 10e (Chapters 24, 39) | Barash, Cullen & Stoelting's Clinical Anesthesia 9e (Chapters 21) | Morgan & Mikhail's Clinical Anesthesiology 7e (Chapter 6)
This is a shared conversation. Sign in to Orris to start your own chat.